Introduction
Acute coronary syndrome (ACS), a spectrum comprising unstable angina pectoris, ST Elevated Myocardial Infarction (STEMI) & Non ST Elevated Myocardial Infarction (NSTEMI) is the major cause of presentation in Emergency Department today. Though ECG and cardiac enzymes are used for diagnosis, they mislead the diagnosis sometimes and delay in treatment initiation. This leads us to search certain new parameters which reflect the pathophysiology of ACS. Markers of plaque stability like Pregnancy Associated Plasma Protein-A and D-Dimer, a marker of ongoing thrombosis are found to be better markers in early diagnosis.
Aim
To evaluate the diagnostic competence of PAPP-A and D-Dimer in acute coronary syndrome over CK-MB and to compare with the inflammatory marker High Sensitive C-Reactive Protein (hs-CRP) which is associated with atherosclerosis.
Materials and Methods
Fifty patients presenting with acute onset of chest pain to Emergency Department with or without ECG changes served as cases and 50 healthy people served as controls. Serum PAPP-A is measured by Enzyme Linked Immunosorbent Assay (ELISA), D-Dimer and hs-CRP by using Latex Turbidimetry method.
Results
A statistical significant difference of PAPP-A and D-Dimer was noted between the ACS and controls (p < 0.001) whereas CK-MB shows no much difference (p 0.09). Statistically significant positive correlation is noted between parameters.
Conclusion
PAPP-A marker of plaque instability and D-Dimer marker of ongoing thrombosis are raised in acute coronary syndrome and thus can be considered as one of the marker in ACS for diagnosis.
Introduction
With the change in lifestyle habits and increased incidence of atherosclerosis the incidence of acute coronary syndrome increased comprising the major group of presentation to the emergency department. Acute Coronary Syndrome (ACS) is a group of disorders consisting of Unstable Angina (UA), Non ST Elevated Myocardial Infarction (NSTEMI), ST Elevated myocardial infarction (STEMI) [1,2].
Among the various groups of ACS, NSTEMI and UA diagnosis is difficult with the routinely done investigations as ECG changes are not seen in both and the raise of cardiac markers which is a differentiating feature between them occurs lately. This is the cause of mislead or missing of diagnosis and delay in initiation of treatment [3].
The cardiac markers used widely at present are markers of cardiac ischemia which include CK-MB, Troponins, and Myoglobin. Minimum time taken for their expression in blood is 2 hours which delays the treatment [4]. In order to initiate treatment at early we need parameters that reflect the ongoing pathology i.e., atherosclerotic formation and rupture. Pregnancy Associated Plasma Protein-A (PAPP-A) secreted from fibroblasts and vascular endothelial cells enhances accumulation of inflammatory cells and lipid laden macrophages thus causing progression of atherosclerosis. PAPP-A also found to play role in atheroma rupture initiating the thrombosis [5]. Ongoing thrombosis in coronary vessels consumes platelets and clotting factors. This process being disorganized there is both fibrin deposition and degradation and thus fibrin degradation marker D-Dimer found to be increased in ACS [6].
With this view we aimed to study the changes of PAPP-A and D-Dimer in both cases and control subjects thus evaluating their diagnostic efficacy over the routinely done cardiac marker CK-MB in early period.
Materials and Methods
Study was conducted in Department of Biochemistry, JJM Medical College after the approval of ethical committee for over a period of one year i.e., from September 2013 to August 2014.
All patients presented with chest pain to the emergency department of Bapuji Hospital & Chigateri General Hospital were taken as study subjects. After informed consent blood samples were collected by venipuncture under aseptic precautions at the time of admission with a precaution of considering the study subjects who presented within 2 hours of acute onset of chest pain, and both serum and plasma are separated and stored at -200c until the assay is done.
The study subjects with liver and kidney disorders, inflammatory arthritis, infections, brain ischaemia, tumours, bleeding disorders, DM, pregnant women and samples collected after 2 hours of acute onset of chest pain are excluded from the study group.
After exclusions based upon the diagnosis at the time of discharge by electrocardiogram and cardiac troponin 50 patients were grouped under cases i.e., ACS which include 35 STEMI, 15 NSTEMI cases and 50 apparently age and sex matched healthy individuals as controls.
PAPP-A was analysed by ELISA method as per the instructions given by the manufacturer DRG international, Germany [7]. Whereas hs-CRP & D-Dimer measured by Latex Turbidimetric method as per the instructions given by the manufacturer EURO Diagnostics & Tulip Diagnostics Chennai [8,9].
Serum levels of PAPP-A up to 2.5mIU/L, plasma D-Dimer up to 250ng/ml DDU, hs-CRP up to 3mg/L are considered as normal [10–12].
Statistical Analysis
All values are expressed in terms of Mean±SD and subjected to proper statistical analyses using Microsoft excel with QI macros software where Z-test applied to find out the statistical significance between cases & controls. Pearson correlation analysis was done for identifying the correlation between the parameters. P-value < 0.05 considered as statistically significant.
Results
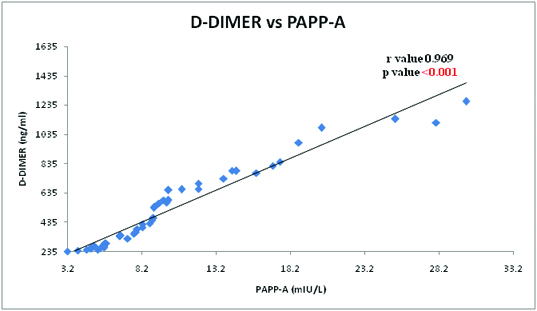
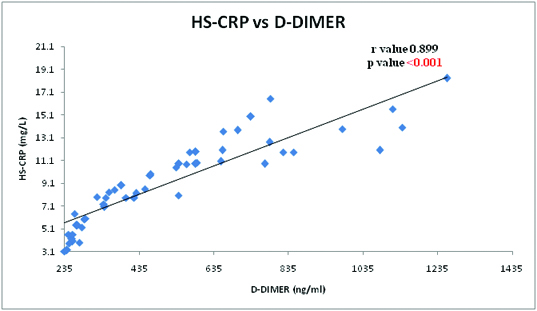
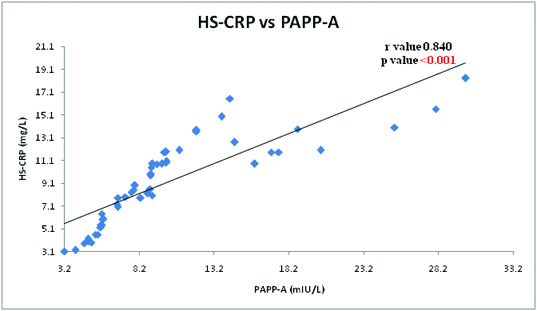
Mean values of PAPP-A, D-Dimer, hs-CRP were showing significant elevation in ACS over controls with a p-value of <0.001 whereas CK-MB values are not raised significantly in ACS as shown in the [Table/Fig-1]. This is because samples are collected within 2 hours of onset of chest pain and normally CK-MB rises after 4-6 hours of onset of symptoms reaching a peak after 24 hours. Pearson correlation analysis was done between the parameters a significant positive correlation is noted between them with a p-value of <0.001 as shown in [Table/Fig-2,3 and 4]. Among them a very strong positive correlation noted between PAPP-A and D-dimer with an r-value of 0.969.
Mean±SD of various parameters in ACS and Controls
| Parameter | Controls | ACS | Z score | p-value |
|---|
| PAPP-A | 1.2 ± 0.6 | 10.2 ± 5.9 | 10.54 | <0.001 |
| D-Dimer | 29.5 ± 18.6 | 524.9 ± 266.4 | 12.9 | <0.001 |
| HS-CRP | 1.5 ± 0.8 | 9.2 ± 3.7 | 14.26 | <0.001 |
| CK-MB | 13.7 ± 4 | 14.9 ± 3 | 1.69 | 0.09 |
PAPP-A: Pregnancy Associated Plasma protein-A ACS: Acute Coronary Syndrome
PAPP-A: Pregnancy Associated Plasma protein-A HS-CRP: High Sensitive C-Reactive Protein
CK-MB: Creatine Kinase MB ACS: Acute Coronary Syndrome
Correlation graph showing positive correlation between PAPP-A and D-Dimer in ACS
Correlation graph showing positive correlation between HS-CRP and D-Dimer in ACS
HS-CRP: High Sensitive C-Reactive Protein ACS: Acute Coronary Syndrome
Correlation graph showing positive correlation between PAPP-A and HS-CRP in ACS
PAPP-A: Pregnancy Associated Plasma protein-A HS-CRP: High Sensitive C-Reactive Protein
ACS: Acute Coronary Syndrome
Discussion
Pregnancy associated plasma/placental protein-A (PAPP-A) is a zinc metalloproteinase identified in 1973 for the first time [13]. It was introduced as marker of downs syndrome and used in prenatal diagnosis along with ultrasound Doppler and free β-HCG [14]. Later found to be useful in diagnosis of pre-eclampsia in early trimester [15]. PAPP-A initially thought to be secreted by placental syncitiotrophoblasts was found to be expressed in ACS in the 2001 [16].
Role of PAPP-A in pathogenesis of ACS was established when Beaudeux JL et al., found PAPP-A in echogenic carotid atherosclerotic plaques of non-symptomatic hyperlipidemic patients by immunohistochemistry thus proving PAPP-A plays a key role in atheroma formation [17]. Whereas Brugger-Anderson et al., had shown increased expression of PAPP-A in atherothrombotic plaques by immunohistochemistry techniques from STEMI patients during postmortem denoting its role not only in atheroma formation but has a role in plaque rupture [18].
PAPP-A via IGF-1 action enhances the atheroma formation by modification of extra-cellular matrix. It is also responsible for instability by fibrous cap thinning [19]. Present study shows significant difference of PAPP-A between the ACS and control groups which is long with studies of Bayes-Genis et al., Iversen et al., [5,19].
PAPP-A, a matrix metalloproteinase exhibits Insulin Growth factor (IGF) cleaving action from its binding protein Insulin Growth Factor Binding Protein-4 (IGFBP 4). The free IGF plays a key role in proliferation of vascular smooth muscle and fibroblast thus altering the peri vascular matrix and enhancement of atheroma formation [20,21]. Apart from atheroma enhancement it also causes chemotaxis of monocytes and neutrophils that leads to increased production of inflammatory markers like hs-CRP [22,23]. Because of increased PAPP-A, the enhancing atheroma leads to thinning of cap which causes increased fibrinogen accumulation and fibrin degradation products [24]. The increased inflammatory mediators further enhance the secretion of metalloproteinases like PAPP-A thus acting like a vicious cycle [25].
D-dimer a marker of cross linked fibrin turnover has been shown to be associated with risk of developing Ischemic Heart Disease (IHD) in future in people with & without baseline vascular disease [26–34]. Salomaa V et al., concluded that higher levels of D-Dimer seen in patients than controls suggesting the high turnover of fibrin, that fits the hypothesis of hyper-coagulable state which precedes the clinical CHD events [35]. In the present study we found significant high levels of D-dimer in ACS than in controls.
Arthur JM et al., found that higher levels of D-Dimer which reflects procoagulant state that contributes independently to recurrent coronary events [36]. Gordon et al., suggested that measurement of both D-dimer and CRP helps in enhancement of risk stratification for IHD [37].
High Sensitive CRP is a marker of plaque instability and inflammation where the levels are raised and noted at far early stages of atheroma formation Suleiman M et al., shown that CRP levels can predict the heart failure after episode of MI [38]. Raise of hs-CRP denotes the effect of inflammation secondary to myocardial necrosis in MI. Significant raise in hs-CRP-value is noted in acute coronary syndrome when compared with controls.
Studies also shown that PAPP-A and D-Dimer raised far early than the CK-MB currently used cardiac marker for ACS as both of them denotes ongoing pathogenesis whereas CK-MB reflects the effect of pathogenesis i.e., myocardial ischaemia [24]. A significant positive correlation is seen between the parameters denoting all are related to unstable athero thrombotic plaques and yet they differ with each other in predicting the outcome.
Heeschen et al., found that PAPP-A levels of >12.1 mIU/L denotes the risk of death/recurrent MI at 30 days & 6 months even with negative troponin results. Though the present study doesn’t comment regarding this because of lack of long term follow up of the study subjects [24].
Bayes Genis et al., found D-dimer level of >500 ng/ml had an independent diagnostic value for MI and increases the diagnostic sensitivity of ECG and history from 73% to 92% [39].
Limitation
Limitations of the present study are sample size not calculated and comparison with high sensitive cardiac troponin should have been done.
Conclusion
We found the markers of plaque instability like PAPP-A and markers of ongoing thrombotic activity like D-Dimer helps in early diagnosis than the routinely done cardiac ischemic markers in ACS. As they reflect the pathological process of ACS i.e., ongoing atherothrombosis PAPP-A and D-Dimer can be used to rule out the false positive cases like GERD and other non-cardiac chest pain that mimics cardiac chest pain. This help us in initiation of treatment appropriately thus decreasing the work load in emergency department.
Conflict of Interest: The authors declare no conflict of interest.
PAPP-A: Pregnancy Associated Plasma protein-A ACS: Acute Coronary Syndrome
PAPP-A: Pregnancy Associated Plasma protein-A HS-CRP: High Sensitive C-Reactive ProteinCK-MB: Creatine Kinase MB ACS: Acute Coronary Syndrome
[1]. Christopher P, Cannon, Eugene Braunwald: Non ST-Segment Elevation Acute Coronary Syndrome and Unstable Angina In Kasper LD, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JLHarrison Principles of Internal Medicine 2012 18th edMcGraw Hill:2015-2021. [Google Scholar]
[2]. Antman EM, Loscalzo J, ST Segment Elevation MI In Kasper LD, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JLHarrison Principles of Internal Medicine 2012 18th edMcGraw Hill:2021-35. [Google Scholar]
[3]. Menown IB, Mackenzie G, Adgey AA, Optimizing the initial 12-lead electrocardiographic diagnosis of acute myocardial infarctionEur Heart J 2000 21:275-83. [Google Scholar]
[4]. Morrow DA, Cannon CP, Jesse RL, Newby K, Ravkilde J, Storrow AB, National academy of clinical biochemistry laboratory medicine practice guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromesCirculation 2007 115:e356-75. [Google Scholar]
[5]. Bayes-Genis A, Conover CA, Overgaard MT, Bailey KR, Christiansen M, Holmes DR, Pregnancy associated plasma protein A as a marker of acute coronary syndromesN Engl J Med 2001 345:1022-29. [Google Scholar]
[6]. Fowkes FGR, Lowe GDO, Housley E, Rattray A, Elton RA, MacGregor IR, Cross-linked fibrin degradation products, risk of coronary heart disease, and progression of peripheral arterial diseaseLancet 1993 342:84-86. [Google Scholar]
[7]. Qiu PQ, Saara K, Juha L, Natalia T, Xuezhong Q, Mauri L, Immunoassays Developed for Pregnancy Associated Plasma Protein-A (PAPP-A) in Pregnancy May Not Recognize PAPP-A in Acute Coronary SyndromesClinical Chemistry 2006 52(3):398-404. [Google Scholar]
[8]. Johnson AM, Amino acid and proteins. In: CA. Burtis, ER. Eshwood, DE. BrunsTeitz fundamental of clinical chemistry 2008 6th editionNew DelhiElsevier:301-303. [Google Scholar]
[9]. Bojic M, Stegner M, Validation of an Automated Immunoturbidimetric Assay for Measurement of Plasma D-DimerClin Chem Lab Med 2003 41(7):958-62. [Google Scholar]
[10]. Gerthoffer W, Hellmich A, Aragon I, Massey C, Serum pregnancy associated plasma protein-A levels in a cohort with cardiovascular diseaseThe FASEB Journal 2014 28:1158.2 [Google Scholar]
[11]. Mayo Medical Laboratories. Available at: www.mayomedicallaboratories.com/test-catalog/clinical+and+interpretive/9290 last accessed on 25/08/2015 [Google Scholar]
[12]. Alan HB Wu, Tietz clinical guide to laboratory tests 2006 4th edElsevier Publications:332-333. [Google Scholar]
[13]. Gall SA, Halbert SP, Antigenic constituents in pregnancy plasma which are undetectable in normal non-pregnant female or male plasmaInt Arch Allergy Appl Immunol 1972 42:503-15. [Google Scholar]
[14]. Barrett SL, Bower C, Hadlow NC, Use of the combined first trimester screen result and low PAPP-A to predict risk of adverse fetal outcomesPrenat Diagn 2008 28:28-35. [Google Scholar]
[15]. Spencer K, Lu CKH, Savvidou M, Papageorghiou AT, Nicolaides KH, Prediction of pre-eclampsia by uterine artery Doppler ultrasonography and maternal serum pregnancy-associated plasma protein-A, free β-human chorionic gonadotropin, activin A and inhibin A at 22 + 0 to 24 + 6 weeks’ gestationUltrasound Obstet Gynecol 2006 27:658-63. [Google Scholar]
[16]. Laterza OF, PAPP-A: a marker of plaque instability. Is it ready for prime time?Future Cardiol 2005 1:495-500. [Google Scholar]
[17]. Beaudeux JL, Burc L, Imbert-Bismut F, Giral P, Bernard M, Bruckert E, Serum plasma pregnancy-associated protein A: a potential marker of echogenic carotid atherosclerotic plaques in asymptomatic hyperlipidemic subjects at high cardiovascular riskArterioscler Thromb Vasc Biol 2003 23:e7-10. [Google Scholar]
[18]. Brugger-Anderson Bostad L, Sandens DA, Larsen AI, Bonarjee VVS, Barvik S, The activity of pregnancy-associated plasma protein A (PAPP-A) as expressed by immunohistochemistry in atherothrombotic plaques obtained by aspiration thrombectomy in patients presenting with a ST-elevation myocardial infarction: a brief communicationThrombosis Journal 2010 8:1 [Google Scholar]
[19]. Iversen KK, Teisner AS, Teisner B, Kliem A, Thanning P, Grande P, Pregnancy-associated plasma protein A, a novel, quick and sensitive marker in ST segment myocardial infarctionAm J Cardiol 2008 101:1389-94. [Google Scholar]
[20]. Bayes-Genis A, Conover CA, Schwartz RS, Insulin-like growth factor axis: a review of atherosclerosis and restenosisCirc Res 2000 86:125-30. [Google Scholar]
[21]. Jones JI, Prevette T, Gockerman A, Clemmons DR, Ligand occupancy of the aVb3 integrin is necessary for smooth muscle cells to migrate in response to insulin-like growth factorProcNatlAcadSci USA 1996 93:2482-87. [Google Scholar]
[22]. Renier G, Clement I, Desfaits AC, Lambert A, Direct stimulatory effect of insulin-like growth factor-I on monocyte and macrophage tumour necrosis factor-a productionEndocrinology 1996 137:4611-18. [Google Scholar]
[23]. Ross R, Atherosclerosis — an inflammatory diseaseN Engl J Med 1999 340:115-26. [Google Scholar]
[24]. Heeschen C, Dimmeler S, Hamm CW, Fichtlscherer S, Simoons ML, Zeiher AM, Pregnancy associated plasma protein-A levels in patients with acute coronary syndrome: comparison with markers of systemic, inflammation, platelet activation and myocardial necrosisJ Am Coll Cardiol 2005 45:229-37. [Google Scholar]
[25]. Galis ZS, Sukhova GK, Kranzhofer R, Clark S, Libby P, Macrophage foam cells from experimental atheroma constitutively produce matrixdegrading proteinasesProcNatlAcadSci U S A 1995 92:402-06. [Google Scholar]
[26]. Cortellaro M, Confrancesco E, Boschetti C, Mussoni L, Donati MB, Cardillo M, Increased fibrin turnover and high PAI-1 activity as predictors of ischemic events in atherosclerotic patients: a case-control studyArterioscler Thromb Vasc Biol 1993 13:1412-17. [Google Scholar]
[27]. Ridker PM, Hennekens CH, Cerskus A, Stampfer MH, Plasma concentration of cross-linked fibrin degradation products (D-dimer) and the risk of future myocardial infarction among apparently healthy menCirculation 1994 90:2236-40. [Google Scholar]
[28]. Smith FB, Lee AJ, Fowkes FGR, Rumley A, Lowe GDO, Hemostatic factors as predictors of ischemic heart disease and stroke in the Edinburgh Artery StudyArterioscler Thromb Vasc Biol 1997 17:3321-25. [Google Scholar]
[29]. Lowe GDO, Yarnell JWG, Sweetnam PM, Rumley A, Thomas HF, Elwood PC, Fibrin D-dimer, tissue plasminogen activator, tissue plasminogen activator inhibitor, and the risk of major ischaemic heart disease in the Caerphilly StudyThromb Haemost 1998 79:129-33. [Google Scholar]
[30]. Smith FB, Rumley A, Lee AJ, Leng GL, Fowkes FGR, Lowe GDO, Haemostatic factors and prediction of ischaemic heart disease and stroke in claudicantsBr J Haematol 1998 100:758-63. [Google Scholar]
[31]. Lowe GDO, Rumley A, Use of fibrinogen and fibrin D-dimer in prediction of arterial thrombotic eventsThromb Haemost 1999 82:667-72. [Google Scholar]
[32]. Moss AJ, Goldstein RE, Marder VJ, Sparks CE, Oakes D, Greenberg H, Thrombogenic factors and recurrent coronary eventsCirculation 1999 99:2517-22. [Google Scholar]
[33]. Cushman M, Lemaitre RN, Kuller LH, Psaty BM, Macy EM, Sharrett AR, Fibrinolytic activation markers predict myocardial infarction in the elderly: the Cardiovascular Health StudyArterioscler Thromb Vasc Biol 1999 19:493-98. [Google Scholar]
[34]. Davies MJ, A macro and micro view of coronary vascular insult in ischemic heart diseaseCirculation 1990 82(II):38-46. [Google Scholar]
[35]. Salomaa V, Stinson V, Kark JD, Folsom AR, Davis CE, Wu KK, Association of fibrinolytic parameters with early atherosclerosisCirculation 1995 91:284-90. [Google Scholar]
[36]. Arthur JM, Robert EG, Victor JM, Charles ES, David O, Henry G, Thrombogenic factors and recurrent coronary eventsCirculation 1999 99:2517-22. [Google Scholar]
[37]. Gordon DOL, John WGY, Rumley A, Bainton D, Peter MS, C-Reactive Protein, Fibrin D-Dimer and incident Ischemic Heart Disease in the speedwell study: Are inflammation and fibrin turnover linked in pathogenesis?Arterioscler Thromb Vasc Biol 2001 21:603-10. [Google Scholar]
[38]. Suleiman M, Khatib R, Agmon Y, Mahamid R, Boulos M, Kapeliovich M, Early Inflammation and Risk of Long-Term Development of Heart Failure and Mortality in Survivors of Acute Myocardial Infarction: Predictive Role of C-Reactive ProteinJ Am Coll Cardiol 2006 47(5):962-68. [Google Scholar]
[39]. Bayes-Genis A, Mateo J, Santalo M, Oliver A, Guindo J, Badimon L, D-Dimer is an early diagnostic marker of coronary ischemia in patients with chest painAm Heart J 2000 140:379-84. [Google Scholar]