A Rare Combination of Ipsilateral Partial Talocalcaneal and Talonavicular Coalition
Raghavendra S Kembhavi1, Boblee James2
1 Assistant Professor, Department of Orthopaedics, Sree Lakshmi Narayan Institute of Medical Sciences, Pondicherry, India.
2 Professor and Head, Department of Orthopaedics, Sree Lakshmi Narayan Institute of Medical Sciences, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghavendra S Kembhavi, Plot no 8, Rajaannamalai Nagar, Behind Police Quaters, Pondicherry-605006, India.
E-mail: Kembhavi.raghavendra@gmail.com
Tarsal coalitions refer to fibrous, cartilaginous or osseous fusion between two tarsal bones. Commonly seen are talocalcaneal coalitions and calcaneonavicular coalitions. Talonavicular, calcaneocuboid and cubonavicular coalition are very uncommonly seen. Talocalcaneal and calcaneonavicular coalitions are generally symptomatic whereas talonavicular coalitions are asymptomatic. Special view radiography, CT and MRI will be helpful in diagnosing coalitions depending on nature of coalitions. In this case report, we present 24-year-old male patient with rare combination of talocalcaneal and talonavicular coalition on ipsilateral side. Patient also showed talar beak sign and arthritic changes at subtalar joint. Considering first time presentation to hospital and milder symptoms, we treated patient conservatively with short leg cast and foot orthoses. With course of treatment, symptoms were relieved significantly.
Cartilaginous, Middle facet, Orthoses, Osseous, Talar beak
Case Report
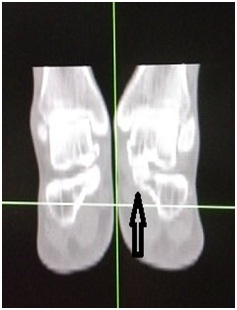
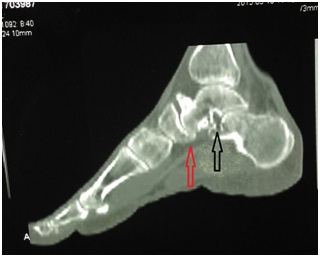
A 24-year-old male patient presented to our hospital with history of vague mild pain over hind foot and midfoot region though pain was mainly at hindfoot region over past one year. Pain used to increase on walking and relieves on rest. There was no history of prior trauma. None of his family members had similar complaints. Patient walked with minimal forefoot abduction but otherwise gait looked near normal. Physical examination showed minimal tenderness over talonavicular and subtalar joint, minimal palpable swelling over dorsal aspect of talonavicular joint, peroneal spasm and minimal loss of medial longitudinal arch when compared to other side. Range of movement was restricted at subtalar joint. No pain was seen in other joints. No obvious anamolies were seen in any other joints of the body and other foot appeared normal. Plain radiography of ankle lateral view showed ‘talar beak sign’ and mild reduction in posterior subtalar joint space [Table/Fig-1]. Oblique radiograph of foot showed bony coalition of talocalcaneal joint extending beyond middle facet towards anterior articular facet [Table/Fig-2]. Computed tomography (CT) coronal sections showed bony coalition (synostosis) of talocalcaneal joint at middle facet [Table/Fig-3]. Sagittal sections of foot showed bony coalition at inferomedial edge of talonavicular joint [Table/Fig-4]. It also showed arthritic changes in the subtalar joint with reduced joint space in posterior subtalar joint [Table/Fig-4]. Patient was treated conservatively considering milder nature of pain and non-disabling disease. Our treatment included short leg casting for ten weeks followed by foot orthoses with medial arch support, physical restriction and analgesics. With course of treatment over three months, patient was symptomatically better.
Lateral radiograph of left ankle showing talar beak (white arrow) and decreased posterior subtalar joint space (red arrow) which are secondary changes to talocalcaneal coalition

Oblique radiograph of foot showing extension of bony talocalcaneal coalition extending beyond middle facet into anterior articular facet

CT scan in coronal section showing talocalcaneal bony coalition at middle facet (arrow)
CT of foot in sagittal section shows arthritic changes in subtalar joint with reduction in posterior subtalar joint space (black arrow) and partial talonavicular coalition at inferomedial edge of the joint (red arrow)
Discussion
Tarsal coalitions are abnormal fusion of tarsal bones which can be bony, fibrous or cartilaginous [1]. Most congenital tarsal coalitions are bilateral. Tarsal coalitions most commonly seen are calcaneonavicular and talocalcaneal, which are seen in 90% of cases whereas talonavicular coalitions are very uncommonly seen. Further uncommon are calcaneocuboid and cubonavicular coalition. However, there have been no documented reports of cases with ipsilateral presentations of talocalcaneal and talonavicular coalition, even partial, as we noticed in this case.
Tarsal coalition are generally transmitted as autosomal dominant and also as autosomal recessive trait in some cases [2]. In our case there was no family history of similar complaints indicating probable autosomal recessive nature of coalition. At birth, tarsal coalitions are fibrous or cartilaginous and ossification may start in childhood [3]. Calcaneonavicular and talocalcaneal coalitions are symptomatic in most cases though many people remain asymptomatic in their life. Talonavicular coalitions are generally asymptomatic. However, they are associated with many other anamolies like clubfoot, symphalangism, clinodactyly and shorter great toe than second toe [2]. In our case, we did not find any of these associated anamolies. Most common symptoms shown are vague pain and stiffness at hindfoot. The reason for pain in coalitions could be progressive ossification during childhood. Repeated microfracture and stressing at coalition site on physical activity leads to progressive ossification which leads to increased rigidity and pain. Hence severity of pain depends on extent of ossification of coalition [4]. Loss of shock absorption feature also leads to pressure at surrounding joint which in turn can lead to pain. In our case, hind foot pain could be due to osseous talocalcaneal coalition and arthritic changes at subtalar joint. Pain and tenderness at talonavicular joint was probably due to bony protrusion formed by talar beak.
Coalitions are better seen in computed tomography when they are bony whereas fibrous or cartilaginous coalitions are better seen in magnetic resonance imaging. However, special view radiography too will help in detecting particular bony coalitions, for example, calcaneonavicular bony coalition are best seen in 45o internal oblique views. Talocalcaneal coalition is difficult to see in plane radiographs because of complex orientation of subtalar joint. However, secondary changes like talar beak, posterior subtalar joint space reduction, broadening of lateral process of talus as it impinges on calcaneal sulcus and lack of clear visualization of middle facet can be seen on plain radiographs. Talar beak formation is due to decreased subtalar motion resulting in overriding of talus on navicular bone secondary to talocalacaneal coalition. It is one of the indirect sign of talocalcaneal coalition [5]. In our patient too we had ‘talar beak sign’ which could have been secondary to talocalcaneal coalition. Another important radiological sign of talocalcaneal coalition is C-sign, which is formed by medial outline of dome of talus to posteroinferior aspect of sustentaculum tali on lateral ankle radiograph. However, presence of this sign is not always diagnostic of talocalcaneal coalition and absence of it does not rule out talocalcaneal coalition [6,7]. In our case, we did not find C-sign. CT scan particularly coronal sections will be helpful in better analysis of bony coalition in subtalar joint and also for proper surgical planning. It will also help in better visualization of degenerative changes which are subtle to see on plane radiography. Talocalcaneal coalition more commonly involves middle facet of subtalar joint near sustentaculum tali [8]. CT scan coronal section in our patient also showed talocalcaneal bony coalition at middle facet. Talonavicular coalition, which are very uncommon are better seen in CT. In our patient CT of foot in sagittal section showed partial talonavicular coalition at inferomedial edge of the joint. It also showed arthritic changes in subtalar joint with reduction in posterior subtalar joint space and probably it was one of the reason for hindfoot pain along with coalition.
Management of symptomatic talocalcaneal coalitions includes conservative treatment and surgical resection of coalitions. Conservative treatment would be sufficient in patients with less symptomatic patients [8]. It includes analgesics, cold compresses, foot orthoses, short leg casting and physical activity restriction [9]. In our patient too, considering milder nature of the pain and non-disabling disease, we decided for conservative management. Surgical resection can be done in patients with grossly symptomatic patients where it is disabling daily activities. Outcome of such surgeries have yielded good short term results though long term results are not fully known yet. Talonavicular coalition, since they are asymptomatic in most cases, surgery is rarely indicated. Pain in such conditions could be due to overload at calcaneocuboid joints. In our patient, pain at talocalcaneal region could be due to talar beak, which in turn is secondary to talocalcaneal coalition. Surgical resection of talar beak has also been described in literature in severe symptomatic cases [10]. However in our case, patient was more symptomatic on subtalar region than at talar beak and hence we did not try for surgical resection of talar beak.
Conclusion
Talonavicular coalitions are uncommonly seen. Ipsilateral talocalcaneal and talonavicular coalitions, even partial have not been reported in literature. Treatment depends on symptomatolgy and extent of ossification at coalition. Conservative treatment would be sufficient in mildly symptomatic patients as we found in this case.
[1]. Nalaboff KE, Schweitzer ME, MRI of Tarsal Coalition: Frequency, Distribution and Innovative SignsBulletin of the NYU Hospital for Joint Diseases 2008 66(1):14-21. [Google Scholar]
[2]. Migues A, Slullitel GA, Suárez E, Galán HL, Case reports: symptomatic bilateral talonavicular coalitionClin Orthop Relat Res 2009 467(1):288-92. [Google Scholar]
[3]. Jackson JF, Stricker SJ, Pediatric foot notes: a review of common congenital foot deformitiesInternational Pediatrics 2003 18(3):133 [Google Scholar]
[4]. Solomon L, Ruhli F, A dissection and computer tomography study on tarsal coalitions in 100 cadaver feetJ Orthopaedics and Related Research 2003 21(2):352-58. [Google Scholar]
[5]. Varich L, Bancroft L, Radiologic case study. Talocalcaneal coalitionOrthopedics 2010 2013:374-452. [Google Scholar]
[6]. Rozansky A, Varley E, Moor M, Wenger DR, Mubarak SJ, A radiologic classification of talocalcaneal coalitions based on 3D reconstructionJ Child Orthop 2010 4(2):129-35. [Google Scholar]
[7]. Taniguchi A, Tanaka Y, Kadono K, C sign for diagnosis of talocalcaneal coalitionRadiology 2003 228(2):501-05. [Google Scholar]
[8]. Mubarak S, Patel N, Upasani V, Moor M, Wenger D, Calcaneonavicular coalition: treatment by excision and fat graftJ Pediatric Orthopedics 2009 29(5):418-26. [Google Scholar]
[9]. Bohne W, Tarsal CoalitionCurrent Opinion in Pediatrics 2001 13:29-35. [Google Scholar]
[10]. Ozyurek S, Guler F, Turan A, Kose O, Symptomatic talar beak in talocalcaneal coalitionBMJ Case Rep 2013 2013:009309 [Google Scholar]