Non Infiltrating Angiolipoma of the Palate in Geriatric Patient: A Case Report with Review of Literature
Deepak Chandrasekaran1, Ravindran Chinnaswami2, Malathi Narasimhan3, Annie Evangelin Nithia Kumar4, Parthasarathy Natarajan5
1 Senior Lecturer, Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
2 Professor and HOD, Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
3 Professor and HOD, Department of Oral and Maxillofacial Pathology, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
4 Post Graduate Student, Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
5 Reader, Department of Prosthodontics, Crown and Bridge, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Chandrasekaran, 1/306, Saraswathy Street, Sri Ranga Nagar, Baai Kahadai, Moulivakkam, Chennai-125, India.
E-mail: deepakvinoth@gmail.com
Angiolipoma is one of the rare variant of lipoma. This benign tumour consists of both fatty and vascular elements. It mostly occur in the trunk and extremities and is uncommon in head and neck region. Angiolipoma is classified as infiltrating and non- infiltrating types. Among all neoplasms of the oral cavity, lipomas account for 1 to 5% and the incidence of angiolipoma is 5 to 17% in it. There is no sex predilection for this tumour. It is classified as infiltrative and non-infiltrative type. Surgical excision is the method to be considered for both the types of angiolipoma, however the infiltrating type recurs post-surgery. We report a rare case report of 55-year-old female with non-infiltrating angiolipoma of the hard palate mimicking a mucocele treated by surgical excision with no signs of recurrence and good wound healing after three months follow up with minimal scar formation.
Angiolipomatosis, Benign neoplasm, Soft tissue neoplasm
Case Report
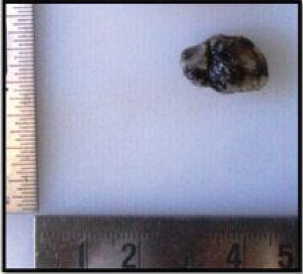
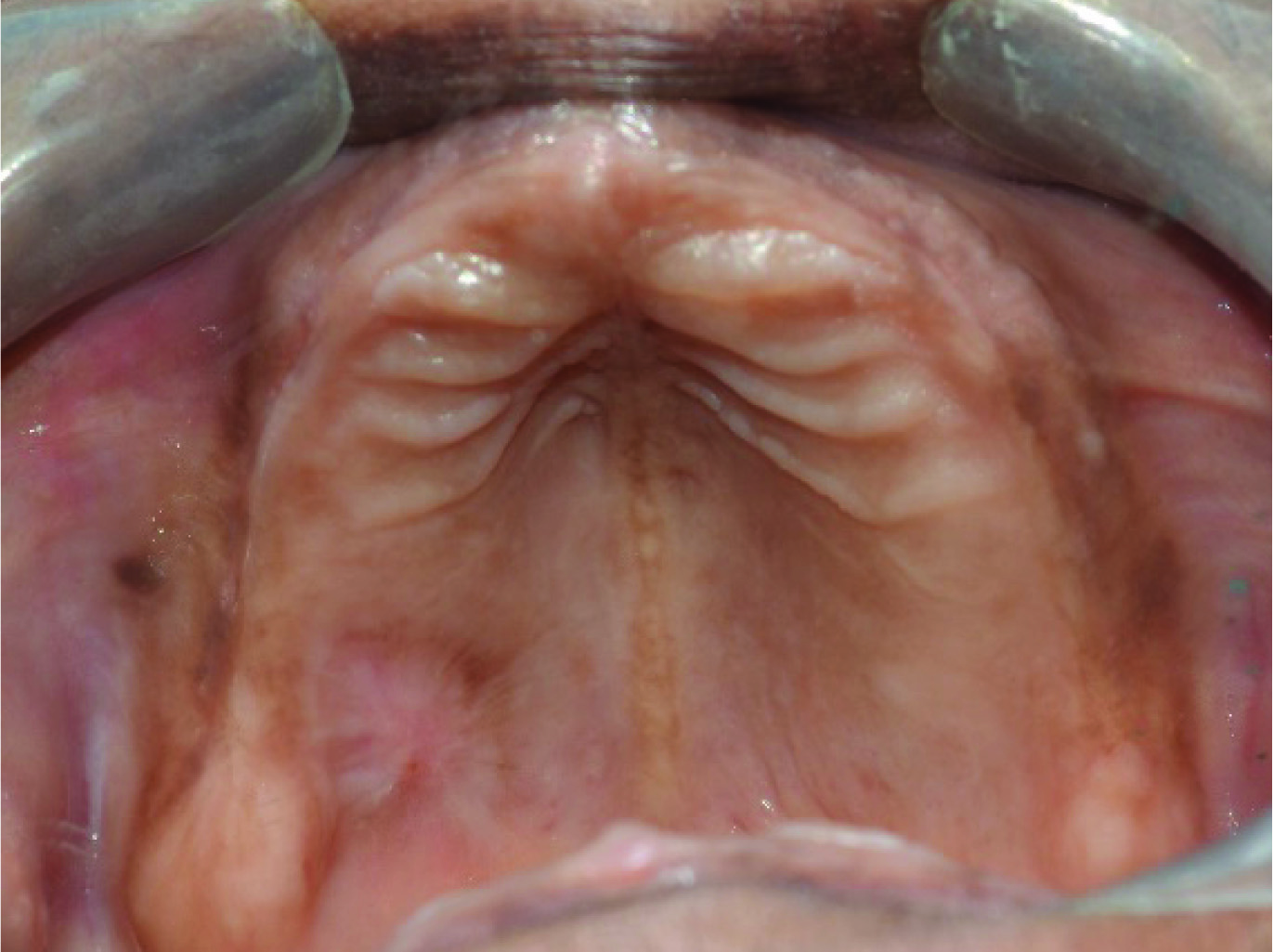
A 55-year-old Indian female reported to the Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University in 2015 with a complaint of a swelling on the right side of the palate for the past one month [Table/Fig-1]. Patient revealed a medical history of Type one diabetes mellitus under control with oral hypoglycaemics (Tab Metformin 500 BID and Tab. Glyciphage BID) for past 10 years. On intraoral examination, patient was completely edentulous and was wearing complete denture. As there was swelling in the palate, she was unable to wear the denture. Clinical examination revealed a single well defined swelling of size 1.5cm x1.5cm in the right side of hard palate in relation to the missing 16, 17 region [Table/Fig-2]. The swelling appeared bluish in colour was soft, fluctuant and non-tender. No significant regional lymphadenopathy was present. Intra oral periapical radiograph revealed no evidence of bone loss in relation to 16 and 17. A provisional diagnosis of mucocele was considered with the clinical findings. Fine Needle Aspiration Cytology (FNAC) showed presence of red blood cells. This provoked us to consider lesions other than mucocele. Hence we planned for an open biopsy, as FNAC report advised us to correlate clinically. An excisional biopsy was performed under local anaesthesia using a 15 size BP blade and electro cautery due to the risk of bleeding. Haemostasis was achieved [Table/Fig-3]. A specimen of 10mm x 15mm was obtained [Table/Fig-4]. A periodontal dressing pack was placed on the maxillary complete denture to cover the defect and to reduce the oedema [Table/Fig-5]. Histopathological examination revealed thin squamous epithelium. The underlying connective tissue showed dense proliferation of adipose tissue along with dilated blood capillaries [Table/Fig-6]. There was no soft tissue infiltration or bony erosion and hence it was diagnosed to be a non-infiltrating type. A one week postoperative review showed healing defect in the palate [Table/Fig-7]. One month follow up showed satisfactory wound healing with minimal scarring. A three month postoperative follow up showed good wound healing with total disappearance of the lesion [Table/Fig-8]. A complete dental rehabilitation was performed for the patient [Table/Fig-9].
Extraoral Photo of the patient.

Intraoral Photograph show the lesion on the Right side of the Palate.

Immediate postoperative Intra oral photograph.

Periodontal dressing to cover the defect and denture stabilized with primary retention.

Microphotograph of the specimen showing thin squamous epithelium with underlying connective tissue showing dense proliferation of adipose tissue along with dilated blood capillaries [40x].

Progressive wound healing after one week.

Three months postoperative wound healing.

Discussion
Angiolipoma is one of the variant of lipoma which was first described by Bowen in 1912 [1]. Head and neck region has been a rare site for the occurrence of angiolipoma [2].
Lipoma is a benign neoplasm that arises from the fat tissue of the body. It is usually soft in consistency, slow growing and most asymptomatic in nature. Angiolipoma is a subtype of lipoma which consists of adipose tissue and vascular components in it [3]. Angiolipoma can be differentiated from other lipomas by the presence of fibrinous micothrombi. This benign tumour is commonly found in the extremities, it is quite uncommon to find it in the oral cavity [4]. Among all neoplasms of the oral cavity,1 to 5% are lipomas and angiolipoma accounts for 5 to 17% in it. The first occurrence of angiolipoma in oral cavity was identified by Davis et al., [5]. There is no sex predilection for this tumour. Angiolipoma frequently is encapsulated or non-encapsulated and can be easily distinguished from other lipomas by the presence of excessive vascular elements [6]. This tumour is usually soft, painless, round and freely mobile in the soft tissues. Mostly these are familial but their genetic transmission is unclear. Angiolipoma have a hamartomatous origin. Various factors have been found to be the etiology of angiolipoma like history of trauma, vascular transformation of lipoma, hormonal imbalance and a central hemangioma undergoing fatty degeneration [2]. Neurilemmoma, myxolipoma, mucocele and Kaposi’s sarcomas are the differential diagnosis of this lesion. However these lesions lack the vascular elements in them. Gonzales – Crusi et al., classified angiolipoma as infiltrating and non-infiltrating type [4]. The non-infiltrating type is encapsulated and occurs in young individuals. The main modality of treatment in infiltrative and non-infiltrative types of angiolipoma is by surgical excision [4]. In 35 to 50% of cases infiltrating type of angiolipoma has been found to recur after surgical excision [7]. Recurrence after surgery is quite rare. The infiltrating angiolipoma is usually poorly encapsulated, occurs in older patients and usually recurs after surgery [6]. Infiltration angiolipoma invades into the adjacent structures and is most common in the head and neck region. Microscopically, these are characterized by the presence of mature adipocytes, proliferation of thin walled vessels in the connective tissue which differentiates it from lipomas. When there are bony changes in the radiograph and increased vascularity, then the possibility of liposarcoma should be considered [8]. Total surgical excision is the treatment of choice for both the infiltrative and non-infiltrative angiolipoma [9]. In case of inadequate excision, radiotherapy is advisable. However in case of non-infiltrating angiolipoma, a simple excision will cure the condition as this lesion has no tendency to recur after surgical removal. However, the chances of recurrence of infiltrating type are high.
Conclusion
As far as our knowledge non infiltrating type of angiolipoma occurs in younger patients, this case report of non-infiltrating angiolipoma of the palate shows the importance to include these lesions as differential diagnosis for palatal swellings in a geriatric patient.
[1]. Choi JY, Goo JM, Chung MJ, Kim HC, Im JG, Angiolipoma of the Posterior Mediastinum with extension into the spinal cord: A case reportKorean J Radiol 2000 1:212-14. [Google Scholar]
[2]. Pattipati S, Naveen Kumar M, Ramadevi Praveen Kumar B, Palatal Lipoma: A case ReportJ Clin Diagn Res 2013 7(12):3105-06. [Google Scholar]
[3]. Yanase S, Nomura J, Matsumura Y, Angiolipoma of the cheek: a case report with a literature reviewAsian Journal of Oral and Maxillofacial Surgery 2011 23:35-37. [Google Scholar]
[4]. Lin JJ, Lin F, Two entities in angiolipoma: A study of 549 cases of lipoma with review of literature on infiltrating angiolipomaCancer 1974 34:720 [Google Scholar]
[5]. Davis GB, Stoelinga P, Tideman H, Angiolipoma of the hard palate: A case report and review of literatureJ Maxillofac Surg 1976 4:242-44. [Google Scholar]
[6]. Flaggert JJ, Heldt LV, Keaton WM, Angiolipoma of the palate. Report of a caseOral Surg 1986 60:333 [Google Scholar]
[7]. Weitzner S, Moynihan PC, Miss J, Angiolipoma of the cheek in the childOral Surg 1978 45(1):95-97. [Google Scholar]
[8]. Dalambiras S, Tilaveridis I, Lordanidis S, Zaraboukas T, Epivatianos A, Infiltrating angiolipoma of the oral cavity: Report of case and literature reviewJ Oral Maxillofac Surg 2010 68:681-83. [Google Scholar]
[9]. Palaia G, Gaimari G, Giudice RL, Excision of an oral angiolipoma by KTP laser: A case reportAnnali di Stomalogia 2011 II(1-2):28-31. [Google Scholar]