Reduction of Complications of Local Anaesthesia in Dental Healthcare Setups by Application of the Six Sigma Methodology: A Statistical Quality Improvement Technique
Syed Akifuddin1, Farheen Khatoon2
1 Reader, Department of Oral and Maxillofacial Surgery, Daswani Dental College and Hospital Kota, Rajasthan, India.
2 Certified Six Sigma Black Belt, Director, Dentomax Dental and Maxillofacial Solutions, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Syed Akifuddin, Reader, Department of Oral and Maxillofacial Surgery, Daswani Dental College and Hospital Kota, Rajasthan-324005, India.
E-mail: akifuddinsyed@gmail.com
Background
Health care faces challenges due to complications, inefficiencies and other concerns that threaten the safety of patients.
Aim
The purpose of his study was to identify causes of complications encountered after administration of local anaesthesia for dental and oral surgical procedures and to reduce the incidence of complications by introduction of six sigma methodology.
Materials and Methods
DMAIC (Define, Measure, Analyse, Improve and Control) process of Six Sigma was taken into consideration to reduce the incidence of complications encountered after administration of local anaesthesia injections for dental and oral surgical procedures using failure mode and effect analysis. Pareto analysis was taken into consideration to analyse the most recurring complications. Paired z-sample test using Minitab Statistical Inference and Fisher’s exact test was used to statistically analyse the obtained data. The p-value <0.05 was considered as significant value.
Results
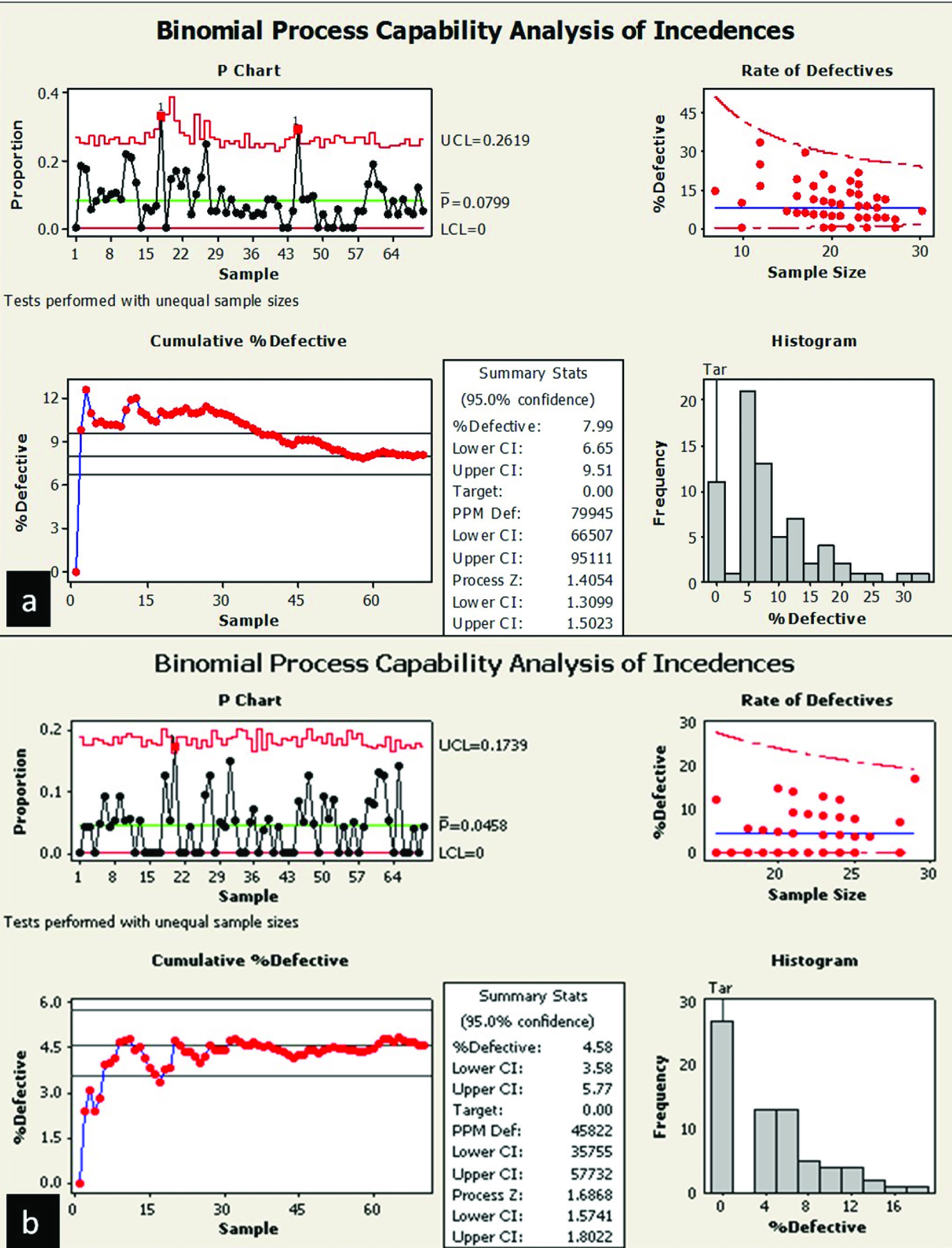
Total 54 systemic and 62 local complications occurred during three months of analyse and measure phase. Syncope, failure of anaesthesia, trismus, auto mordeduras and pain at injection site was found to be most recurring complications. Cumulative defective percentage was 7.99 in case of pre-improved data and decreased to 4.58 in the control phase. Estimate for difference was 0.0341228 and 95% lower bound for difference was 0.0193966. p-value was found to be highly significant with p= 0.000.
Conclusion
The application of six sigma improvement methodology in healthcare tends to deliver consistently better results to the patients as well as hospitals and results in better patient compliance as well as satisfaction.
Dentistry, Failure mode and effect analysis, Pareto analysis, Risk priority number
Introduction
Health care offers vast advancements in prevention, control and treatment of diseases but on the contrary also faces challenges due to complications, inefficiencies and other concerns that threaten the safety of patients [1]. People holding a position of authority, i.e. those who are responsible for the functioning of their department, institution, clinic, or a corporate hospital setup has a duty to monitor the output of quality of the health services provided in their respective setups, and to be able to do that, they must be well versed with methodologies employed to control quality.
The six sigma methodology is one of the quality improvement techniques for problem solving and process improvement. It was first developed by Motorola, a well known American telecom company [2]. Application of this methodology benefitted the company with a $16 billion profit in a 5 year span [3]. It is considered as a methodology of implementing Total Quality Management (TQM) and is an innovative approach to continue improvement process [4]. It was introduced as an improvement technique in manufacturing sector but later on due to success of projects, it was implemented to reduce shortcomings in various sectors including healthcare.
The use of these tools and techniques is guided by a structured improvement method known as DMAIC. This methodology constitutes five steps which stand for defining a problem or improvement opportunity, measure, analyse, improve and control [3]. The first phase defines who the customers are, their requirements, process capabilities and provides objectives for project-based improvement efforts. The second phase measures the quality characteristics that will lead to improvement in customer satisfaction and product performance and provides the metrics of data on which the improvement efforts will be based [4]. The third phase of this methodology is the analysis phase, this phase aims to evaluate data gathered in earlier phases of the study. This phase utilizes various analytical tools available such as Pareto analysis, regression analysis, fish-bone diagram, hypothesis testing, process flow diagram, tree-diagrams, statistical process control charts, etc., to identify the required plan and alterations to obtain performance objectives along with customer satisfaction. In the next phase i.e. improve phase, data collected and studied in previous phases is used to assign necessary modifications within the process with the aim of implementation of improvement to increase customer satisfaction and process profitability. The last phase, control phase monitors the process through quality management tools, compares data obtained during pre and post improvement phase and reveals the maintenance of performance improvement changes [5].
Literature has been published about successful implementation of DMAIC strategy in sectors of diagnostic imaging [6], emergency room [7], paramedic services [3], eye surgeries [8], radiology [2], etc. However, no study has been reported related to local anaesthesia complications in dentistry. Local anaesthesia is the reversible blockade of nerve conduction in a circumscribed area that produces loss of sensation [9]. It is the most frequently performed clinical procedure in any dental or oral surgical operatory and incidence of complications are definitely present [10]. Few studies [10–12] exist regarding the types of complications encountered and authors discuss their views regarding a specific complication.
In the present study, DMAIC methodology is taken into consideration to reduce the incidence of complications encountered when administering local anaesthesia injections for dental and oral surgical procedures, a common practice performed in all dental and oral surgical operatories. By doing so, it is intended to put forward the concept of six sigma, which once understood, can be applied as a improvement technique to all surgical situations.
Materials and Methods
The study was planned and conducted with the participation and conditional co-operation of the managements of five selected corporate dental healthcare providers in Hyderabad city. Ethical clearance was taken for the commencement of the study from the ethical committee of the institute. The inclusion criteria for the selection of study participants was dentists who performed an average of 4-9 outpatient local anaesthesia procedures per day, those who were willing to record and share the qualitative and quantitative data throughout the study period of 6 months and those who agreed to strictly implement the suggested ‘improve’ strategies. Any unusual event occurring during and after the injection was recorded on a chart provided along with the patient’s records. The DMAIC process was then charted. In the define phase of DMAIC, a team comprising of a maxillofacial surgeon and a dental surgeon with six sigma black belt qualification was assembled to initiate the process with a brainstorming session. SIPOC (Supplier, Input, Process, Output and Customer) table [Table/Fig-1] was framed for local anaesthesia administration process.
SIPOC (Supplier, Input, Process, Output and Customer) table for local anaesthesia administration process
| S | I | P | O | C |
|---|
| Supplier | Input | Process | Output | Customer |
| Doctors | Clinical signs | 1. Diagnosis2. Counselling3. Anaesthesia4. Procedure5. Discharge | Patient treated | Patient |
| Staff | Data recording | Safety Performed | Hospital Management |
| Patient | Verbal feedback | | |
In the measure phase the team determined the metrics to measure the existing process. The metrics chosen for the Six Sigma study were total number of local anaesthesia injections performed in the dental hospitals and number of complications of each type that occurred post injection. Complications that were not encountered at all were excluded. Data were collected for a period of three months [Table/Fig-2].
Complications encountered at during the study period of three months and analysis of the frequency of occurrence
| Systemic Complications |
|---|
| Sub category | Number of incidences | Percentage of incidences | Cum Percentage |
|---|
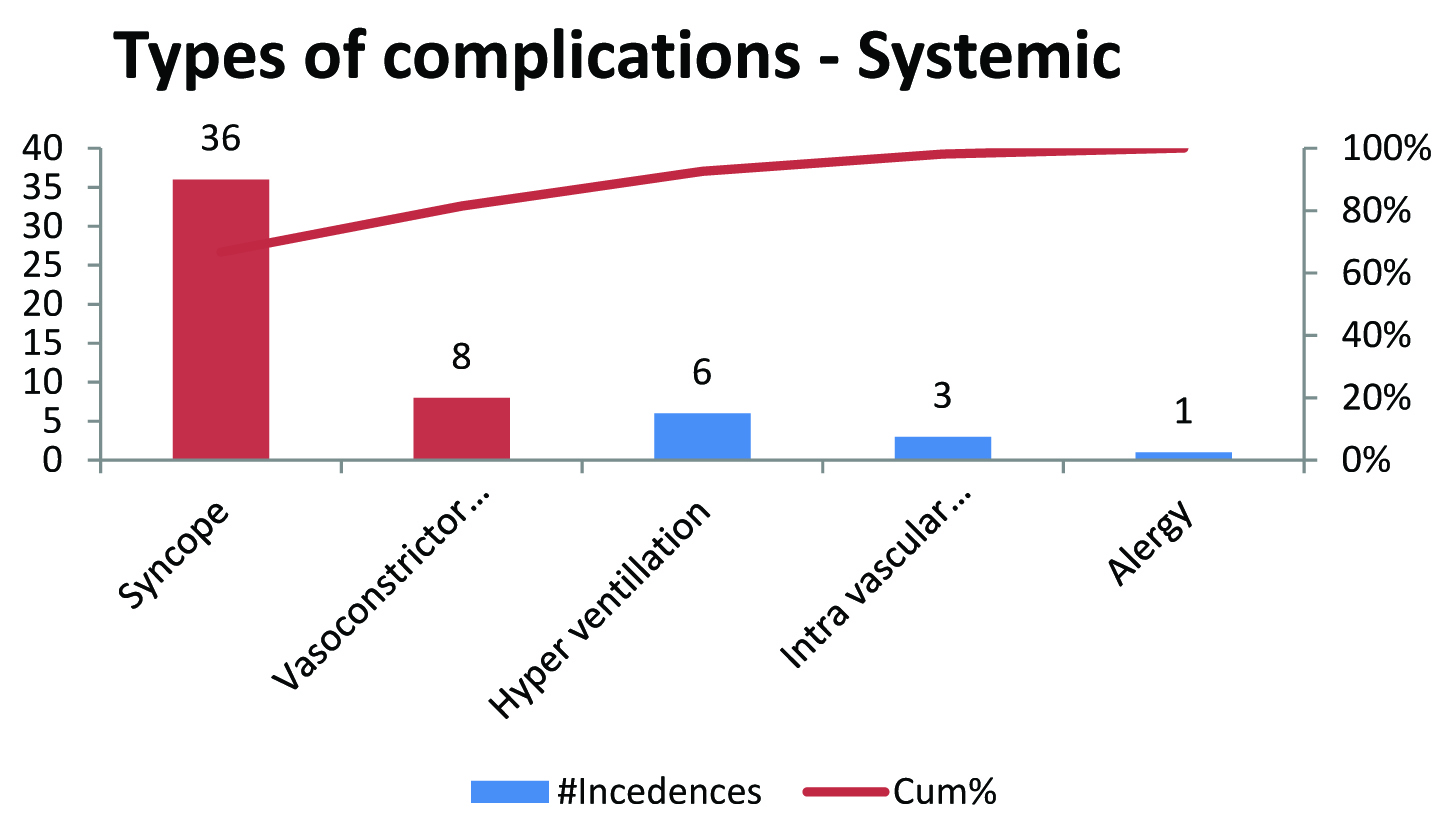
| Syncope | 36 | 67% | 67% |
| Vasoconstrictor Drug complication | 8 | 15% | 81% |
| Hyper ventillation | 6 | 11% | 93% |
| Intra vascular injection | 3 | 6% | 98% |
| Allergy | 1 | 2% | 100% |
| Local : Complications |
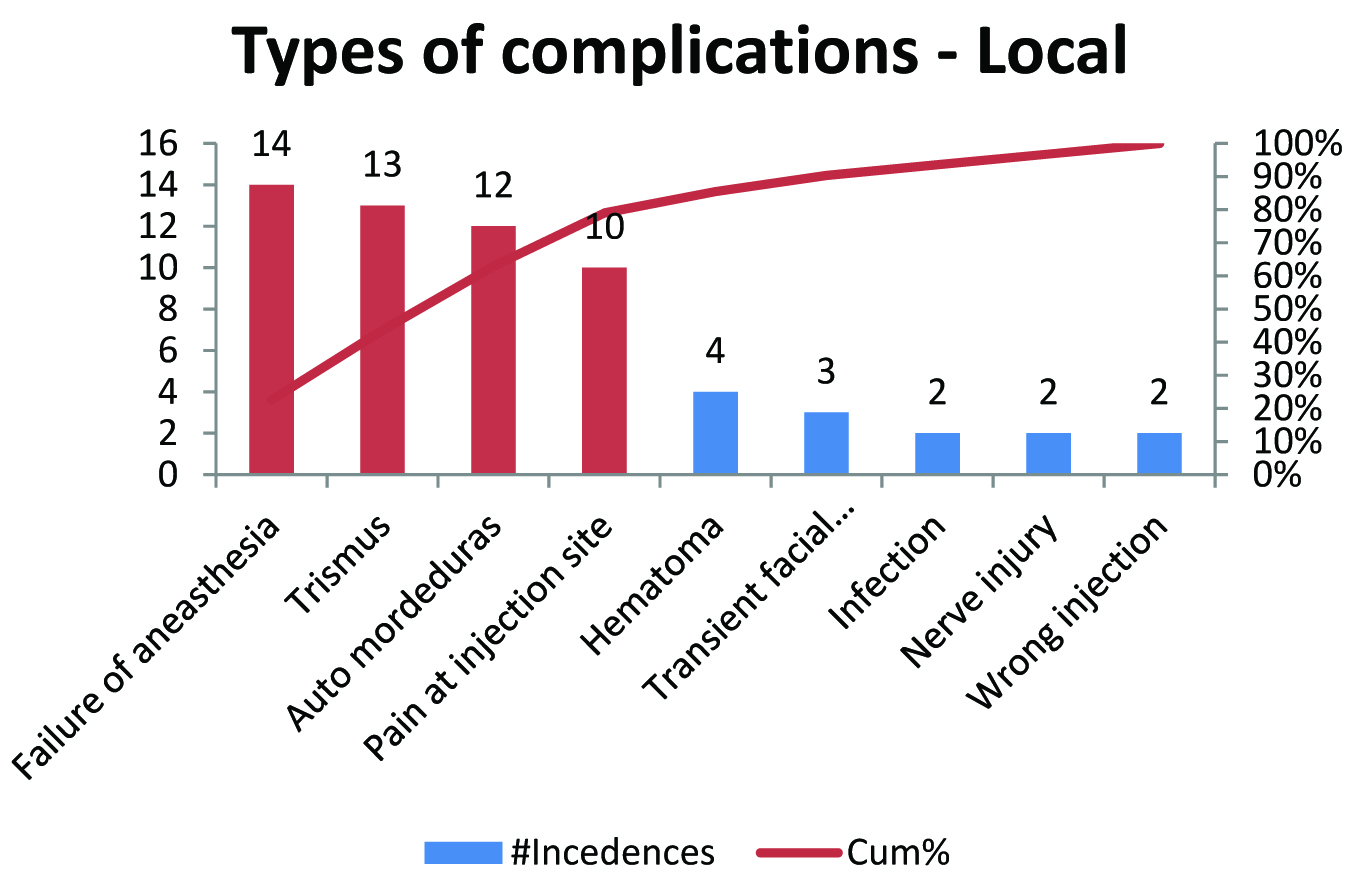
| Failure of aneasthesia | 14 | 23% | 23% |
| Trismus | 13 | 21% | 44% |
| Auto mordeduras | 12 | 19% | 63% |
| Pain at injection site | 10 | 16% | 79% |
| Hematoma | 4 | 6% | 85% |
| Transient facial paralysis | 3 | 5% | 90% |
| Infection | 2 | 3% | 94% |
| Nerve injury | 2 | 3% | 97% |
| Wrong injection | 2 | 3% | 100% |
In the third phase, analysis phase using Failure Mode and Effect Analysis (FMEA), the team analysed the frequency of occurrence of each complication in relation to their causes. Mode of failure and analysis of effects was carried out and risk priority number (RPN). RPN is a product of severity, occurrence and detectability. In the fourth phase, improvement phase, most recurring complications were taken into account. In the fifth phase, control phase analysis was carried out to find the improvement in the reduction of local anaesthesia complications by comparing the RPN data before and after the improve phase. Cumulative Distribution Function (CDF) was used to find Cumulative Defective Percentage. Pareto analysis was carried out to find the most recurring complications. Paired z-sample test using Minitab Statistical Inference and Fisher’s-exact test was used to statistically analyse the obtained data. The p-value <0.05 was considered as significant value.
Results
During the first three months of the study, first three phases of DMAIC i.e. define, measure and analysis was taken into account. Total 54 systemic and 62 local complications occurred [Table/Fig-2]. 36 cases of syncope, eight of vasoconstrictor drug complication, six of hyper ventilation, three of intra vascular injection and one of allergy out of total 54 systemic complications [Table/Fig-3] was notated. In case of local complications, failure of anaesthesia was found in 14 cases, trismus in 13, auto mordeduras in 12, pain at injection site in 10, haematoma in four, transient facial paralysis in three, infection, nerve injury and wrong injection in two cases [Table/Fig-4]. Pareto analysis was taken into account to find the most recurring complications. Syncope, failure of anaesthesia, trismus, auto mordeduras and pain at injection site was found to be most recurring complications [Table/Fig-5] and action was recommended to reduce RPN. Injection in supine position was recommended for syncope, use of Felipressin in place of adrenaline or limitation of adrenaline dose for vasoconstricter drug complication, training to identify land marks correctly in obese patients and management of infection preoperatively for failure of anaesthesia, create awareness to discard needle after every two to three injections for trismus, educate patient before giving LA for Auto mordeduras, modification of technique and use of topical anaesthesia for pain at injection site was recommended. RPN score in syncope patients with severity level 7 showed reduction from 112 to 84 and 64 to 48 in syncope patients with severity level 4. RPN score in vasoconstrictor drug complication patients with severity score 7 was reduced from 42 to 28 and from 30 to 20 with severity score 5. In case of failure of anaesthesia score was reduced from 70 to 50, in patients with trismus from 245 to 175, in case of auto mordeduras reduction was from 210 to 140 and pain at injection site RPN score showed reduction from 90 to 60 [Table/Fig-6]. Cumulative Defective Percentage was 7.99 in case of pre-improved data and it was found to be 4.58 in the control phase [Table/Fig-7]. Estimate for difference was 0.0341228 and 95% lower bound for difference was 0.0193966. p-Value was found to be highly significant with p= 0.000.
Pareto analysis of systemic complications
Pareto analysis of local complications
Failure Mode, Effect Analysis (FMEA) using Risk Priority Number (RPN) and recommended actions
| Failure Mode | Effect of failure | Severity(Low to High)1 - 10 | Potential cause | Occurrence(Low to High)1 - 10 | Detectability(Low to High)10 - 1 | RPN | Recommended action to reduce RPN |
|---|
| Syncope-fainting | Patient faints | 7 | Apprehensive patient | 8 | 2 | 112 | Injection in supine position |
| Syncope-faintness | Delays the service | 4 | Apprehensive patient | 8 | 2 | 64 | Injection in supine position |
| Vasoconstricter drug complication | Results in palpitation | 7 | Use of Vasoconstricter | 6 | 1 | 42 | Limit adrenaline dose |
| Vasoconstricter drug complication | Rise in BP | 5 | Use of Vasoconstricter | 6 | 1 | 30 | Limit adrenaline dose |
| Failure of aneasthesia | Pain | 5 | Wrong land mark, Presence of infection | 7 | 2 | 70 | Training to identify land marks correctly in obese patients and manage infection pre operatively |
| Trismus | Patient discomfort | 5 | Wrong technique, Presence of infection | 7 | 7 | 245 | Create awareness to discard needle after every two to three injections |
| Auto mordeduras | Patient discomfort | 5 | Patient not educated properly of post operative care | 6 | 7 | 210 | Educate patient before giving LA |
| Pain at injection site | Patient discomfort | 5 | Wrong technique | 6 | 3 | 90 | Modify technique and use of topical anaesthetic |
Comparison of RPN scores analysis phase and control phase
| Failure Mode | Effect of failure | Analysis phase | Improve phase | Control phase |
|---|
| Severity(Low to High)1 - 10 | Potential cause | Occurrence(Low to High)1 - 10 | Detectability(Low to High)10 - 1 | RPN | Recommended action to reduce RPN | Severity | Occurance | Detectability | RPN’ |
| Syncope | Patient faints | 7 | Apprehensive patient | 8 | 2 | 112 | Injection in supine position | 7 | 6 | 2 | 84 |
| Syncope | Delays the service | 4 | Apprehensive patient | 8 | 2 | 64 | Injection in supine position | 4 | 6 | 2 | 48 |
| Vasoconstricter drug complication | Results in palpitation | 7 | Use of Vasoconstricter | 6 | 1 | 42 | Use of Felipressin in place of adrenaline/limit adrenaline dose | 7 | 4 | 1 | 28 |
| Vasoconstricter drug complication | Rise in BP | 5 | Use of Vasoconstricter | 6 | 1 | 30 | avoid/limit adrenaline dose | 5 | 4 | 1 | 20 |
| Failure of anaesthesia | Pain | 5 | Wrong land markPresence of infection | 7 | 2 | 70 | Training to identify land marks orrectly in Obese patients and manage infection pre operating | 5 | 5 | 2 | 50 |
| Trismus | Patient Discomfort | 5 | Wrong techniquePresence of infection | 7 | 7 | 245 | Create awareness to discard needle after every two to three injections | 5 | 5 | 7 | 175 |
| Auto mordeduras | Patient discomfort | 5 | Patient not educated properly of post op care | 6 | 7 | 210 | Educate patient before giving LA | 5 | 4 | 7 | 140 |
| Pain at injection site | Patient discomfort | 5 | Wrong technique | 6 | 3 | 90 | Modify technique and use of topical anaesthetic | 5 | 4 | 3 | 60 |
Data showing Cumulative defective percentage pre and post-improvement phase
Discussion
Six sigma is a novel preface in the healthcare sector to identify the shortcomings within the process and thus provides opportunities to deal with the challenges encountered by this sector [1]. It is a business or trade performance improvement strategy launched by Motorola company that intends to reduce errors or shortcomings within the business process to as low as 3.4 occasions per million opportunities. Thus, in the healthcare, it can be described as a planned methodology to enhance hospital profitability along with increase and improve patient compliance and satisfaction by launching statistical tools and improving hospital management that can lead to patient safety, and quality treatment [4,13].
The present study was undertaken to identify the most frequently occurring incidences after administration of oral local anaesthesia followed by specific remedial measures and plans to implement the measures which resulted in reduction of number of incidents. The method selected to analyse the most recurring complications was Pareto analysis. Pareto Analysis is a simple method for prioritizing possible measures by identifying the problems that will be resolved by making the required changes. It is based on the Pareto Principle, also known as 80/20 rule which states that 20 percent of causes generate 80 percent of results [14]. In Pareto Analysis, a vertical bar chart with causes on the x-axis and number of occurrences on the y-axis is designed and bar chart is arranged in descending order of cause importance, that is, the cause with the highest count first. The cumulative count for each cause is calculated in descending order by the formula {Individual Cause Count}/{Total Causes Count}x100). A line is drawn at 80% on the y-axis consecutively parallel to the x-axis and this line falls at the point of intersection with the curve on the x-axis. This point of intersection on the x-axis separates the important reasons on the left (vital few) from the less important reasons on the right (trivial many) [15].
In the present study, the pre and post data of the most recurring causes was compared using Risk Priority Number (RPN). It was found to be decreased during the control phase after failure mode effect analysis and implementation of required measures during the improve phase. The RPN score is obtained by the multiplication of occurrence of incidence, severity score and incidence detectability. This score helps to find out critical failure modes and evaluates the risk related with the procedure [16] Baddour AA et al., conducted a study to reduce the incidence of needle stick injuries in healthcare workers utilising six sigma methodolgy and concluded this strategy as an effective method in cause reduction [3]. Kuo AM et al., carried out a study using six sigma system for postanaesthesia care unit workflow improvement and revealed that the new method decreased and improved the service gaps between health care providers and patients as well as balanced the requirements of health care managers and delivered health care services to patients by utilizing the six sigma high-quality principles [17]. Karen R et al., initiated a Cancer Service Line Patient Flow Project using the DMAIC process of Six Sigma to improve patient flow and reduce delays and found that before the initiation of project, 29% of the treatments started within 22 minutes, however after implementing the changes, this increased to 78% [18]. Khan V analysed outpatient waiting time and patient satisfaction due to presence of agitated patients and staff complains in the hospital [2]. The author concluded that application of Six Sigma was utilized to pinpoint the delays and helped to retrieve alternative methods to improve management capabilities. Bucci RV et al., carried out a study at Akron’s Hospital in northeast Ohia utilizing lean six sigma and concluded that methodology resulted in improved employee morale, increased employee involvement, improved imaging quality of MRI, decreased patient waiting time as well as reduced patient complains [19]. Thus, the studies available in the literature and also the present study demonstrates that the application of six sigma improvement methodology in healthcare tends to deliver consistently better results to the patients and hospitals. The limitation of the study is that however the present study succeeded in reducing the complications encountered due to administration of local anaesthesia but it might not be practically possible to go below this figure as this is a biological process, which allows us only a limited degree of control. Application of this methodology can be considered in occupational hazards to healthcare professionals, surgical safety, wound infections, surgical complications, patients waiting time, professional manpower utilization, operation theatre turnaround time, material management, etc.
Conclusion
The present study concludes that identification of cause to problem helps in reduction of risk of complication. The most frequently occurring incidences after administration of oral local anaesthesia was reduced after identification of causes followed by specific remedial measures and implementation of plans to reduce number of incidents. The scope is unlimited, six sigma can provide solution to all problems. This methodology acts as a bird’s eye towards better patient fulfilment and to increase hospital profitability. Thus, the application of six sigma improvement strategy in healthcare sector tends to deliver consistently better results to the patients as well as hospitals and results in better patient compliance as well as satisfaction.
[1]. Taner MT, Sezen B, Antony J, An overview of six sigma applications in healthcare industryInternational Journal of Health Care Quality Assurance 2007 20(4):329-40. [Google Scholar]
[2]. Khan V, Marose RA, Improving radiology out-patient registration process using six sigma methodologyProceedings for the Northeast Region Decision Sciences Institute 2013 :980Available at: www.nedsi.org/proc/2013/proc/p121126002.pdf [Google Scholar]
[3]. Baddour AA, Saleh HA, Use six sigma approach to improve healthcare workers safetyInternational Journal of Pure and Applied Sciences and Technology 2013 18(1):54-68. [Google Scholar]
[4]. Desai TN, Shrivastava RL, Six sigma- a new direction to quality and productivity managementProceedings for the World Congress on Engineering and Computer Sciences 2008 [Google Scholar]
[5]. Bandyopadhyay JK, Coppens K, Six sigma approach to healthcare quality and productivity managementInternational Journal of Quality and Productivity Management 2005 5(1):1-13. [Google Scholar]
[6]. Patrick J, Puterman ML, Improving resource utilization for diagnostic services through flexible inpatient scheduling: a method for improving resource utilizationThe Journal of the Operational Research Society 2007 58(2):235-45. [Google Scholar]
[7]. Fieri M, Ranney NF, Schroeder EB, Van Aken EM, Stone AH, Analysis and improvement of patient turnaround time in an Emergency DepartmentSystems and Information Engineering Design Symposium (SIEDS) IEEE 2010 :239-44. [Google Scholar]
[8]. Jin X, Lim SY, A simulation based analysis on reducing patient waiting time for consultation in an outpatient eye clinicProceedings of the 2013 Winter Simulation Conference:2192-203. [Google Scholar]
[9]. Ogle OE, Mahjoubi G, Local anaesthesia: agents, techniques, and complicationsDent Clin North Am 2012 56(1):133-48. [Google Scholar]
[10]. Kaufman E, Goharian S, Katz Y, Adverse reactions triggered by dental local anaesthetics: A Clinical SurveyAnaesth Prog 2000 47:134-38. [Google Scholar]
[11]. Daublander M, Muler R, Lipp MDW, The incidence of complications associated with local anaesthesia in dentistryAnaesth Prog 1997 44:132-41. [Google Scholar]
[12]. Lustig JP, Zusman SP, Immediate complications of local anaesthetic administered to 1007 consecutive patientsJ Am Dent Assoc 1999 130:496-99. [Google Scholar]
[13]. Venera TA, Doru C, Tiberiu T. Six Sigma and the Continuous Improvement of the dental medical services quality. Proceedings of the 5th WSEAS International Conference on Economy and Management Transformation. 2010:604–09 [Google Scholar]
[14]. Pareto Analysis. Using the 80:20 rule to prioritize. Available at: http://www.mindtools.com [Google Scholar]
[15]. Haughey D. Pareto Analysis Step by Step. Available at: http://www.projectsmart.co.uk/pareto-analysis-step-by-step.php [Google Scholar]
[16]. FMEA RPN Guide for FMEA information and resources. Available at: http://www.fmea-fmeca.com/fmea-rpn.html [Google Scholar]
[17]. Kuo AM, Borycki E, Kushniruka A, Lee TS, A healthcare Lean Six Sigma System for postanaesthesia care unit workflow improvementQual Manag health care 2011 20(1):4-14. [Google Scholar]
[18]. Karen R, Deb D, The oncology service line’s use of six sigma in the cowdery patient care center: creating standardized processes to improve patient flow, improving staff and patient satisfactionOncology Nursing Forum 2007 34(2):524 [Google Scholar]
[19]. Bucci RV, A lean six sigma journey in radiologyRadiology management 2011 33(3):27-33. [Google Scholar]