Decreased bony alveolus in vertical dimension is a common finding in patients going for prosthetic rehabilitation. They can result due to orofacial pathology, faciomaxillary injury or surgical procedures [1]. Preprosthetic surgery encompasses surgical manoeuvre for achieving an ideal bony and soft tissue contour for receiving a dental prosthesis [2]. Current modalities include autogenous grafting materials, guided bone regeneration, alloplastic grafting materials, etc. The recent advancement to this bone gaining procedure is callus distraction osteogenesis [3].
The science of distraction dates back to 1905 when Codvilla distracted the limbs. After that the science was passive till 1960s. Ilizarov then took for a more complete study of the process. In the following years it was used in facial region for animals and 20 years later on human beings [1]. Alveolar distraction osteogenesis was first reported by Chin and Toth in 1996 [4]. The principle involves an intentional osteotomy of the proposed area followed by traction force applied to the callus [1].
After its widespread use in facial bones, the process has been used in the alveolus of maxilla and mandible. The science could be applied to the alveolar bone because of the development of miniature distraction devices [3]. Alveolar distraction can be divided into two categories, in which bone is gained vertically (vertical distraction) and in which bone is gained horizontally (horizontal distraction). The indications for alveolar distraction osteogenesis are any acquired or congenital alveolar defects [3]. It is contraindicated in severely resorbed residual bony heights in either jaws [5].
The process of distraction avoids bone grafting procedures from other body parts and its associated complications. It has also an added advantage of recreation of soft tissues along with the hard tissues [3]. Complications associated with the procedure are malposed distracted segment, bone defects formation, fracture of transport segment and infections leading to failure [6].
In this study we present our experience in vertical alveolar ridge augmentation by distraction osteogenesis in patients reporting for dental rehabilitation but having a vertically deficient alveolus.
Materials and Methods
Patient selection
Ten patients aged 16 to 46 years with vertically deficient ridges [Table/Fig-1,2] underwent vertical augmentation using indigenously designed intraoral eccentric distractors in the Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University, Chennai, India.
Deficient maxillary alveolus

Deficient mandibular alveolus

The inclusion criteria were good general and physical health of the patient, severely resorbed ridges (class V-VI, Cawood and Howell 1988) and patients falling in ASA grade 1 and ASA grade 2 categories for general anaesthesia. Patients with previous history of radiotherapy in head and neck region or preprosthetic surgeries were excluded from the study.
Seven of the patients were post trauma cases, two were completely edentulous patients and one patient was a partially edentulous case. A detailed case history was taken including the patients motivation for the long term rehabilitation plan.
The patients were informed in detail about the treatment plan and consent was obtained. The study was conducted with the permission of the institutional ethics committee.
Distractor device
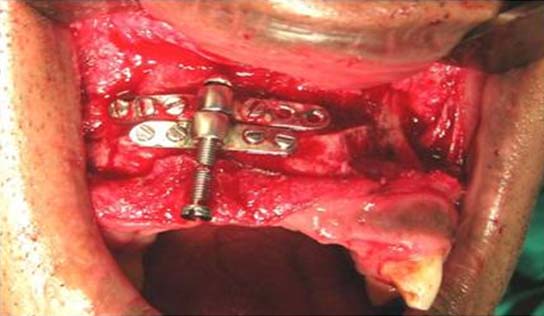
The device [Table/Fig-3] used for the purpose consisted of a screw and two 2mm miniplate fixed to the screw so that one miniplate was fixed and other miniplate could slide on the screw. The length of the bone plate is determined by the length of the segement to be distracted. The lower plate is called the base plate and the upper one is called the transport plate. The base plate is fixed to the alveolus and the transport plate to the transport segment. When rotation of the screw head is done, the transport plate glides along it, carrying with it the attached bony segment. The activation is done with the help of a screw driver. The distraction device was indigenously manufactured with SS-316 (ISO 3506). For each patient a custom made distraction device was fabricated. Variable length of the rod can be taken as per the augmentation required. We used length of 12mm and 15mm.

Five procedures were performed under general anaesthesia and five under local anaesthesia. The type of anaesthesia for the procedure was dependent on patient compliance, procedure time, surgical technique considerations and the amount of bone gain to be achieved. For patients under local anaesthesia complete blood count, serological markers were conducted and for patients under general anaesthesia pre-anaesthetic checkup and associated tests were done.
Surgical procedure
Face preparation was done with 5% povidone iodine and 2% xylocaine with adrenalin (1:80000) was administered over the planned incision site. Horizontal incision was placed at the junction of attached and free gingiva extending along the extent of the defect and a mucoperiosteal flap elevated. Vertical tunneling along margin of the defect was done superiorly to facilitate vertical osteotomy. Device was then adapted to the buccal cortex and reference osteotomy line scored. A 701 carbide bur was used to make two bony vertical cuts and a third one joining the two vertical cuts which was known as the horizontal cut. Using fine 5mm osteotome cuts were completed and segment mobilised. In this way the transport segment was created. Care was taken to place the vertical cuts in close vicinity to the tooth adjoining the edentulous space but giving due respect to the periodontal ligament space. In the mandible due care was taken not to injure the inferior alveolar nerve or the mental nerve. In the maxilla, the osteotomy cut was kept away from maxillary sinus and nasal cavity. The transport segment after the completion of osteotomy was checked for vertical translational movement without disturbing the crestal mucosa and the distractor was fixed [Table/Fig-4,5]. The wound was closed in layers, periosteal closure and mucosal closure. Due care was given for proper periosteal closure so that an ideal vicinity of distraction space is maintained for proper bony regeneration.

Prophylactic antibiotics (amoxicillin and clavulanate, 625mg-bd, 1 hour before surgery and was continued for five days postoperatively). When general anaesthesia was used, parenteral antibiotics were administered. This was supplemented with non steroidal anti-inflammatory drugs, proton pump inhibitors and mouthwashes. Following the procedure the patient was advised to have semi solid diet and maintain a fair oral hygiene.
Distraction protocol
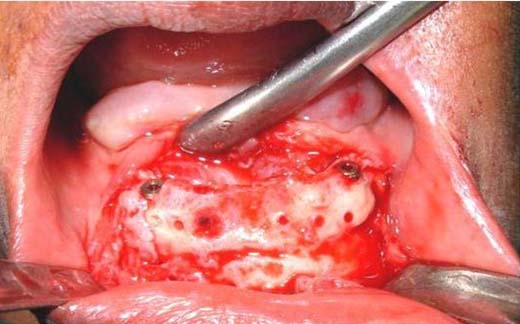
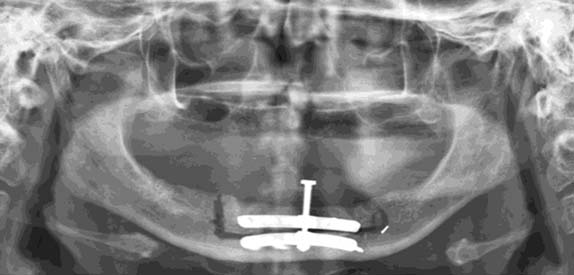
The distraction process was initiated on the fourth post operative day [3] with a frequency of twice daily. The pitch of the distractor screw was 0.5mm and hence vertical ridge augmentation was achieved at a rate of 1mm/day. The time period for distraction was dependent on the amount of augmentation planned. Following distraction a consolidation period of 3-5 months [7] was maintained and after which the device was removed [Table/Fig-6,7], followed by implants placement [Table/Fig-8,9] or conventional prosthesis. Orthopantamogram were taken one day before the starting of the distraction [Table/Fig-10,11], before removal of the distractor [Table/Fig-12,13] and after the placement of implants [Table/Fig-14,15]. An assessment of the quality of the regenerated bone was done by histological study post consolidation period and also by ultrasonogram.
Augmented ma xillary ridge

Augmented mandibular ridge

Implants placed in maxilla
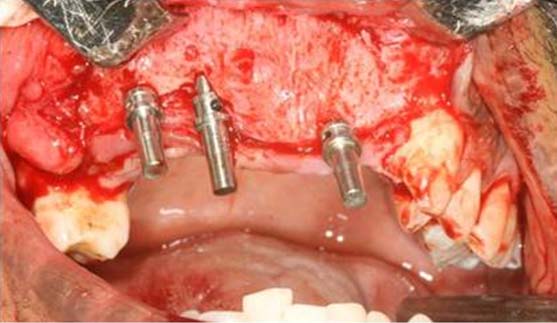
Implants placed in mandible
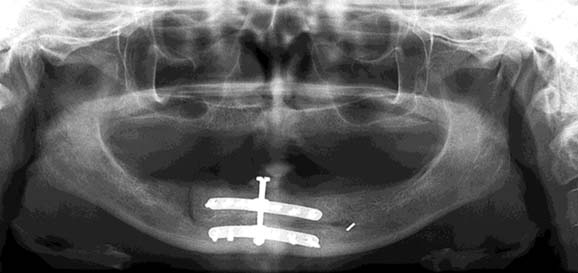
Orthopantomogram after distractor placement in maxilla

Orthopantomogram after distractor placement in mandible
Orthopantomogram post distraction in maxilla

Orthopantomogram post distraction in mandible
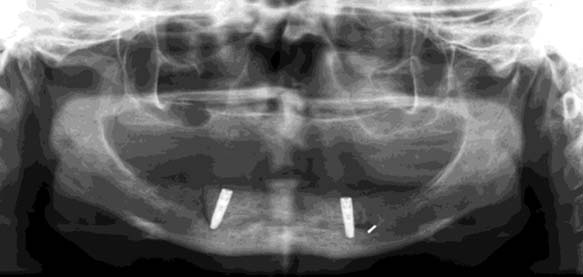
Orthopantomogram after implant placement in maxilla

Orthopantomogram after implant placement in mandible
Calculation of vertical bone gain
For calculating the actual height gained, Magnification Factor (MF) of the orthopantomogram had to be calculated. It was done by dividing the difference of Radiographic Length (RL) of the screw in the OPG and the Actual Length (AL) of the screw by the actual length of the screw and multiplying by 100. To obtain the vertical bone gain the length of the distractor pre activation (LD1) which consisted of the distance between the superior portion of the basal plate and superior portion of the transport plate was calculated substracting the magnification factor. The length of the distractor post activation (LD2) is obtained by the same method after three months.
The vertical bone gained was obtained by:
VERTICAL BONE GAIN: LD2-LD1.
Results
The vertical height achieved was clinically calculated summing the number of rotations performed with the activating device (every complete rotation was equal to 0.5 mm). Also, the gap between the miniplates attached to the screw of the distractor device was measured at the end of consolidation period. Dimensional distortion was corrected taking into account the magnification factor. The height gained in our study ranged from 6 mm to 11 mm. Complications such as incorrect vector of distraction, loss of transport segment, pain and paresthesia were encounterd. Incorrect vector was corrected by osteotomy and repostionining of the transport segment. Pain and paresthesia resolved with time.
Rehabilitation was feasible in the neoridges either in the form of regular prosthesis or with the help of implant supported prosthesis [Table/Fig-16,17]. There were no other complications including resorption in the follow up period.
After maxillary prosthetic rehabilitation

After prosthetic rehabilitation

Discussion
Alveolar ridge augmentation is a definitive pretreatment procedure for the correction of severely deficient alveolar bone. The procedure can be carried out under local anaesthesia and the postopertative period is usually uneventful. The bone formed is covered by crestal mucosa and does not resorb significantly with time. It is also strong enough to bear the mechanical forces of implant loading [8]. In our study 5 surgeries were carried out under local anaesthesia with good patient compliance.
Compared to vertical guided bone regeneration, distraction osteogenesis results in greater vertical bone gain thus permitting the correction of very relevant defects. Moreover, it can be successfully applied to extended defects such as total or partial edentulism [8]. In the present study too, a significant increase in height was obtained with the highest limit being 11mm [Table/Fig-18].
Augmentation achieved with location and follow-up.
| PatientNo. | Age(years) | Diagnosis | Location | Vertical augmentationachieved (mm) | Follow upafterdistraction (month) |
|---|
| 1 | 28 | Post trauma | 15 to 22 | 11 | 24 |
| 2 | 44 | Post trauma | 11 to 2733 to 41 | 116 | 18 |
| 3 | 16 | Post trauma | 13 to 21 | transport segment resorbed | 3 |
| 4 | 46 | Anodontia | Lower anterior mandible | 7 | 6 |
| 5 | 31 | Post trauma | 13to 21 | 7 | 4 |
| 6 | 35 | Post trauma | 11 to 23 | 8 | 6 |
| 7 | 40 | Anodontia | Lower anterior mandible | 5 | 5 |
| 8 | 35 | Post trauma | 12 to 24 | 7 | 6 |
| 9 | 40 | Anodontia | 32to 42 | transport segment resorbed | 7 |
| 10 | 28 | Post trauma | 12 to 23 | 7 | 6 |
With allogenic grafts there are high chances of infection. It also does not give a proper aesthetic value after the placement of implants. The allogenic material also does not have the strength to bear the implant load. Its use is also limited for augmentation of short span of alveolar ridges [9]. In our study there was no evidence of infection in the consolidation period and follow up. Aesthetics was also pleasing after the placement of implants.
Clinically the science of distraction consists of a osteotomy cut, latency period, distraction period, consolidation and remodeling [10]. In our study too we followed the same.
The latency period is the time from osteotomy to the starting of distraction [5]. Allowing for this latency period helps secure an endosteal revascularization potential for the mobilized segment that then participates in supporting matrix proliferation as distraction osteogenesis progresses [11]. Thus a guideline of 4 to 7 days latency seems justified as followed by Chin and Toth [4] in their study. In this study also a latency period of 4 days was chosen as followed by Chin and Toth.
The rate of distraction is ideal when it encompasses the principles needed in an ideal bone healing. Over enthusiastic distraction rate will result in non union and too slow distraction will result in early union [12]. Histological analysis by Li et al., reveals a rate as slow as 0.3mm/day do not have a stimulant potential on cell proliferation [13]. A rate of 0.7mm/day is optimal for cell proliferation but a higher rate of 1.3mm/day hampers physiologic tissue response during healing resulting in cell necrosis. Thus it is assumed that there should be a continuous distraction rate of 1mm/day in a rhythmic manner followed by consolidation period and then removal of the distraction device [12]. In our study rate of distraction was 1mm/day in accordance with the observation made by Li et al., [13]. The consolidation period is the time gap between stoppage of the distraction and removal of the distraction device. Tissue biopsies three months after distraction revealed woven bone interlaced with parallel fibered bone in a process of maturation but biopsy two months after showed more connective tissue matrix in the fibrous interzone. So to be on a safer side the consolidation period can be extended upto three months [7]. In the present study also we followed the same time period.
In this study we have used indigenous, custom made distraction devices with eccentric application. The primary advantage of this device as compared to endosseous and implant system is that it allows the clinician to have a good control over the distraction vector during surgery as reported by Zaffe D et al., in their study [1].
Alveolar distraction is a natural progression in the evolution of distraction technique [14]. The process of alveolar distraction has some complications namely difficulty in lingual cortical plate osteotomy, unfavourable fractures of bony segments, protrusion of the screw head in the oral cavity, wound dehisence, tilting of gained bone and bony defects as observed by Saulacic et al., [6]. In our study we too encountered incorrect vector of distraction, loss of transport segment and paresthesia.
Radiographically vertical movement of the transport segment could be appreciated with increase in gap between the two miniplates. Radiolucency was still observable in the distraction gap one month after distraction but with an increase in radioopacity. The use of computed tomography can add more precision for the assessment of the healing wound but it has a demerit of high cost and excessive radiation exposure. The metal distractor causes artifacts and gives an unclear picture of the distraction wound [15]. The outcome in terms of accuracy and surgical precision in the present study could have been enhanced by use of computed tomography and surgical simulation in a 3D model thus minimizing complications.
The limitations of the present study are its relatively small sample size and follow-up period.
Conclusion
Alveolar vertical distraction osteogenesis is a dependaple and predictable method for both hard and soft tissue genesis. The vertical bone gain reached more than 10 mm without the use of bone transplantation, thus reducing the morbidity with this technique. The bone gain reached at the end of distraction appeared to be lasting and the infection rate is extremely limited. Most of the complications confronted is easy to resolve. Implants placement is feasible with primary stability in neogenerated bone at the level of the distracted areas.