Introduction
Copper is an important trace element for normal growth and development of the body. It is also essential for maturation of collagen tissues. The purpose of the study was to estimate the serum copper levels in rheumatoid arthritis patients and to see its association with the various parameters of disease activity.
Materials and Methods
The study was carried out among 50 diagnosed rheumatoid arthritis patients (25 each of active disease & remission patients) and 50 age and sex matched controls. Fasting blood sample was collected for estimation of serum copper, haemoglobin level and ESR in the subjects.
Results
Mean serum copper level in the case group was found to be significantly higher than that of the control group (p-value<0.001). This increase of copper level was more in active disease than those with remission (p-value < 0.0001). A significant positive correlation was found between serum copper level and ESR, serum copper level and morning stiffness and a negative correlation was found between serum copper level and haemoglobin level in rheumatoid arthritis patients.
Conclusion
In rheumatoid arthritis patients, serum copper level may be used as an additional biochemical marker for estimation of disease activity.
Arthritis, ESR, Haemoglobin, Morning stiffness
Introduction
Rheumatoid arthritis is a chronic disease with a wide variety of systemic manifestations including persistent inflammatory synovitis, usually involving peripheral joints in a symmetric manner. Synovitis leads to cartilage damage and bone erosions and subsequently leads to changes in joint integrity. Clinical presentation varies from mild oligoarticular illness to relentless progressive polyarthritis with significant functional impairment [1].
According to the modern concept, the pathogenesis of RA is a complex process involving synovial cell proliferation and fibrosis, pannus formation and cartilage and bone erosion [2–4]. In India, the prevalence of rheumatoid arthritis in rural population is 0.7% according to Malviya et al., [5].
American College of Rheumatology developed revised criteria in 1987, for classification of RA, which demonstrate a sensitivity of 91-94% and a specificity of 89%. These criteria can be used as guidelines for establishing diagnosis. According to this revised criteria, four of seven criteria are required to classify a patient as having rheumatoid arthritis (RA). The seven criteria includes: morning stiffness, arthritis of three or more joint areas, arthritis of hand joints, symmetric arthritis, rheumatoid nodules, serum rheumatoid factor and radiographic changes [1,6].
Foods high in copper and copper bracelets were thought to be beneficial in treating arthritic conditions. In 1945, patients with rheumatoid arthritis were shown to exhibit higher than normal serum copper levels [7]. Copper complexes were used in the treatment of RA in the 50’s and 60’s [8]. Even the time-tested copper bracelet was eventually shown to be an effective anti-inflammatory, due to the absorption of copper through the skin. In fact, the main copper containing enzyme, ceruloplasmin, is significantly elevated in inflammatory conditions and has anti -inflammatory activity [9,10]. Most of the copper found in human body is in protein bound form like ceruloplasmin, copper-albumin, metallothionines, copper containing enzymes like cytochrome c oxidase, superoxide dismuatse, lysyl oxidase etc. It plays a role in the production of haemoglobin, (the main component of RBCs), myelin (the substance that surrounds nerve fibres) and melanin (a dark pigment hair and skin). Copper deficiency significantly lower the activity of the copper dependent enzymes due to which determination of copper required by the body is important [11].
Many studies are available which found variable results regarding serum copper levels in RA patients [12–15].
Keeping the above points in mind, we made an attempt to do a study on serum level of copper in RA patients and to see the association between the markers of disease activity and the level of serum copper in RA, if any.
Materials and Methods
This hospital based cross-sectional study was carried out among 50 cases of rheumatoid arthritis that were diagnosed according to the revised criteria outlined by American College of rheumatology, 1987. Fifty age and sex matched subjects were taken as control.
Diagnosis of RA was made as per ACR (American college of Rheumatology) criteria for clinical remission of rheumatoid arthritis [6]. RA patients not in clinical remission were taken as having active disease. Conditions found to increase copper levels-any other acute inflammatory conditions, renal, hepatic diseases, urinary tract infections, leprosy, malignancies, pregnant women, patients on oral contraceptive pills, patients wearing copper bracelets, ornaments or patients using copper utensils for cooking and feeding were excluded from the study. Also care was taken to exclude patients on disease modifying anti rheumatic drugs (DMARDS) or any other antibiotic.
Fasting blood samples were collected for estimation of serum copper, haemoglobin level and ESR. Serum copper level was estimated within 2 to 3 hours of blood-collection, in the department of biochemistry, by simple and sensitive colorimetric method.
Copper, released from ceruloplasmin in an acidic medium, reacts with Di-Br-PAESA to form a orange-red coloured complex. Intensity of the complex formed is directly proportional to the amount of copper present in the sample [16].
Erythrocyte Sedimentation rate (ESR) and haemoglobin levels were estimated by Westegrens method and acid haematin method respectively.
Statistical Analysis
A database was constructed on Microsoft Excel 2007, and statistical analysis was done. Students t-test and Pearson’s correlation tests were done.
Results
Morning stiffness, haemoglobin, ESR and serum copper levels were measured in control and case groups and means and standard deviations were calculated [Table/Fig-1].
Parameters measured in the study group
| Parameters | ControlsMean ± SD | Active disease(Mean ± SD) | Disease in remission(Mean ± SD) |
|---|
| Serum Cu (μg/dl) | 111.16 ± 24.95 | 200 ± 23.18 | 151.6 ± 21.15 |
| ESR (mm) | 21.26 ± 15.77 | 80 ± 25 | 17.36 ± 6.38 |
| Haemoglobin(g/dl) | 10.86 ± 2.17 | 8.41 ± 1.41 | 9.42 ± 1.45 |
| Morning stiffness | ……. | 40min aprox. | <12min |
In the study, we found higher incidence of RA in females (76%) than in males (24%). The ratio was found to be approximately 1:3.
Mean serum copper level amongst male and female cases was 172.91μg/dl and 176.71 μg/dl respectively. There was no significant difference (p-value >0.05) in serum copper level between the two groups, as evaluated by applying students t-test.
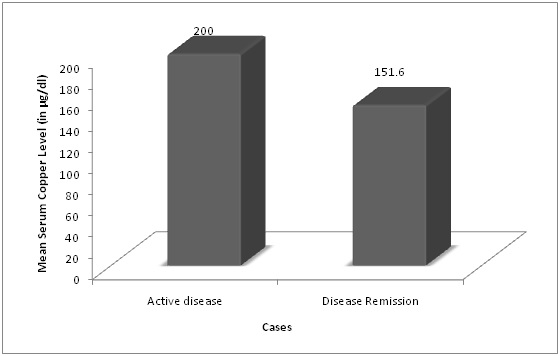
The mean serum copper level in the case group was significantly higher than in control group (p-value<0.001). On comparing 25 cases of active disease with 25 cases of disease in remission, the mean serum copper was found to be 200 ± 23.18 μg/dl and 151.6 ±21.15 μg/dl respectively, thus showing a highly significant difference in the two groups (p-value < 0.0001) [Table/Fig-2].
Bar diagram showing mean serum copper levels in groups with active disease and disease in remission
ESR was found to be elevated in cases with a mean level of 47.72±36.80mm at the end of 1st hour, which is very highly significant (p-value<0.001), whereas haemoglobin was found to be significantly lower in cases as compared to controls (p-value<0.01). An extremely significant difference in ESR at the end of the 1st hour (p-value<0.001) and, haemoglobin levels (p-value<0.0165) were found between the two groups i.e. cases of active disease and cases of disease in remission.
A very highly significant positive correlation (r=0.73, p<0.001) has been observed between Serum copper level and ESR and significant positive correlation (r=0.46, p<0.01) also has been noticed between serum copper level and morning stiffness. On the other hand, a significant negative correlation (r= -0.45, p<0.001) has been observed between serum copper level and haemoglobin.
Discussion
The distribution of cases were mostly clustered in the age group of 27-31 years (16%) followed by the age group of 37-41 years (14%) and 52-56 years (14%). 60% of the cases were between 25-50 years of age. Only 2 cases (4%) were seen in the age group beyond 61 years. The finding conforms to the observation made by ARA (1987) who reported the maximum age incidence between 25-30 years [1]. Similar age incidence was observed by Malaviya et al., in a study conducted by a house-house survey of a population near Delhi in 1993 [5].
In the present study there were 12 (24%) male cases and 38 (76%) female cases and the male: female ratio was 1:3.01. The findings coincide with those of ARA which states the ratio of male and female cases as 1:3. Kiss, lovei, et al., found similar results in a survey on rheumatoid arthritis patients in Hungary [17].
Serum copper level in this study was found to be significantly elevated in the cases as compared to control group. There was also highly significant difference in the serum copper level between active disease group and group in remission (p-value < 0.0001). These findings are similar to that of studies done by Xin L et al., Strecker D et al., and Shatha Rouf Moustafa et al., [12–14]. It might be attributed to the release of copper from its stores predominantly liver to maintain its increased requirement by lysyl oxidase, superoxide dismutase, glycylhistidine complex etc. [11]. Also, ceruloplasmin itself is said to have anti-inflammatory role. So an additional role is perhaps played by ceruloplasmin which is increased in rheumatoid arthritis as an acute phase protein.
The ESR was seen to be significantly elevated in cases as compared to control group. Among the case group again, patients in active disease, had a much higher level of ESR at the end of 1st hour as opposed to patients with disease in remission. The difference in the mean was extremely significant. Similar results were found by O. Cagayan et al., and Grennan D et al., [18,19]. In RA, fibrinogen, alpha 2 macroglobulin and immunoglobulins are increased which in turn helps in aggregation of RBCs and hence increased in ESR level [20].
Mean haemoglobin level in 50 patients of rheumatoid arthritis was significantly lower as opposed to that of control groups. Again those with active disease had a significantly lower haemoglobin level than in those with disease in remission (p<0.05), which implies that severity of Anaemia correlates with severity of the disease. Anaemia in rheumatoid arthritis may be due to decreased utilization of iron, reduced erythropoietin levels, premature destruction of red blood cells, NSAID associated Anaemia [21].
Very highly significant positive correlation (r=0.73, p<0.001) was observed between serum copper level and ESR and significant positive correlation (r=0.46, p<0.01) was also found between serum copper level and morning stiffness. On the other hand, a significant negative correlation (r= -0.45, p<0.001) has been observed between serum copper level and haemoglobin [Table/Fig-3].
Relation between Serum Copper Concentration and the following markers of disease activity
| Cases | No of patients | Correlation Coefficient | p-value |
|---|
| ESR | 50 | 0.73 | <0.001 |
| Haemoglobin | 50 | -0.45 | <0.01 |
| Morning Stiffness | 50 | 0.46 | <0.01 |
AG White et al., reported that serum copper level can be used as an index of erosive activity in rheumatoid arthritis [22]. Highly significant correlation was found between serum copper level and composite activity index criteria which among others includes haemoglobin, ESR, morning stiffness. (r=0.73, p<0.001).
Limitation
The limitation of our study includes less number of subjects involved in the study. Also, since liver is the store house of copper, estimation of hepatic tissue content of copper would have been a better indicator of actual amount of total body copper which could have helped in giving a direction towards treatment of rheumatoid arthritis, by supplementation of copper. Follow up study of disease activity with supplementation of copper could have revealed the role of copper more elaborately.
Conclusion
In the study we found that, serum copper level raises with the disease activity in RA; hence can be used as an alternative indirect marker to assess disease activity as well as severity in addition to the existing parameters.
[1]. Shah Ankur E, William St. Clair, Harrison’s Principles of Internal Medicine 2012 Volume 218th editionChapter 321 Rheumatoid Arthritis [Google Scholar]
[2]. Arend WP, Dayer JM, Cytokines and Cytokine inhibitors or antagonists in rheumatoid arthritisArthritis Rheum 1990 33:305-15. [Google Scholar]
[3]. Harris ED, Rheumatoid Arthritis. Pathophysiology and implications for therapyN Engl J Med 1990 322(18):1277-89. [Google Scholar]
[4]. Koch A E, Kunkel S L, Harlow L A, Johnson B, Evanoff H L, Haines GK, Enhanced production of monocyte chemoattractant protein-1 in rheumatoid arthritisJ Clin Invest 1992 90(3):772-79. [Google Scholar]
[5]. Malaviya AN, Kapoor SK, Singh RR, Kumar A, Pande I, Prevalence of Rheumatoid arthritis in the adult Indian PopulationRheumatol Int 1993 13(4):131-34. [Google Scholar]
[6]. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritisArthritis Rheum 1988 31(3):315-24. [Google Scholar]
[7]. Jacobson DM, Corinthian bronze and the gold of alchemists, Gold Bulletin 2000 33(2):60-66. [Google Scholar]
[8]. Grass G, Rensing C, Solioz M, Metallic Copper as an Antimicrobial Surface ApplEnviron Microbiol 2011 77(5):1541-47. [Google Scholar]
[9]. Milanino R, Marrella M, Gasperini R, Pasqualicchio M, Velo G, Cu and Zn body levels in inflammation: an overview of the data obtained from animal and human studiesAgents Actions 1983 39:195-209. [Google Scholar]
[10]. Gubler CJ, Lahey ME, Cartwright GE, Wintrobe MM, Studies on copper metabolism. IX. Transportation of copper in bloodJour. Clin. Investigations 1953 32:405-14. [Google Scholar]
[11]. Romero-Chapman N, Lee J, Tinker D, Uriu-Hare J Y, Keen C L, Rucker R R, Purification, properties and influence of dietary copper on accumulation and functional activity of lysyl oxidase in rat skinBiochem J 1991 275(Pt 3):657-62. [Google Scholar]
[12]. Xin L, Yang X, Cai G, Fan D, Xia Q, Liu Let al, Serum Levels of Copper and Zinc in Patients with Rheumatoid Arthritis: a Meta-analysisBiol Trace Elem Res 2015 [Epub ahead of print] [Google Scholar]
[13]. Strecker D, Mierzecki A, Radomska K, Copper levels in patients with rheumatoid arthritisAnn Agric Environ Med 2013 20(2):312-16. [Google Scholar]
[14]. Shatha Rouf Moustafa, Namir Al-Taweel, Fadhil Mohsen, Association of Boron, Copper, Germanium, Magnesium, Selenium and Zinc with Incidence of Rheumatoid ArthritisAmerican Journal of Internal Medicine 2015 3(3):132-140. [Google Scholar]
[15]. Bajpayee Davendra P, Significance of plasma copper and caeruloplasmin concentrations in rheumatoid arthritisAnn. rheum. Dis 1975 :34:162 [Google Scholar]
[16]. Abe A, Yamashita S, Noma A, Sensitive, direct colorimetric assay for copper in serumClin Chem 1989 35(4):552-54. [Google Scholar]
[17]. Kiss CG, Lovei C, Suto G, Varju C, Nagy Z, Fuzesi Z, Prevalence of rheumatoid arthritis in the South-Transdanubian region of Hungary based on a representative survey of 10,000 inhabitantsJ Rheumatology 2005 32(9):1688-90. [Google Scholar]
[18]. Oktay Caglayan, Aydog Y Sukro, Serum Zinc and Copper levels in rheumatoid arthritisJournal of Islamic Academy of Sciences 1997 10(1):19-24. [Google Scholar]
[19]. Grennan DM, Anderson JA, Kennedy AC, Mitchell W, Dick WC, Buchanan WW, Relation between haemoglobin and other clinical and laboratory parameter in rheumatoid arthritisCurr Med Res Opin 1975 3(2):104-08. [Google Scholar]
[20]. Youssef A, Wood B, Baron D N, Serum copper: a marker of disease activity in rheumatoid arthritisJ Clin Pathol 1983 36(1):14-17. [Google Scholar]
[21]. Peeters H R, Jongen-Lavrencic M, Raja A N, Ramdin H S, Vreugdenhil G, Breedveld F C, Course and characteristics of anaemia in patients with rheumatoid arthritis of recent onsetAnn Rheum Dis 1996 55(3):162-68. [Google Scholar]
[22]. White A. G, Scudder P, Dormandy T.L, Martin V.M, opper, an index of erosive activity?Oxford Journal of Medicine, Rheumatology 1978 17(1):3-5. [Google Scholar]