Infectious diseases are leading causes of morbidity and mortality in tropical countries. The term acute undifferentiated febrile illness (AUFI) connotes fever of <14 days duration without any evidence of organ or system specific aetiology [1]. In resource limited settings fever may be treated empirically or self treated due to lack of access to diagnostic tests. Thus, knowledge of local prevalence of infections is critical in order to target clinical work up and treatment [2]. There are only a limited number of studies from Northern India reporting on the aetiology of fever and reliable surveillance data are not available [3]. The main objective of this study was to describe the aetiology of fever among patients in a tertiary care hospital in Northern India.
Materials and Methods
This was conducted as a retrospective, observational study over a period of 12 months between December 2012 to November 2013 at Himalayan Institute of Medical Sciences, Swami Rama Himalayan University, Dehradun, India. The study included patients (age>18years) presenting with AUFI with oral temperature over 38.3oC within last 24 hours, duration of fever ranging from 5-14 days, no specific single organ involvement by history taking and physical examination, normal or non-specific results of the following investigations: complete blood count, thick film for malaria, urinalysis and chest roentgenogram. Diagnosis was confirmed by suitable laboratory tests after exhaustive clinical examination. Patients suffering from more than one infective aetiology were considered as mixed infection.
Laboratory tests
Tests had been ordered according to the discretion of the treating physicians and no additional tests were conducted for the purposes of the study. Blood cultures were processed through automated “Bactec 9120” (BD Diagnostics). Malaria was diagnosed with microscopy slides stained with Leishman stain (Fisher scientific) and/or antigen detection by rapid diagnostic kits (QDX). Further the following microbiological tests were used: Scrub typhus Detect IgM ELISA (InBios International, Inc, USA), Dengue Duo NS1/ IgM Cassette (SD Bioline), Leptospira IgM Cassette (SD Bioline), Widal Ag kit with titres of O≥80, H≥160 or four fold rise in titres (Febrile Antigen set, Span Diagnostics Ltd., Gujarat, India), Anti HEV IgM EIA (Diasorin, Italy) and Anti HAV IgM EIA (Diasorin, Italy).
Results
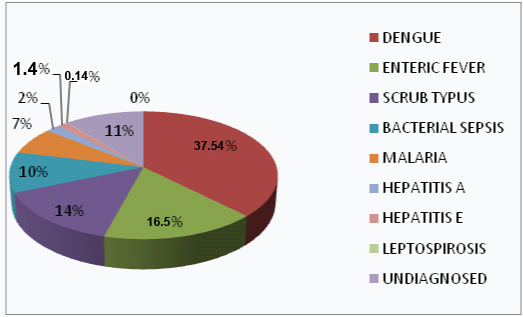
A total of 2547 patients with AUFI were evaluated. Of these, 1663(65.3%) were males and 884(34.7%) were females. Dengue (37.54%); enteric fever (16.5%); scrub typhus (14.42%); bacterial sepsis (10.3%); malaria (6.8%); hepatitis A (1.9%); Hepatitis E (1.4%); leptospirosis (0.14%); were the main infections while no specific diagnosis could be delineated in 11% as shown in [Table/Fig-1]. Mixed infection was noted in 48(1.88%) patients. Most common mixed infections were Dengue with scrub typhus (15 cases), Malaria with scrub typhus (11 cases) and malaria with dengue (8 cases). Three patients were diagnosed to be suffering from malaria with dengue with scrub typhus. Rest was one case each of different combination of urinary tract infection, malaria, dengue, enteric fever and hepatitis A infection.
Aetiological pattern of febrile patients (total no. =2547)
In our study, AUFI occurred most commonly during the months of August, September and October (56.1%) as shown in [Table/Fig-2]. These are the months of monsoon and post monsoon period.
The most common signs and symptoms, deranged laboratory parameters and duration of hospital stay of these febrile illnesses according to their aetiological agents are depicted in [Table/Fig-3].
Month wise distribution of adult febrile patients along with their aetiologies of common causes of fever
| Month | Dengue | Enteric Fever | Scrub Typus | Malaria | Total (%) |
|---|
| DEC’12 | 16 | 14 | 14 | 10 | 54(2.12) |
| JAN’13 | 1 | 4 | 3 | 0 | 8 (0.3) |
| FEB’13 | 1 | 15 | 5 | 0 | 21 (0.8) |
| MAR’13 | 1 | 18 | 0 | 1 | 20 (0.81) |
| APR’13 | 2 | 20 | 2 | 7 | 31 (1.2) |
| MAY’13 | 2 | 30 | 1 | 16 | 49 (1.3) |
| JUN’13 | 0 | 26 | 2 | 23 | 51 (2) |
| JUL’13 | 30 | 25 | 3 | 15 | 73 (2.9) |
| AUG’13 | 34 | 50 | 71 | 13 | 168 (6.5) |
| SEP’13 | 94 | 72 | 80 | 90 | 336(13.19%) |
| OCT’13 | 631 | 108 | 140 | 0 | 879 (34.5) |
| NOV’13 | 144 | 42 | 46 | 0 | 232 (9.1) |
| TOTAL | 956 (37.54%) | 424 (16.64%) | 367 (14.42%) | 175 (6.8%) | 1922 |
Clinical and laboratory parameters associated with common aetiological agents of AUFI
| Parameters | Dengue(n=956) | Enteric fever(n=424) | Scrub Typhus(n=367) | Malaria(n=175) |
|---|
| Days of hospitalization* | 5.4 ± 2.2 | 3.7 ± 1.4 | 8.5 ± 3.7 | 6.5 ± 5.4 |
| Clinical |
| Fever | 92.7 | 100 | 100 | 100 |
| Abdominal pain | 5.4 | 83.9 | 8.1 | 14.2 |
| Altered bowel habits | 2.9 | 70.7 | 4.0 | 11.4 |
| Bleeding | 5.7 | 0 | 0.8 | 0 |
| Lymphadenopathy | 6.0 | 0 | 10.0 | 0 |
| Icterus | 1.5 | 0 | 15.8 | 20 |
| Splenomegaly | 0.2 | 20.2 | 9.8 | 58.2 |
| Hepatomegaly | 16.6 | 9.9 | 19.6 | 61.7 |
| Rash | 83.6 | 0.2 | 6.2 | 0 |
| Haematological |
| Anaemia | 1.0 | 7.5 | 86.1 | 89.1 |
| Leucopenia | 92.9 | 60.3 | 12.2 | 65.7 |
| Thrombocytopenia | 92.0 | 28.7 | 29.9 | 54.2 |
| Biochemical |
| ALT | 57.0 | 59.9 | 51.4 | 31.4 |
| AST | 70.9 | 44.3 | 27.2 | 26.2 |
| ALP | 1.8 | 3.3 | 42.5 | 7.4 |
| Bilirubin | 15.1 | 2.8 | 48.2 | 8.0 |
| Albumin | 9.9 | 52.8 | 48.2 | 71.4 |
| Azotemia | 4.7 | 2.3 | 21.5 | 20.0 |
NOTE: All figures except * are mentioned in percentages; * mentioned as mean ± SD
Discussion
The study revealed the heavy burden of tropical infections such as dengue, enteric fever, scrub typhus and malaria. Previous studies in Northern and Southern parts of the country have shown the similar results [1,4,5]. A similar study conducted by Singh R et al., [6] from the region of Uttarakhand also showed that dengue, malaria, typhoid and enteric fever are the most common aetiological agents of acute febrile illness.
Males were affected twice as that of females. This may be due to their easy exposure to mosquitoes and mites because of their outdoor activities. In our study, AUFI occurred most commonly during monsoon and post monsoon seasons (56.1%) as shown in [Table/Fig-2]. For, mosquitoes and mites to breed and thrive, monsoon period is considered the best time. Drinking water is also contaminated during rainy season. All these factors lead to increase in above mentioned causes of fever in these particular months. Seasonal upsurge in fever is also a well known documentation in other studies [5,7,8].
Dengue, malaria, scrub typhus, enteric fever and leptospirosis have been identified as major causes of AUFI in Thailand, Malaysia and Nepal [7–11]. Various studies conducted particularly in South India by Chrispal et al., [5], Gopalakrishnan et al., [12], and Kashinkunti et al., [13] have also showed similar results.
In a cohort study by Abrahamsen et al., [14] from Southern India, bacterial infections (38%) and TB (19%) were the most common aetiological agents of fever. Another study from east India [15] reported that TB (53%), neoplasms (17%) and collagen vascular disorders (11%) were the dominant causes.
Mixed infection with more than one aetiological agent can result in an illness with overlapping symptoms, resulting in a situation where the diagnosis and management of such a patient could be challenging for the treating physician [16–20]. Symptoms of one disease may mimic with other disease which are also prevalent in this area. So, patients presenting with acute febrile illness should not be presumed to be suffering from single infection alone. The clinician should investigate thoroughly to look for other causes of fever.
Limitations
Limitations of the study were that it did not make an exhaustive search into all the causes of fever since viral studies are not available in our institute and it would have increased the cost to the patient. Secondly, the study included only adult patients while children would expect to have different fever aetiologies due to exposure and immunity. Hence, the pattern of fever aetiology found in this study would not be representative for the causes of fever in general population. Further, studies are needed, both community and hospital based including the adult as well as paediatric population in order to provide more evidence based information about the prevalence of aetiologies of fever in tropical country like India.
Conclusion
Our study clearly identified the major aetiologies of AUFI in this part of India. Dengue was the commonest cause of AUFI followed by enteric fever, scrub typhus and malaria. Active fever surveillance is necessary as clinical diagnosis is not always sufficient to detect all febrile cases. Laboratory confirmation is essential to refine disease burden estimates of common causes of AUFI. We would recommend establishing accurate epidemiologic database of different aetiologies of fever in every region to anticipate epidemic preparedness in terms of resources and health care delivery.
NOTE: All figures except * are mentioned in percentages; * mentioned as mean ± SD