Parameatal Urethral Cyst in a Newborn–A Case Report and Review of the Literature
Christos Kaselas1, Ioannis Spyridakis2, Dimitrios Patoulias3, Paschalis Tsioulas4, Ioannis Patoulias5
1 Pediatric Surgery Department, “Aristotle” University Medical School, “G. Gennimatas” General and University Hospital, Thessaloniki, Greece.
2 Ioannis Spyridakis, 2nd Pediatric Surgery Department, & quot; Aristotle & quot; University Medical School, & quot; G. Papageorgiou & quot; General and University Hospital, Thessaloniki, Greece.
3 Dimitrios Patoulias, 1st Pediatric Surgery Department, & quot; Aristotle & quot; University Medical School, & quot; G. Gennimatas & quot; General and University Hospital, Thessaloniki, Greece.
4 Paschalis Tsioulas, 2nd Pediatric Surgery Department, & quot; Aristotle & quot; University Medical School, & quot; G. Papageorgiou & quot; General and University Hospital, Thessaloniki, Greece.
5 Ioannis Patoulias, 1st Pediatric Surgery Department, & quot; Aristotle & quot; University Medical School, & quot; G. Gennimatas & quot; General and University Hospital, Thessaloniki, Greece.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR:Dr. Christos Kaselas, Department of Pediatric Surgery, “G. Gennimatas” General and University Hospital, 41 Ethnikis Amynis str, 54635, Thessaloniki, Greece.
E-mail: xkaselas@otenet.gr
Parameatal urethral cysts are rare congenital lesions of the penis that are usually <1cm in diameter in the paediatric population and do not create any urinary difficulties. Their natural course is either to resolve or to be surgically excised without any postoperative complications. We report a case of a newborn with a parameatal urethral cyst that produced voiding difficulties and was treated by surgical excision.
Cyst, Glans penis, Penile diseases, Urogenital abnormality, Urethral diseases
Case Report
A male newborn, 7 days of age, was referred to our department from a primary care paediatrician because on his 3rd day of life he developed a penile cyst on the urethral meatus with a ventrolateral location that seemed to increase in size. In the paediatrician’s report it was stated that although the newborn was healthy, he seemed to develop a gradually increasing discomfort prior to voiding, and that voiding itself had a long duration, thin line and increased distance of micturition. The patient was an otherwise healthy male newborn, the second child of a healthy mother, who was born at 38 weeks of gestation with caesarean section and birth weight 2830 gram. Prenatal and perinatal history was normal, free of any pathological findings. He was feeding normally and gained weight appropriately for his age.
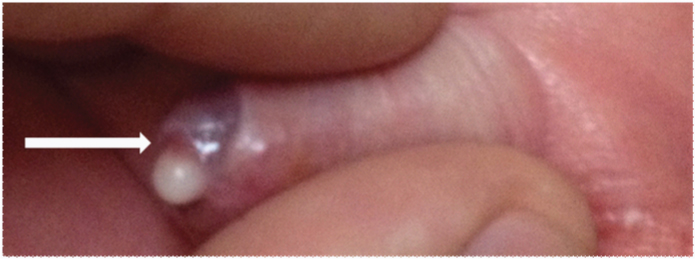
At arrival the child was healthy without any signs of discomfort. Physical examination was normal apart from the penile cyst [Table/Fig-1]. At initial observation, the cyst gave the impression to be filled with a milky substance, mimicking either a smegma pearl or an inflamed cyst with purulent content. It was located on the ventral and lateral surface of the urethral meatus, with distinct boundaries from the urethral mucosa and partially occluding the meatus due to its side [Table/Fig-2]. An inflamed purulent cyst was excluded as the infant did not show any topical or systematic signs of inflammation. A possible smegma pearl was also excluded.
The parameatal urethral cyst

Lateral view of the glans. Note how the cyst partly covers the meatus. Only the posterior meatus is free (arrow)
After examination was completed, the child started crying and showed signs of irritation and discomfort. The mother explained that he starts that kind of behaviour just before urination. So, we advised her to open the diapers so that we can see how he urinates. We noticed that the diapers were not at all wet although they were changed by the mother before they started their way to the hospital-the family leaves in a town almost two hours’ drive away. Finally, we managed to confirm the paediatrician’s description of the child’s micturition and decided to hospitalize him for further investigation.
Full blood count and C-reactive protein (CRP) measurement and also urinalysis were normal. An ultrasound evaluation of the upper and lower urinary system was scheduled in fear of a possible obstructive pattern of urination that could affect the rest of the urinary tract without any pathological findings.
We decided that the best approach for the management of the patient’s pathology was surgical excision of the cyst. The cyst was excised “en bloc” without any intraoperative problems. The postoperative period was normal, the child started urinating without any discomfort and with a normal pattern and was discharged home.
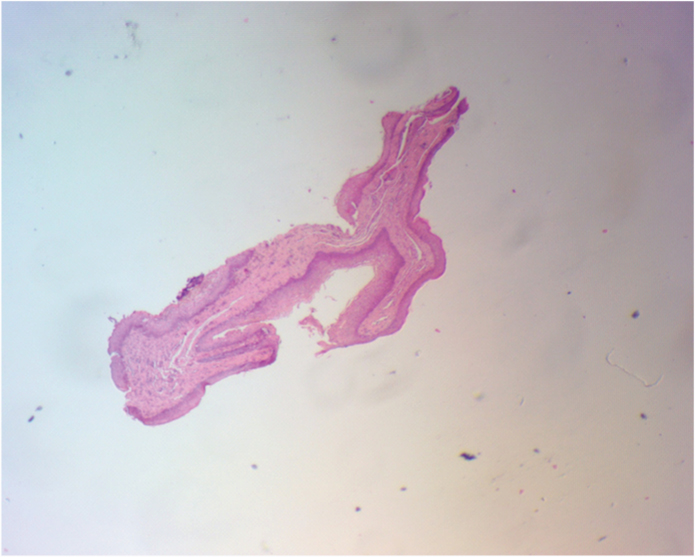
The histopathological report described a cystic lesion 0.2cm in diameter with a squamous epithelial lining indicating a median raphe cyst [Table/Fig-3]. Three months later, follow up is free of any complications and a postoperative ultrasound re-evaluation is normal. In lieu of a formal ethics committee, the principles of the Helsinki Declaration were followed.
Histopathological microphotograph of the excised cyst
Discussion
Parameatal urethral cysts are rare benign congenital lesions of the penis. Since the first description by Lantin and Thompson in 1956, no more than 50 cases have been described in the literature, both for adults and children [1–3]. In the paediatric population they are even rarer and can present at any age, from infancy to adulthood. Although the cysts may be recognized in infancy, usually they manifest after the first year of life. Patients however, present seeking treatment in their early to late childhood but also during the pre-pubertal period [4–6].
They are considered to be part of the median raphe cysts family that extend and can present at any point along the ventral raphe of the penis [7,8]. In the paediatric population they usually follow an asymptomatic course. The management is conservative with reassurance of the parents that the cyst will probably resolve and for its benign nature [4,5].
However the location of the cyst on the penis creates an increased disruption to parents that needs to be dealt with respect and consistency [4]. Another issue is whether the location of the cyst produces voiding problems, deflection of urinary stream or obstructive phenomena during urination [5]. This is almost never encountered if the cyst is discovered in the neonatal period but there have been cases in older patients that they complained for such symptoms [4,5,7]. Surgical management is selected in cases that the cyst does not resolve and usually during childhood or adolescence when it creates symptoms or for cosmetic reasons [4,7,9].
The cysts do not usually exceed 1cm in diameter in children and 2 cm in adult patients. The epithelium of the cyst can be transitional, cuboidal, columnar and squamous or a combination of epithelial types [4–7,9]. The aetiology of the cysts is unclear and several theories exist. It is thought that their existence is either due to persistence of cystic spaces during preputial delamination, or anomalous fusion of the urethra during organogenesis or are caused by obstruction of the paraurethral ducts [4,7,8].
This case is exceptional from the anticipated pattern of presentation of this rare condition. In our case, the cyst is found in a newborn-during its first week of life, with a tendency to increase in size creating voiding problems, mainly in the pattern of micturition and not obstructive phenomena as proven after ultrasound evaluation. The histopathological examination reported that the lining of the cyst was by squamous lining. Based on that finding and the very young age we tend to accept the theory that probably the cyst is created due to a late event during urethral fusion. However its tendency to increase in diameter could be attributed to obstruction of the paraurethral ducts. A combination of more than one pathogenetic mechanism cannot be excluded.
Conclusion
The management of paraurethral meatal cysts should be conservative in cases that it remains asymptomatic. However, close observation is essential as the cyst may increase in size and/or create voiding difficulties or other symptomatology. In these cases a thorough evaluation of the urinary tract is mandatory to evaluate for obstructive phenomena and surgical excision should be selected.
Conflict of interest
None of the contributing authors have any conflict of interest, including specific financial interests or relationships and affiliations relevant to the subject matter or materials discussed in the manuscript.
[1]. Lal S, Agarwal A, Parameatal cyst: A presentation of rare case and review of literatureJ Clin Diagn Res 2013 7:1757-58. [Google Scholar]
[2]. Nerli RB, Shivangouda P, Hiremath MB, Parameatal urethral cyst presenting with painful intercourseMed Surg Urol 2012 1:104 [Google Scholar]
[3]. Lantin PM, Thompson IM, Parameatal cysts of the glans penisJ Urol 1956 76:753-55. [Google Scholar]
[4]. Willis HL, Snow BW, Cartwright PC, Wallis MC, Oottamasathien S, deVries C, Parameatal urethral cysts in prepubertal malesJ Urol 2011 185:1042-45. [Google Scholar]
[5]. Onaran M, Tan MO, Camtosun A, Irkilata L, Erdem O, Bozkirli I, Parameatal cyst of urethra: A rare congenital anomalyInt Urol Nephrol 2006 38:273-74. [Google Scholar]
[6]. Lorette G, Machet MC, Maruani A, Parameatal cyst in a 4-year-old boyEur J Paediatr 2013 172:1701 [Google Scholar]
[7]. Shao IH, Chen TD, Shao HT, Chen HW, Male median raphe cysts: serial retrospective analysis and histopathological classificationDiagnostic Pathology 2012 7:121-25. [Google Scholar]
[8]. Otsuka T, Ueda Y, Terauchi M, Kinoshita Y, Median raphe (parameatal) cysts of the penisJ Urol 1998 159:1918-20. [Google Scholar]
[9]. Sinha AK, Kumar B, Kumar A, Singh MK, Kumar P, Congenital parameatal urethral cyst in male: A case report and review of literatureJ Ped Surg Case Reports 2015 3:267-68. [Google Scholar]