The objective of endodontic treatment is the elimination of microscopic organisms from the root canal system and the subsequent establishment of an effective barrier to avert further entry of microorganisms or their items to the periapical tissues [1].
Conventional endodontic treatment has been indicated to be effective in around 90% of cases. If endodontic therapy fails then retreatment is indicated. In the event that this is impractical or if retreatment fails, periapical surgery may be needed. Periapical surgery comprises of one, or a combination of, simple curettage of infected or inflamed tissue, removal of an infected or damaged root apex or a retrograde filling to avoid correspondence between the root canal system and the periapical tissues. Most examinations concerning retrograde fillings have concentrated either on the biocompatibility of the retrograde filling material or assessing apical microleakage. There are possibly two avenues by which leakage can happen at the apex of a root sealed with a retrograde filling. The principal is by apical microleakage i.e. is leakage along the interface between the filling material and the canal wall. The second route is by the flow of fluids and substances along open tubules at the resected root end, that is, via permeable apical dentin. The total of the leakage along these two pathways may be termed "apical leakage" [1].
Many materials have been proposed for utilization in retrograde fillings such as silver amalgam, gutta-percha, calcium hydroxide based cements, zinc oxide and eugenol, mineral trioxide aggregate, resins, glass ionomer cement, I.R.M, Portland cement [2–5]. This new proliferation of materials raised questions about their utilization, principally on the grounds that as of recently a perfect material that exhibits satisfactory physical-chemical and biological properties, for example, simplicity of manipulation, dimensional stability, non toxicity, radiopacity, non resorbability, not being influenced by the vicinity of dampness and capacity to empower the repair of apical tissue, has not been accounted for in the literature [6]. In recent years, the most commonly used root end filling materials have been glass ionomer cement, IRM and MTA. Although many studies have investigated microleakage of various root end materials separately, very few have examined the influence of the apical bevel and its relationship to apical dentin permeability of various retrograde filling materials [1,5].
Hence the present invitro study is undertaken to evaluate the root end sealing ability of four different retrograde filling materials in teeth with root apices resected at different angles using a fluorescent dye-penetration method.
Materials and Methods
The study was conducted in Department Conservative Dentistry and Endodontics, Pacific Dental College Udaipur in year 2011. A total of 110 single rooted human maxillary anterior teeth were ultrasonically cleaned, disinfected and stored in normal saline. Only 100 permanent teeth [Table/Fig-1] with intact root and without caries were selected. Teeth with calcification, fractured root and with multiple canals were excluded. The teeth were decoronated at the cementoenamel junction and the samples were standardized to a length of 15 mm using a diamond disc. Root canal preparation was carried out in all the teeth by conventional technique using 5.25% sodium hypochlorite as irrigating solution with hand instrumentation (K–files). The apical portion of the canal was prepared with a No. 40 K-file and rest of the canal was flared using conventional step back technique (upto No. 60 K-file).
Sample division into two groups.
| Group A- the root apices resected at 0° to the long axis of the root (50) | Group B- the root apices resected at 45° to the long axis of the root (50) |
|---|
| Subgroup A1 (ProRoot MTA), n=10 | Subgroup B1 (ProRoot MTA), n=10 |
| Subgroup A2 (Portland Cement) n=10 | Subgroup B2 (Portland Cement) n=10 |
| Subgroup A3 (IRM) n=10 | Subgroup B3 (IRM) n=10 |
| Subgroup A4 (GIC Ketac N-100) n=10 | Subgroup B4 (GIC Ketac N-100) n=10 |
| Subgroup A5 (Positive Control) n=5 | Subgroup B5 (Positive Control) n=5 |
| Subgroup A6 (Negative Control) n=5 | Subgroup B6 (Negative Control) n=5 |
The cleaned and shaped canals were dried with paper points and obturated with gutta percha using lateral condensation technique and AH-Plus (DentsPly, Mailleffer) as root canal sealer. Access cavity was sealed with MD-TEMP white (MetaBiomed Co Ltd, Korea). The roots were then stored at room temperature under 100% humidity for one week.
The root resection were carried out by removing 2 mm in group A and 1 mm in group B using diamond disc under constant irrigation with sodium chloride solution. A 3mm deep root end cavity was prepared using no. #8 round bur with slow speed contra angle hand piece. Depth of the root end cavity was checked using periodontal probe. The teeth were then coated with two layers of nail varnish except the tip where the retrograde root filling material was placed.
Each material was condensed into the prepared cavity using small pluggers.
In addition, within both the groups, five teeth with retro preparation received no filling (subgroup A5 and B5) and served as a positive control while five teeth that were instrumented and obturated were completely covered with nail varnish (subgroup A6 and B6) and served as negative control.
All roots were exposed to an aqueous solution of a fluorescent dye (Acrydine Orange) for 24 hours, longitudinally sectioned and then the extent of dye penetration was measured using a fluorescent microscope.
Scoring for dye penetration for apical microleakage [
7]
0 No dye penetration.
1 Dye penetration into apical one third of retrograde filling material.
2 Dye penetration into apical middle third of retrograde filling material.
3 Dye penetration into full length of retrograde filling material.
4 Dye penetration beyond retrograde filling material.
The statistical analysis was done using ANOVA [Table/Fig-2&4], to test for any significance. MTA showed the statistically significant difference in microleakage, when compared to Portland cement, IRM and LC-GIC. Portland cement showed statistically significant difference with IRM, but not a statistically significant difference with LC-GIC. IRM showed statistically significant difference with LC-GIC. No significant difference was obtained when all four materials were compared at both angles individually by Post-hoc test [Table/Fig-3&5].
Mean value of dye penetration between materials at 0° angle (ANOVA).
| Material | No. of sample | Mean (SD) | F value | p value |
|---|
| M.T.A. | 10 | .30 (.483) | 13.697 | .000* |
| Portland Cement | 10 | 1.10 (.568) |
| I.R.M. | 10 | 2.40 (.843) |
| RMG.I.C. | 10 | 1.30 (.966) |
*Significant (p<0.05)
Pair wise comparison between materials at 0° angle (Post hoc Test).
| MATERIAL | MATERIAL | MEAN DIFFERENCE | S.E. | p value |
|---|
| M.T.A. | PORTLAND CEMENT | .80 | .332 | .021* |
| I.R.M. | 2.10 | .332 | .000* |
| RMG.I.C. | 1.10 | .332 | .002* |
| PORTLAND CEMENT | M.T.A. | .80 | .332 | .021* |
| I.R.M. | 1.30 | .332 | .000* |
| RMG.I.C. | .30 | .332 | .372 |
| I.R.M. | M.T.A. | 2.10 | .332 | .000* |
| PORTLAND CEMENT | 1.30 | .332 | .000* |
| RMG.I.C. | 1.00 | .332 | .005* |
| RMG.I.C. | M.T.A. | 1.10 | .332 | .002* |
| PORTLAND CEMENT | .30 | .332 | .372 |
| I.R.M. | 1.00 | .332 | .005* |
*Significant (p<0.05)
Mean value of dye penetration between between MTA, Portland Cement, IRM & LC-GIC at 45° angle (ANOVA).
| Material | No. of sample | Mean (SD) | F value | p value |
|---|
| M.T.A. | 10 | .40 (.516) | 9.516 | .000* |
| Portland Cement | 10 | 1.40 (.843) |
| I.R.M. | 10 | 2.40 (.966) |
| RMG.I.C. | 10 | 1.60 (.966) |
*Significant (p<0.05)
Pair wise comparison between MTA, Portland Cement, IRM & LC-GIC at 45°angle (Post hoc Test).
| Material (1) | Material (2) | Mean difference | S.E. | p value |
|---|
| M.T.A. | Portland Cement | 1.00 | .377 | .012* |
| I.R.M. | 2.00 | .377 | .000* |
| RMG.I.C. | 1.20 | .377 | .003* |
| Portland Cement | M.T.A. | 1.00 | .377 | .012* |
| I.R.M. | 1.00 | .377 | .012* |
| RMG.I.C. | .20 | .377 | .599 |
| I.R.M. | M.T.A. | 2.00 | .377 | .000* |
| Portland Cement | 1.00 | .377 | .012* |
| RMG.I.C. | .80 | .377 | .041* |
| RMG.I.C. | M.T.A. | 1.20 | .377 | .003* |
| Portland Cement | .20 | .377 | .599 |
| I.R.M. | .80 | .377 | .041* |
*Significant (p<0.05)
Discussion
Most of the tribulations in endodontics are resolved using conventional treatment approach. However, in certain conditions such as, large periapical lesions, separated instruments in the canals, apical variations, improper obturations, calcified canals and dilacerated roots etc., surgical intervention may be necessary [8–10].
The biocompatibility of dental materials is one of the most important and most studied factors in endodontic surgery, but the “fluid-tight” sealing of the canal is no less important for the success of root canal fillings [11]. Failure of apical surgery can generally be attributed to poor marginal sealing of the root ends, characterized by inadequate contact between the filling material and the tooth surface [12]. Apical sealing should prevent leakage of interstitial fluid into the root canal, as such fluid may carry microorganisms into the canal. Apicoectomy and retrograde preparations increase the chances for leakage of the remaining root, reinforcing the need for retrofilling [13]. After the basic steps of endodontic surgery, often root end preparation is advocated and a suitable root end filling material is inserted.
Hence, the aim of placing a root-end filling material is to develop a “fluid-tight” apical seal which inhibits the leakage of residual irritants from the root canal into the periradicular tissue and vice versa [14]. Numerous materials have been used as root end restoratives, but none of them fulfill the ideal properties of the root end filling material [8].
Newer materials like Mineral Trioxide Aggregate (MTA), calcium phosphate and bone cement are also frequently used for root-end filling. Various alternatives to amalgam have been advocated, amongst which GIC, IRM and MTA are the materials which have shown promising results in numerous studies [15].
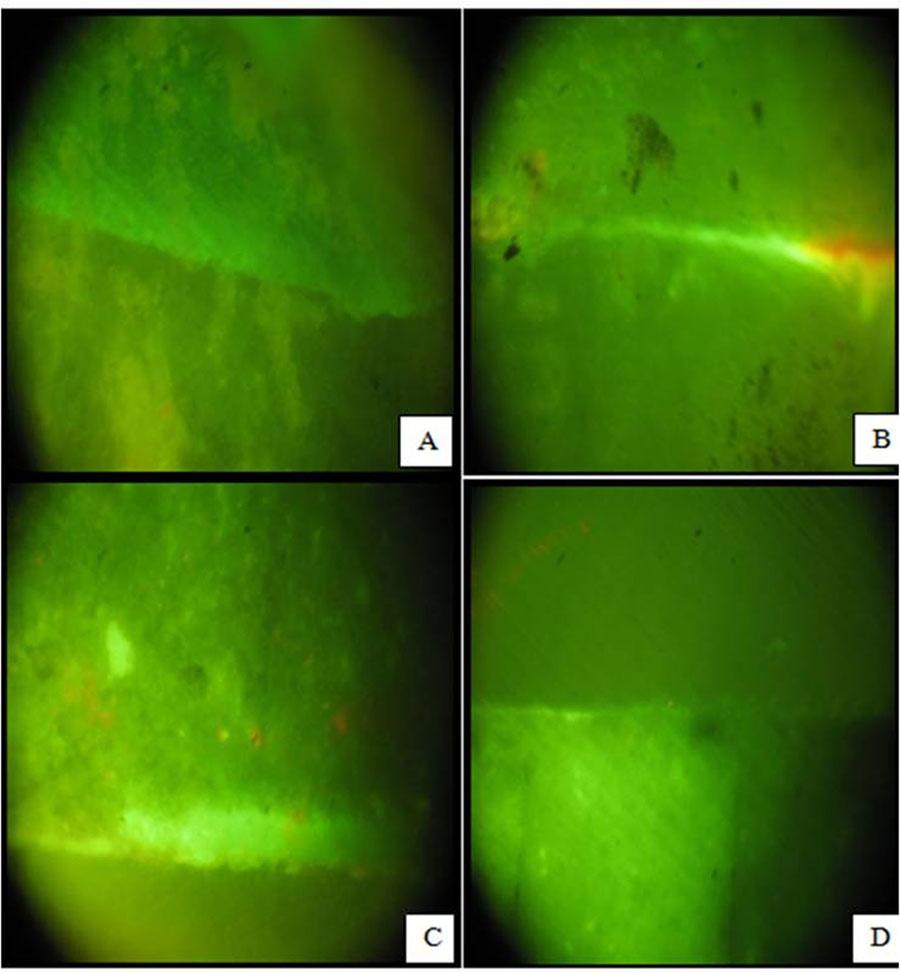
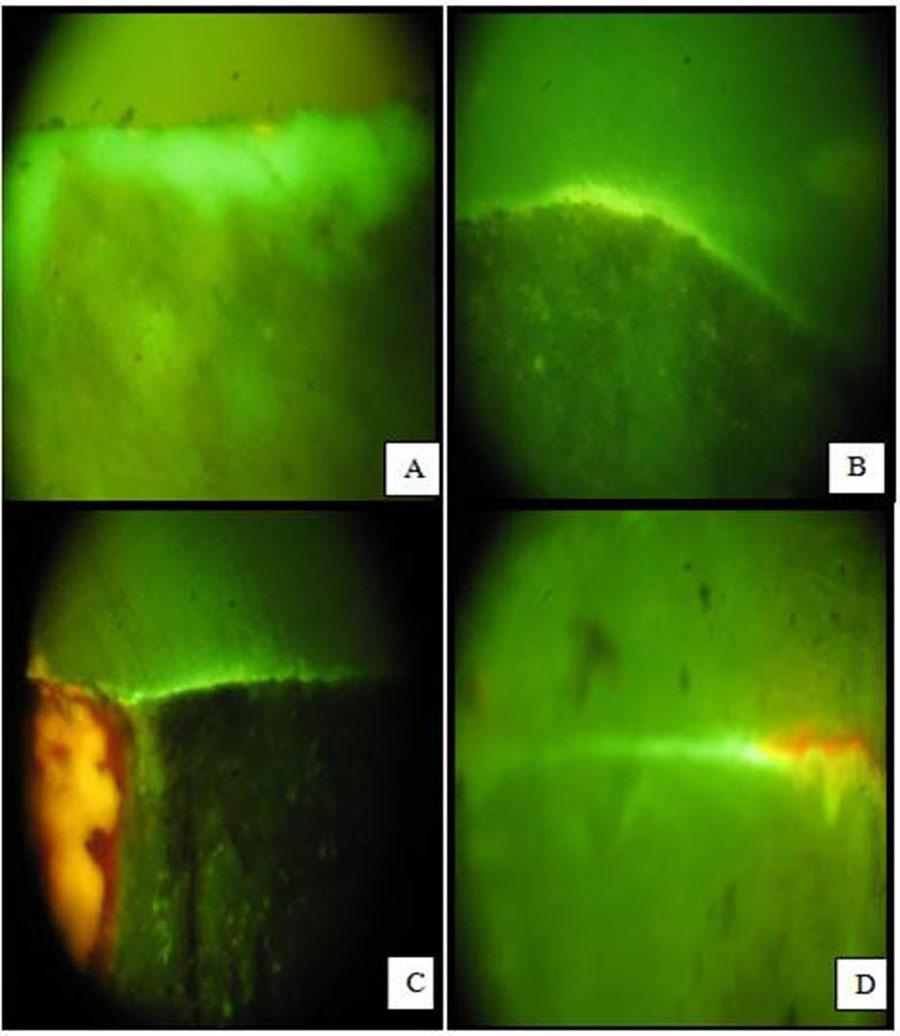
As a component of clinical protocol different angles have been used to section the apical root during apicoectomies. Traditionally, a 45° root end bevel was utilized. A 45° bevel is considered a reliable option to facilitate the material insertion, and is demonstrated when access is restricted in the operating field [16]. However, incremented leakage has been reported when a 45° root end bevel was utilized. Incremented leakage is primarily due to leakage through permeable apical dentin since a resection angle of 45° exposes many more dentinal tubules than a flat 0° cut. Thus, it has been proposed that the perfect edge of resection is flat (0°) since it minimizes apical leakage [1]. Root end cavity can be prepared by a bur or an ultrasonic instrument. The researches have demonstrated that ultrasonic instruments create more micro fractures than burs during root end cavity preparations [1] [Table/Fig-6a-d, 7a-d].
A. MTA Dye Leakage At 0° B. MTA Dye Leakage At 45° C. Portland cement Dye Leakage At 0° D. Portland cement Dye Leakage At 45°
A. IRM Dye Leakage At 0° B. IRM Dye Leakage At 45° C. LC GIC Dye Leakage At 0° D. LC GIC Dye Leakage At 45°
Group A- The root apices resected at 0° to the long axis of the root.
MTA (A1) showed the least microleakage [Table/Fig-6a] compared to all other groups i.e. IRM [Table/Fig-7a], Portland cement [Table/Fig-6c], and GIC [Table/Fig-7c]. The results of this study are also concurrent with the study done by Torabinejad et al., which showed that MTA had the least apical microleakage compared with IRM and super EBA [15]. Wu et al., revealed that both GIC and MTA showed less micro leakage than silver amalgam and super-EBA cement [17]. The results observed by Hong et al., are not concomitant with the results of the present study [18]. Hong et al., did not observe any significant difference in the maximum pore diameter of MTA and Portland cement between the measurements at 90 minutes and 48 hours [18]. This may be due to the difference in irregularities and particle size of Portland cement.
MTA gave better result because the principal ions of dental hard tissues i.e. calcium and phosphorus are the main ions present in this material. Hence, MTA is highly biocompatible when used in contact with cells and tissues. MTA also induces hard tissue barrier, this would minimize interaction between material and host tissues [19].
After placement of MTA in root canals and its continuous disintegration, hydroxyapatite crystals nucleate and develop, filling the spaces in the between MTA and the dentinal wall. At first the seal is mechanical, however with time, because of dissemination of particles, a chemical bond happens [20]. Consequently MTA tends to give better results where the issue of microleakage is concerned.
Group B- The root apices resected at 45° to the long axis of the root.
MTA (Group B1) showed the least microleakage [Table/Fig-6b] compared to all other groups i.e. Portland cement [Table/Fig-6d], IRM [Table/Fig-7b] and GIC [Table/Fig-7d]. The results of this study are also concurrent with the study done by Torabinejad et al., and Wu et al. Torabinejad et al., reported that MTA showed the least apical microleakage compared with IRM and Super EBA [15]. Wu et al., revealed that both GIC and MTA showed less micro leakage than amalgam and super-EBA cement [18]. Clinically resecting the apex at 0° may be more difficult and might require removal of normal bone to achieve the same. So placing a 45° angle might help in achieving the same result as that with a 0° angle, with lesser removal of bone.
Comparison of micro-leakage within the sub-groups at two angles (0° and 45°): Comparison of micro-leakage within the sub-group (A1 & B1) showed that there was no statistically significant difference in any material when compared in between the two angles. Results of the present study are not in concurrence with the results of the study by Gilheany et al., who showed that increasing the depth of the retrograde filling significantly decreased apical leakage and that there was a significant increase in apical leakage as the amount of the bevel increased [1].
It is reasonable to infer that the increased leakage was primarily due to leakage through permeable apical dentin since a resection angle of 45° exposes many more dentinal tubules than a flat, 0° cut.
The positive control groups (A5 & B5) showed maximum dye leakage. The negative control group (A6 & B6) showed no leakage at all.
In the present study, there was no statistically significant difference in any material when compared in between the two angles. Correlation of the information acquired from different leakage studies shows significant variety when associated with the after effects of the present study and examination of clinical studies shows that there are many variables in these investigations. The main variables include: the number of cases, materials tested, distinctive sort of dyes, absence of standardization or assessment criteria for quantitative results got in these studies. Because of these variables it is difficult to compare the results with one another.
In the present study, least microleakage was seen in MTA which can be owed to its property of having excellent marginal adaptation and sealing ability. MTA shows absorbtion of dihydrogen monoxide during hydration of the powder leading to expansion during setting which may be the reason for its excellent sealing ability [21]. Another fascinating component is the arrangement of cementum and periodontal ligament strands contiguous to MTA.
IRM when contrasted with MTA indicated fundamentally more leakage. The findings in the study are in accordance with an in vitro study done by Sel uk Erkut. This can be attributed to the fact that IRM, a zinc oxide eugenol cement reinforced by 20% polymethylmethacrylate by weight reinforces the cement and as a result it eliminates the quandary of absorbability and decreases disintegration of cement leading to better adaptation to the cavity walls [22]. The placement techniques for these materials require watchful planning of dentin surface and their application in a dry field. Contamination of apical preparation and/or disruption of the setting reaction with dampness before it has come to finish could bring about significant leakage for light cure glass ionomer concrete bonds with the dentin in a surgical field [15]. Thus, co-ordinate use of this method and extrapolation of these outcomes to invivo circumstances requires further studies. There may be constrained access in a surgical field to light curing of the material with a standard light guide; along these lines a smaller light guide required for this reason should be produced.
Most model systems used for measuring microleakage and dentin permeability do not completely reproduce the in vivo environment. It is not known whether or not the factors evaluated here may alter the success rate of clinical treatment; however, since the treatment goal is to minimize the possibility of bacteria and their metabolites exiting the root canal system and gaining entry to the periapical tissues, any factor which may improve the seal between the canal and the periapical tissues should be utilized. Finally, when measured in vitro, the porousness of the resected apical dentin and microleakage around the retrograde filling material both has a noteworthy impact on apical leakage [1].
Conclusion
Microleakage was observed in all the sub groups. MTA recorded the least apical leakage value while IRM recorded the maximum apical leakage value among all the materials. On comparison between the apical microleakage values, MTA and IRM showed statistically significant difference from all the materials, whereas difference in the sealing ability of Portland cement and RMGIC was not statistically significant. There was no statistically significant difference among all the materials at 0° and 45° angle.
*Significant (p<0.05)
*Significant (p<0.05)
*Significant (p<0.05)
*Significant (p<0.05)