Amniotic Band Syndrome - A Dreaded Condition
Durga R1, T.K. Renukadevi2
1 Junior Resident, Department of Obstetrics & Gynaecology, ESI medical college & PGIMSR, KK Nagar, Chennai, India.
2 Professor and HOD, Department of Obstetrics & Gynaecology, ESI Medical College & PGIMSR, KK Nagar, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Durga. R, No 51/2, Sriram Nagar Third Main Road, Mugalivakkamroad, Porur, Chennai-600116, India. E-mail : jrs_durai@yahoo.co.in
Amniotic band syndrome is a unique condition in which amnion a normal structure causes complications. A case of second gravid, obese who is a known diabetic came to OPD at 13 weeks pregnancy for regular antenatal check up. A routine ultrasonogram was advised in which multiple anomalies were noted and the diagnosis of amniotic band syndrome was made. The parents were counseled for medical termination of pregnancy and after obtaining the consent termination were performed and the parents were asked to postpone the next pregnancy for minimum 6 months. This anomaly as seen in this patient could be due to risk factors like diabetes and obesity.
Abdominal wall defects, Amputation, Limb body wall complex, Vascular occlusion, Obesity, Hyperglycemia
Case Report
A 31-year-old obese G2P1L1 who is a known case of type 2 diabetes mellitus with previous healthy female child delivered by caesarian section presented in our hospital OPD at 13 weeks pregnancy with LMP:4/8/2013 and EDD:11/5/2014 for regular antenatal check up. She had previous dating scan at 5 weeks which showed regular gestational sac and dating scan corresponding to her menstrual age though her menstrual cycles were irregular. She had regular follow up with the diabetologist and her blood sugar was under control. She was advised nuchal translucency scan at 14 weeks.
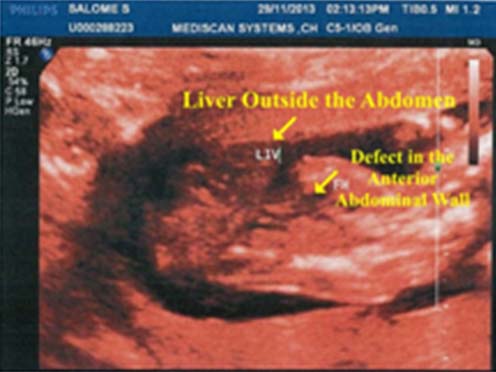
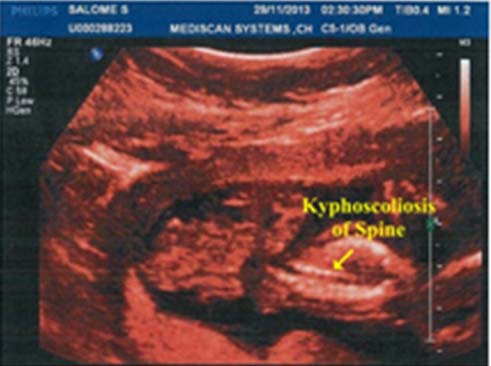
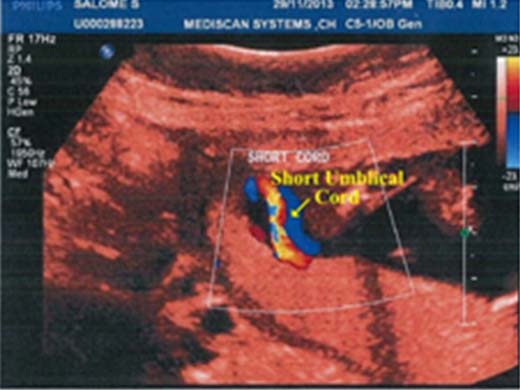
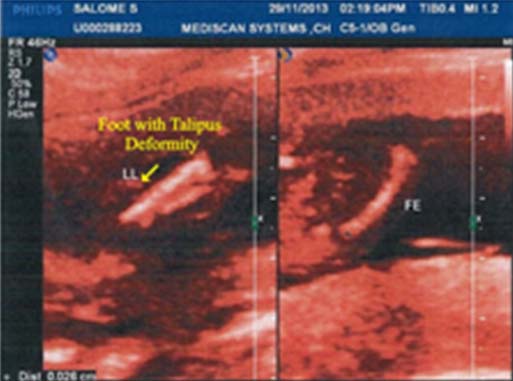
The ultrasonogram report in our hospital showed a single live intrauterine gestation of 14-15 weeks with cardiac activity well visualized. Anterior abdominal wall was not well appreciated in the present scan and abdominal circumference was reduced. Spine was not well visualized in lumbar and sacral region. Umblical cord was short. Few thin band like structures were noted in amniotic cavity. Hence, the most probable diagnosis of amniotic band syndrome was made. The patient was referred to mediscan to confirm the diagnosis which showed a single intrauterine gestation corresponding to 16 weeks. Large abdominal wall defect and entire abdominal contents were seen outside [Table/Fig-1]. Spine appeared deformed and irregular, Kyphoscoliosis was seen [Table/Fig-2]. Short umblical cord with single umblical artery was noted [Table/Fig-3]. One lower limb showed talipes deformity and other limb not visualized [Table/Fig-4]. Probable diagnosis of Amniotic band syndrome was made and they requested clinical correlation.
The parents were counseled about the anomalies of the baby and its incompatibility with life. After obtaining consent, Medical Termination of Pregnancy was performed using oral mifepristone tablet followed by tablet misoprostol per vaginally.
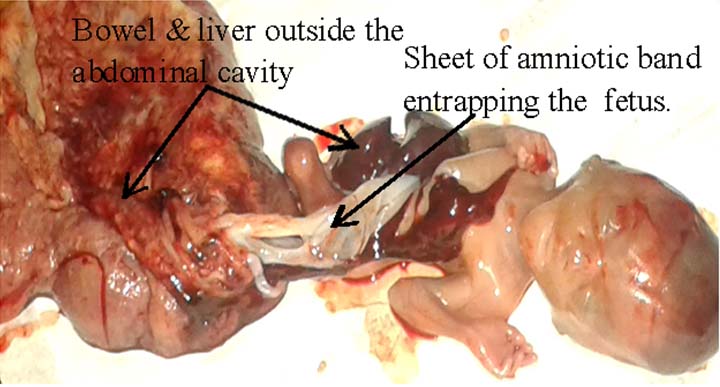
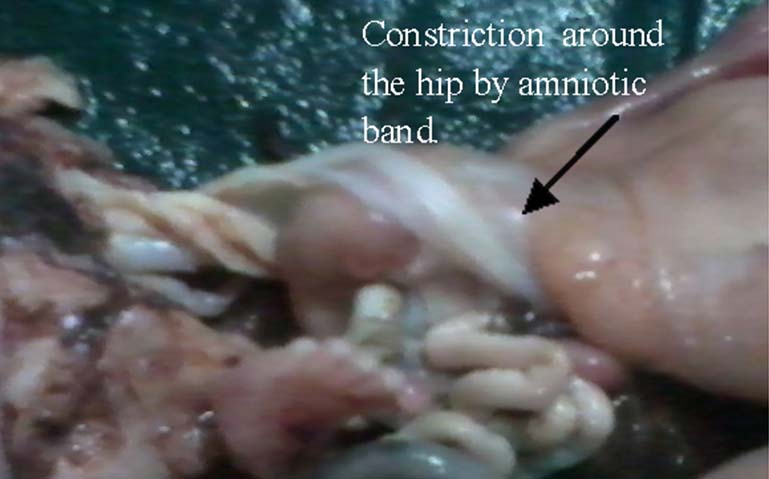
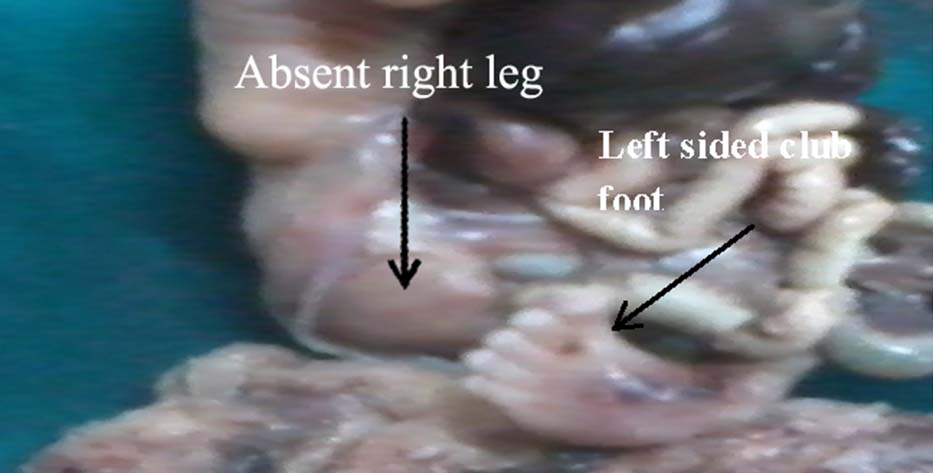
The terminated fetus showed sheet of amniotic band extending from the hip around the thorax. Right leg was absent due to constricting effect of the band & left leg club footed. Anterior abdominal wall defect with liver and bowel outside were observed. Umblical cord was short with single umblical artery. These anomalies were photographed [Table/Fig-5,6,7,8 and 9].

Amniotic band around hip.

The mother was counseled to postpone the next pregnancy atleast 6-8 weeks and she was started on folic acid tablets. She was advised to be on regular follow up. The patient is on regular follow up and doing well.
Discussion
Amniotic band syndrome is difficult to diagnose and the incidence of amniotic band syndrome vary widely from 1 in 1200 to 1 in 15000 live births and is responsible for 178 in 10,000 miscarriages [1].
Aetiopathogenesis
The pathogenesis of amniotic band syndrome is explained by two theories [1].
Intrinsic theory (Vascular theory): This may cause intrinsic defect in the blood circulation.
Extrinsic theory (Amniotic band theory): Suggests that birth defects which causes loss of amniotic fluid and extrusion of various organs.
Risk Factors
There are many studies which show many risk factors associated with this syndrome [2].
Inhabitants of high altitude. The hypoxic mechanism in the high altitude is associated with this syndrome.
The genetic origin of this syndrome has been reported.
First born with non cephalic presentation has increased incidence according to some studies.
Three cases were reported with the use of misoprostol.
Diabetes and Amniotic band syndrome: Vasculopathy seen in Diabetes adds on to the risk of vascular disruption seen in amniotic band syndrome as in this case.
Obesity and diabetes is possibly a cause of early amnion rupture.
Differential diagnoses: Neural tube defects, Omphalocele, Fanconi syndrome and Isolated lymphatic and vascular malformations.
Clinical features: The findings may be isolated defects including isolated facial defects, digital amputation, Kyphotic lardosis or scoliosis, club foot, extrachorionic haemorrhage, Large slash like defect of both thoracoabdominal cavity can occur with evisceration of viscera, Deformation of calvarium, if complete, the fetus may be anencephalic and if partial the fetus may appear to have an encephalocele. In limb body wall complex, there is a constellation of abnormalities thoracoabdominoschisis and limb defects and Umblical cord is usually absent or short as in this case [2–5].
Diagnostic investigations: The amniotic band syndrome is very difficult to diagnose and has a very poor outcome.
Ultrasonogram: These abnormalities are diagnosed at the end of first or second trimester. The deformities seen in ultrasound are:
Head/face entrapment: Acrania, anencephaly and facial clefts.
Truncal entrapment: Abdominal defects, rib clefting and congenital scoliosis.
Extremity entrapment: Variable levels of limb amputation, Variable levels of limb constriction, lymphoedema, pseudosyndactylity and phocomelia.
Colour Doppler should be done to differentiate this condition from lymphatic and vascular complications [6].
Management: A fetus with amniotic band syndrome should be delivered in a tertiary care center where neonatologists, pediatric surgeons and orthopedicians are available. Treatment depends on nature of amniotic band syndrome and the severity of deformation.
In case of mild limb constriction, constriction band is released using Z-plasty where the surgeon makes incisions along the band and removes fragile skin that went into the creases. Then zigzag incisions are made to obtain the pointed flaps which are sutured to obtain normal contour.
In case of severe bony abnormalities, realignment surgeries are recommended.
In severe anomaly affecting the abdominal wall and visceras which is life threatening as in this case termination of pregnancy is recommended [1,2].
Conclusion
Thus, amnion which is a protective structure of the fetus becomes destructive in this syndrome. Hence, this syndrome though rare should be kept in mind during first trimester scanning. Moreover, in this case there are risk factors for the various anomalies like obesity and diabetes mellitus which increases the risk in addition to the mechanical effects of amniotic bands.
[1]. en.Wikipedia.org [internet]. Wikipedia foundation inc, [updated 2015 July 12 ]. Available from: http://en.wikipedia.org/wiki/Amniotic_Band_Syndrome [Google Scholar]
[2]. Cignini P, Georlandino C, Padula F, Dugo N, Cafa EV, Spata A, Epidemiology and risk factors of amniotic band syndrome, or ADAM sequenceJ Prenat Med 2012 6(4):59-63. [Google Scholar]
[3]. Furdon SA, Donlon CR, Examination of the newborn foot: positional and structural abnormalitiesAdvances in Neonatal Care 2002 2(5):248-58. [Google Scholar]
[4]. McGuirk CK, Westgate MN, Holmes LB, Limb deficiencies in newborn infantsPediatrics 2001 108(4):e64 [Google Scholar]
[5]. Jabor NA, Cronin ED, Bilateral Cleft Lip and Palate and Limb Deformities: A Presentation of Amniotic Band Sequence?Journal of Craniofacial Surgery 2000 11(4):388-93. [Google Scholar]
[6]. Nardozza LM, Araujo Júnior E, Caetano AC, Moron AF, Prenatal Diagnosis of Amniotic band syndrome in the third trimester of pregnancy using 3D ultrasoundJ Clin imaging Sci 2012 2:22 [Google Scholar]