The sternalis muscle, an uncommon anatomical variant of the chest wall musculature, though perhaps well known to anatomists, is quite unfamiliar to clinicians and radiologists despite attempts to highlight its clinical importance in recent years. During routine dissection for undergraduate medical teaching, in the department of anatomy, we came across two cases of sternalis muscle. The first was a unique case of unilateral right sternalis with contralateral insertion on the left sternocleidomastoid, and the second case where bilateral presence of the muscle was noted with ipsilateral insertion. The former was supplied by medial pectoral nerve and the latter by lower intercostal nerves. Usually present between the pectoral and superficial fasciae, wide ranging prevalence and morphology have been attributed to this muscular variant. Opinions differ on its development and nerve supply. Its presence can be misdiagnosed as a wide range of benign and malignant anterior chest wall lesions and tumours, but it is also of great use as a pedicle flap or flap microvascular anastomosis in reconstructive surgeries of anterior chest wall, head and neck and breast. In this paper, two cases of sternalis muscle which presented very differently from each other are discussed.
Mammogram, Muscular variant, Parasternalis, Rectus thoracicus superficialis
Case 1
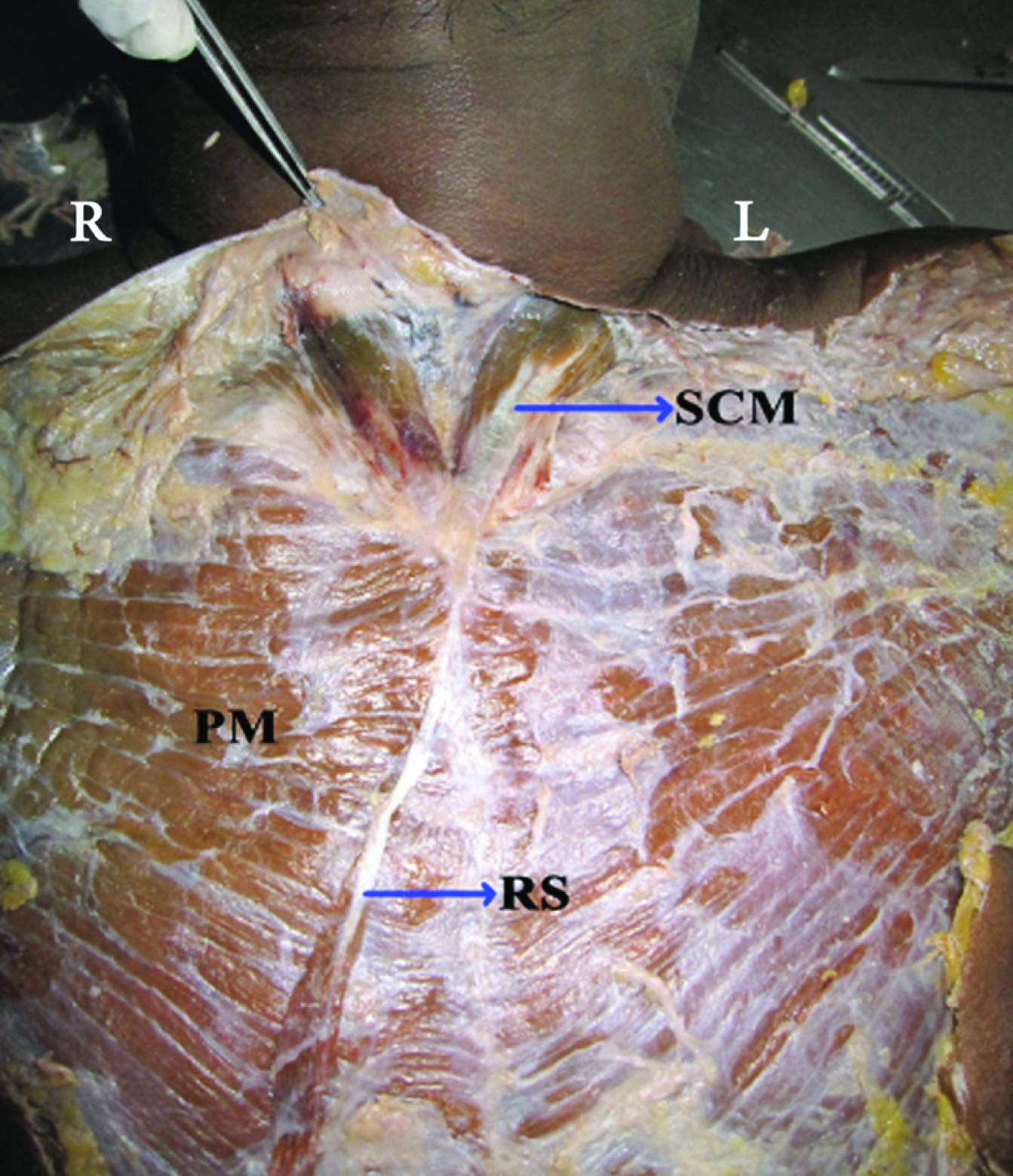
A unilateral rectus sternalis muscle was observed in a 80-year-old male cadaver. Located on the right side, the muscle took origin by a small fleshy belly from the lower part of pectoral fascia, at the level of 7th costal cartilage. The fusiform muscle belly tapered into a thin delicate tendon at the level of 4th costal cartilage, continued, for a short distance along right sternal margin, before crossing the sternum from right to left over the sternal angle and the left clavicle to merge with the sternal head of left sternocleidomastoid muscle [Table/Fig-1]. The muscle was supplied by twigs from the medial pectoral nerve.
Unilateral right sternalis muscle with contralateral insertion on the left sternocleidomastoid
R:Right, L:Left, PM:Pectoralis major, SCM:Sternocleidomastoid, RS:Rectus sternalis
Case 2
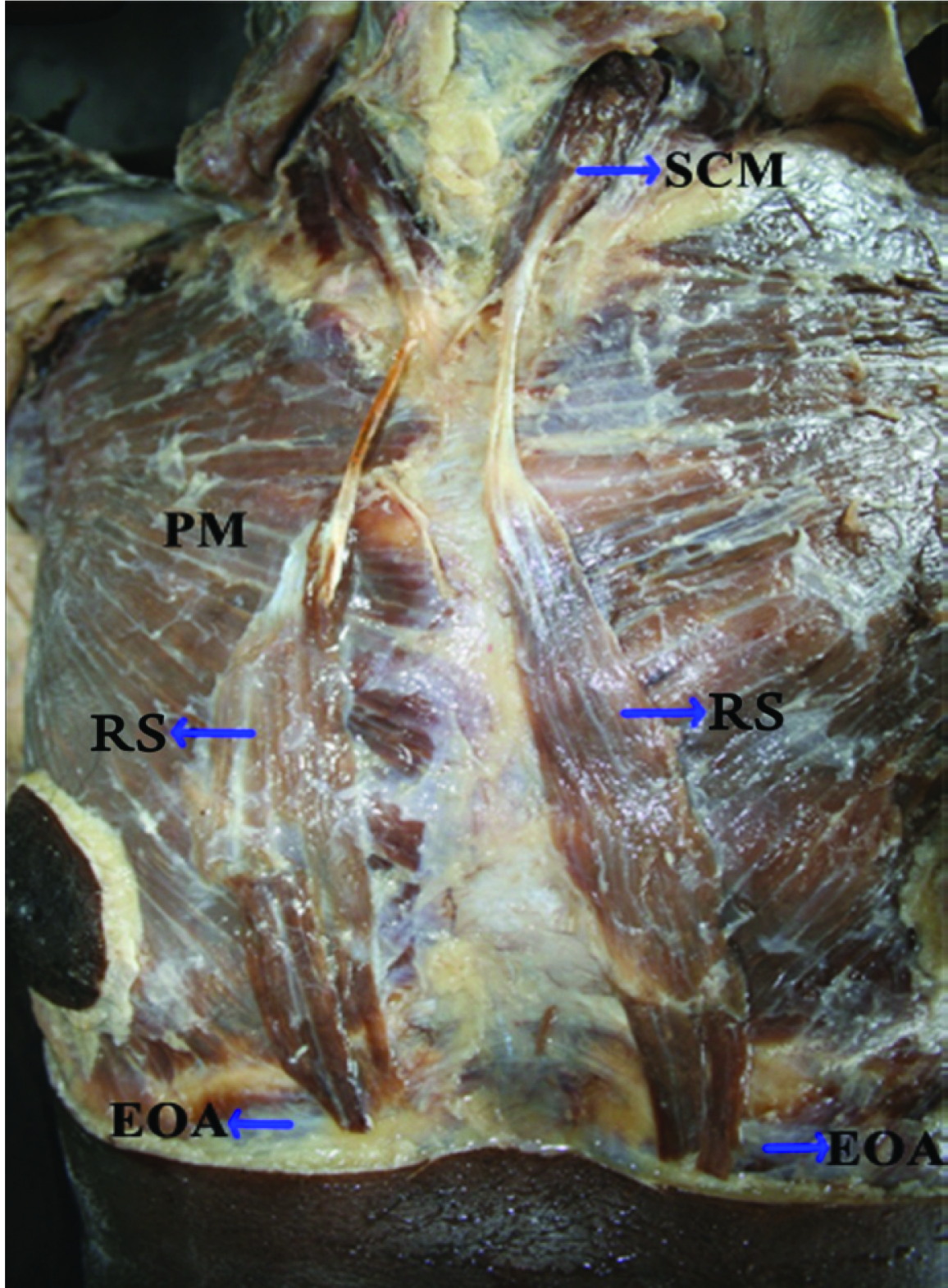
Bilateral sternalis muscle was observed in a 70-year-old male cadaver. Muscles on both sides, roughly fusiform in shape, had a fleshy origin from external oblique aponeurosis at the level of seventh costal cartilage. The muscles became tendinous near the sternal angle, continued upwards and crossed the clavicle, to insert into the sternal head of ipsilateral sternocleidomastoid. Both muscles were innervated by lower intercostal nerves [Table/Fig-2].
Bilateral rectus sternalis muscle with ipsilateral insertion
PM:Pectoralis major, SCM:Sternocleidomastoid, RS:Rectus sternalis, EOA:External oblique aponeurosis
Discussion
The sternalis muscle is known by a host of synonyms including episternalis, parasternalis, rectus sternalis, rectus thoracicus superficialis etc [1], courtesy various authors who have studied this muscle, probably to accurately describe its location and morphology. Cadaveric studies reveal a wide ranging prevalence both within and between geographic groups, the highest ratio of 11.5% being reported in Asian population and the lowest of 4.4% in Europeans [2]. According to Jelev et al., among Asians, the least prevalence of 1% is among Taiwanese and maximum of 23.5% in Northern Chinese [3]. The reported differences in prevalence rates could be due to small sample size or due to the fact that one could easily miss noticing a small ill defined muscle [2]. The prevalence is not well known in India, as hardly any studies have been done on the Indian population except by Harish et al., and Katara P et al., who reported prevalence rates of 0.69% and 3.3% respectively [1,4]. However, there are about ten case reports from India by different authors [5–14], during the five year period from 2011-2015.
The development of the muscle is often a bone of contention. The most common view attributes its origin to pectoralis major and rectus abdominus due to the fact that sternalis muscle is usually supplied by pectoral or intercostal nerves [15,16]. But Turner who did an in-depth study on sternalis muscle did not come across a single case of continuity of sternalis with rectus abdominis muscle [17]. The inferior attachment of sternalis was often to the external oblique aponeurosis which lies in a more superficial plane to the rectus abdominis [2].
In our second case, the inferior attachment of sternalis was to the external oblique aponeurosis and the muscle was innervated by lower intercostal nerves. Researchers who support the view that sternalis is derived from rectus state that sternalis was found to be innervated by intercostal nerves [3,15]. But according to Snosek et al., [2], the innervation could be inappropriately attributed to the intercostal nerves as they exit very close to the muscle, or traverse the muscle on the way to their cutaneous destinations.
Ever since Cunningham traced small nerve twigs supplying sternalis muscle to the pectoral nerves, the hypothesis that sternalis could be a derivative of pectoralis major gained strength [18]. Cunningham et al., emphasized that the delicate branches of the pectoral nerves to the sternalis muscle may be damaged during routine dissection and hence overlooked [19]. In our first case, the unilateral sternalis was innervated by medial pectoral nerve. Cunningham believed that sternalis is an aberrant, displaced, rotated segment of pectoralis muscle mass [18].
Sternalis is often found to have connections with pectoralis major muscle [3,15,17]. The muscular connects ranging from a few muscle fibres to large fascicles could result from incomplete or partial rotation of the segments of the pectoralis muscle and may cause deficits in it [2]. If these displaced segments migrate from their normal course, they may make connections with adjacent structures resulting in apparent continuity with sternocleidomastoid above or rectus abdominis below [2].
This hypothesis can explain the attachment of the sternalis across the midline. The displaced segment migrating across the midline might have resulted in a crossed sternalis muscle as observed in our first case.
After extensive research on sternalis muscle, Snosek et al., [2] stated that its presence could be attributed to variations caused by dis-turbance to the normal process of development of the pectoralis major muscle which include similar variations like pectoralis minimus, pectoralis tertius, infraclavicularis, chondroepitrochlearis etc, as reported by Bergman et al., [20]. In many instances, the presence of the sternalis muscle is associated with atypical development of pectoralis major or deficiencies in the medial aspect of pectoralis major muscle [17,18].
Relatively small sized without apparent function [17], the sternalis muscle is not associated with any evident clinical symptoms [2]. But its presence could be of great clinical significance due to its ability to alter routine mammograms [21].
The early detection of breast cancer often depends on high quality mammography [21]. Improved imaging of the deeper portions of the breast periodically reveals an irregular mass projected over the medial aspect of the craniocaudal mammogram, which is the sternalis muscle, sometimes confusing the radiologist thus leading to misdiagnosis. Bradley et al., reported that 4 women of an estimated 32,000 who had mammograms had an unusual irregular structure, visible medially on the craniocaudal projection that posed a diagnostic dilemma [21]. The medial aspect of the breast where lesions can be present is coincidentally where sternalis muscle is most commonly visible [22].
The sternalis muscle, when present appears as a flame shaped or speculated triangular structure on the medial aspect of craniocaudal projections [23]. Identification and recognition of this rare anatomical variant can reduce the chances of misdiagnosis, avoid subsequent diagnostic procedures like biopsies, and also misinterpretation as recurrence at a later date [4]. Sternalis muscle when present can mimic a focal density and its presence can be confirmed by MRI or CT imaging [23].
Sternalis muscle has surgical implications too. It can be used to cover the prosthesis in augmentation mammoplasty or as a pedicle flap in plastic and reconstructive surgeries of the head and neck [24]. There are very few reports in the literature of sternalis muscle crossing the midline [7,10,17,25]. As described earlier, this can be attributed to development.
Sternalis is an anatomical variant of the chest wall musculature with varying prevalence and morphology. Its development and hence nerve supply is debated but the most convincing concept attributes its development to pectoralis major [2]. Generally, muscles of the body are bilaterally symmetrical and never cross the midline, except perhaps, small muscles of face, like compressor naris, orbicularis oris, etc, or the muscles of the larynx, such as transverse or oblique arytenoids, where they serve specific function. In our first case, the tendon of right sternalis muscle crossed to the opposite side across the sternum and gained attachment to the left sternocleidomastoid which is very rare. This could strengthen the view that sternalis muscle could be considered as a displaced segment of pectoralis major muscle which has migrated from its normal position and made connections with opposite sternocleidomastoid [2].
Conclusion
Though without any significant physiological function, the presence of sternalis muscle has tremendous clinical importance owing to its potential in confusing radiologists while interpreting mammograms and at the same time, is of use as a pedicle flap in the reconstructive surgeries of the head and neck as well as a cover for prosthesis in reconstructive surgeries of the breast. Hence radiologists and surgeons operating on this area should be well aware of this muscular variant.
[1]. Katara P, Chauhan S, Arora R, Saini P, A unilateral rectus sternalis muscleJ Clin Diagn Res 2013 79(12):2665-67. [Google Scholar]
[2]. Snosek M, Tubbs SR, Loukas M, Sternalis muscle. What every anatomist and clinician should knowClinical Anatomy 2014 27:866-84. [Google Scholar]
[3]. Jelev L, Georgiev G, Surchev L, The sternalis muscle in the Bulgarian population: Classification of sternalesJ Anat 2001 199:359-63. [Google Scholar]
[4]. Harish K, Gopinath KS, Sternalis muscle - Importance in surgery of the breastSurg Radiol Anat 2003 25:311-14. [Google Scholar]
[5]. Vaithianathan G, Aruna S, Rajila RHS, Balajim T, Sternalis “mystery” muscle and its clinical implicationsIJAE 2011 116(3):139-43. [Google Scholar]
[6]. Patel MM, Singel TC, A Unilateral Rectus Sternalis: An Important Variant in the Thoracic RegionNJIRM 2011 2(2):53-55. [Google Scholar]
[7]. Simhadri D, Suseelamma D, Praveen Kumar M, Uncommon Variation in Musculature of the Chest wallAnat Physiol 2012 2:113 [Google Scholar]
[8]. Singla RK, Sachdeva K, Bilateral Musculus Sternalis: A Case ReportJCDR 2012 6(3):465-68. [Google Scholar]
[9]. Raju S, Raghu J, Reddy SM, Sirisha B, Indira B, Sujata M, An Unilateral Rectus Sternalis Muscle: It’s Clinical SignificanceJournal of Surgical Academica 2012 2(1):21-22. [Google Scholar]
[10]. Roy N, Roy S, Sternalis muscleJournal of current trends in clinical medicine & laboratory biochemistry 2013 1(3):50-52. [Google Scholar]
[11]. Bharathi D, Sarala HS, Padmalatha N, Balakrishna Morphology of Rectus Sternalis: A Cadaveric StudyInternational Journal of Life Sciences Research 2014 2(4):65-67. [Google Scholar]
[12]. Cherian SB, Gandhalam AJ, Rectus sternalis muscle: An anatomical variant of anterior chest wall Rectus sternalis muscle: An anatomical variant of anterior chest wallOA Anatomy 2014 2(2):16 [Google Scholar]
[13]. Bilodi AS, Sasikala P, Anuradha P, Karthikeyan V, A study on muscle variant – rectus sternalisWorld Journal of Pharmacy and Pharmaceutical Sciences 2015 4(4):1035-40. [Google Scholar]
[14]. Gajare RA, Sternalis A Case ReportInternational Journal of Scientific Study 2015 2(10):154-57. [Google Scholar]
[15]. O’Neill MN, Folan-Curran J, Case report: bilateral sternalis muscle with bilateral pectoralis major anomalyJ Anat 1998 193:289-92. [Google Scholar]
[16]. Kida MY, Kudoh H, Innervation of the sternalis muscle accompanied by congenital partial absence of the pectoralis major muscleOkajimas Folia Anat Jpn 1991 67:449-55. [Google Scholar]
[17]. Turner WM, On the musculus sternalisJ Anat Physiol 1867 1:246-53. [Google Scholar]
[18]. Cunningham DJ, The muscle sternalisJ Anat Physiol 1884 18:208-10. [Google Scholar]
[19]. Cunningham DJ, The muscle sternalisJ Anat Physiol 1888 22:391-407. [Google Scholar]
[20]. Bergman RA, Thompson SA, Afifi AK, Saadeh FA, Compendium of Human Anatomic VariationBaltimoreUrban and Schwarzenberg [Google Scholar]
[21]. Bradley FM, Hoover HC, Hulka CA, Whitman GJ, McCarthy KA, Hall DA, The sternalis muscle - An unusual normal finding seen on mammographyAmer J Roentgenol 1996 166:33-36. [Google Scholar]
[22]. Pojchamarnwiputh S, Muttarak M, Na-Chiangmai W, Benign breast lesions mimicking carcinoma at mammographySingapore Med J 2007 48:958-68. [Google Scholar]
[23]. Goktan C, Orguc S, Serter S, Ovali GY, Musculus sternalis - A normal but rare mammographic finding and magnetic resonance imaging demonstrationBreast J 2006 12:488-89. [Google Scholar]
[24]. Khan UD, Use of the rectus sternalis in augmentation mammoplaty: Case report and literature searchAnesthetic Plast Surg 2008 32:21-24. [Google Scholar]
[25]. Raikos A, Paraskevas GK, Tzika M, Faustmann P, Triaridis S, Kordali P, Sternalis muscle : a new crossed subtype, classification, and surgical implicationsAnn Plast Surg 2011 67:646-68. [Google Scholar]