Prenatal Diagnosis of Tectocerebellar Dysraphia with Occipital Encephalocele
Hakan Timur1, Cem Y Sanhal2, Aytekin Tokmak3, Kamil H Müftüoglu4, Nuri Danisman5
1 Perinatology Assistant, Department of Obstetrics and Gynecology, Division of Perinatology, Health Research and Education Hospital, Ankara, Turkey.
2 Perinatology Assistant, Department of Obstetrics and Gynecology, Division of Perinatology, Health Research and Education Hospital, Ankara, Turkey.
3 M.D, Department of Obstetrics and Gynecology, Division of Perinatology, Health Research and Education Hospital, Ankara, Turkey.
4 Pathology Specialist, Zekai Tahir Burak Women’s, Department of Obstetrics and Gynecology, Division of Perinatology, Health Research and Education Hospital, Ankara, Turkey.
5 Perinatology Specialist, Assoc. Prof, Zekai Tahir Burak Women’s, Department of Pathology, Division of Perinatology, Health Research and Education Hospital, Ankara, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hakan Timur, (Institutional): Talatpasa Boulevard, No:75, Hamamönü, Altındag, 06230 Ankara, Turkey. E-mail : drhakantimur@gmail.com
Tectocerebellar dysraphia (TCD) is an extremely rare disorder and comprises the congenital abnormalities including occipital encephalocele, aplasia and/or hypoplasia of cerebellar vermis and deformity of tectum. Only few reported cases of this entity are there in the literature. However, the diagnosis in each of the previous cases had been made after birth. We herein describe the first reported case of prenatal diagnosis for TCD in a Turkish woman.
Cerebellar vermis, Deformity of tectum, Hypoplasia
Case Report
A 23-year-old woman, gravida 1, para 0, was referred to our perinatology unit at 18 weeks’ gestation for ultrasonography, with the suspicion of cranial abnormality. Her personal and family histories were unremarkable, and she had a nonconsanguineous marriage. She did not report any medication use, had no history of fever (with or without rash), ionizing radiation exposure during the first trimester.
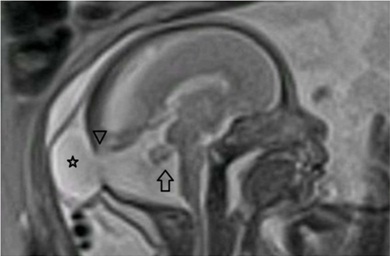
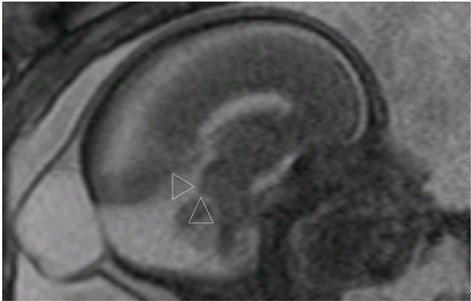
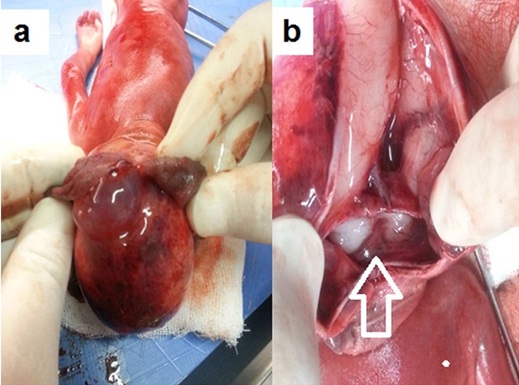
On grayscale sonography a bone defect at the occipital region and a 24x23x17 mm encephalocele associated with the large posterior fossa was detected [Table/Fig-1]. Mild lateral ventriculomegaly (13 mm) and inferior vermian agenesis were the other findings. Magnetic Resonance Imaging (MRI) of the fetal brain was requested following genetic amniocentesis. Two weeks later, MRI revealed that the tentorium and position of the torcular herophili were both elevated [Table/Fig-2]. Tectal distortion and beaking were also noted [Table/Fig-3]. Cavum septum pellucidum, corpus callosum was normal and transcerebellar length was 22 mm. No other congenital malformations were visualised. The prenatal diagnosis was tectocerebellar dysraphia (TCD) with occipital encephalocele. Based on the findings of TCD with occipital encephalocele in the fetus by prenatal ultrasound screening and MRI, the parents were informed about the anomalies. It was told that repeated surgical interventions with poor prognosis may be required for the fetus, and termination of the pregnancy was recommended. The couple chose the termination of pregnancy after our counseling about the postnatal prognosis of TCD. The use of vaginal prostaglandin E1 analogue was successful for the pregnancy termination. A female fetus weighing 340 gm, 17.5 cm in length was delivered. The diagnosis was confirmed on the postmortem examination and there was no karyotype anomaly (46, XX). At the autopsy, a smooth surface, broad based, soft cystic mass about 2 cm in diameter was detected in the back of the skull. When the sac was incised, absence of the cerebellar vermis and partial absence of the tectum, a large ventriculus quartus communicating with the occipital menigocele sac and an occipital bone defect were noted. The other parts of meninges and brain, cranial nerves and their lengths were all in normal appearance. There were also no features of facial dysmorphism and other congenital anomalies [Table/Fig-4]. The couple was counseled for future pregnancies to be evaluated properly for the same condition.
Bone defect at the occipital bone and encephalocele (asterisk) associated with the posterior fossa. Inferior vermis is absent

Occipital encephalocele (asterisk), elevated torcular herophili (arrowhead) and inferior vermian agenesis (arrow) on T2-weighted image of MRI
Tectal beaking (arrowheads) on T2-weighted image of MRI.
(a) Autopsy denoting encephalocele. (b) Inferior vermian agenesis (arrow)
Discussion
Tectocerebellar dysraphia (TCD) was initially described by Padget and Lindenberg in 1972 as ‘inverse cerebellum with occipital encephalocele’ [1]. In 1978, Friede suggested a new clinico-pathological entity apart from Dandy Walker syndrome and constituted the term ‘tectocerebellar dysraphia with occipital encephalocele’. According to this definition encephalocele, aplasia or hypoplasia of cerebellar vermis and tectal deformity are the main components [2]. A definitive cause for this entity is still undefined. Encephalocele, as being one of the major components, may point a failure in the closure of neural tube and neuropores during embryogenesis around the days 33 to 44 of gestation [3,4]. Moreover, it was hypothetically suggested that TCD could be one of the steps of the spectrum from Dandy-Walker malformations to Chiari type II [1].
Beside the major components, TCD may be accompanied with aplasia of mammillary bodies, fusion of thalami, anomalies of cerebral gyral patterns, bifid atlas, bulky basal ganglia, cervical hydromelia and congenital heart disease [1,2,5,6].
Unfortunately, the reported morbidity of TCD is extensive and episodic tachypnea, irregular breathing, opsoclonus, ataxia, marked hypotonia of the extremities, polydactyly, coloboma, unfavourable neurologic development and perinatal-postnatal mortality could be the clinical manifestations. The prognosis is usually poor if hydrocephalus is severe [7,8]. On the other hand, excellent neurological prognosis at the 4-year follow-up of a case with TCD and solely vermian encephalocele was reported after the surgical repair of a 5-month-old girl [9].
Like in TCD, occipital encephalocele was described as a component of some other genetic syndromes. However, the triad of occipital encephalocele, polycystic kidneys and postaxial polydactyly in Meckel-Gruber, phocomelia, radial ray defects and urogenital anomalies in Von Voss and agyria together with retinal dysplasia in Walker Warburg syndrome enables the performance of the correct differential diagnosis [10]. Recently, Poretti et al., investigated the relation between TCD with occipital encephalocele and Joubert syndrome [11]. They reported that similar findings as molar tooth sign in MRI, absence of the midbrain decussation of the superior cerebellar peduncles in colour-coded fractional anisotropy and homozygous mutation within the TMEM237 gene may reveal that TCD with occipital encephalocele may represent as a structural manifestation within Joubert syndrome and related disorders spectrum.
Conclusion
In conclusion, we want to emphasize that the prenatal diagnosis of TCD with occipital encephalocele could be performed with ultrasonography and MRI. The couple in this case report chose the termination of the pregnancy because of the potential poor prognosis due to the size of the encephalocele sac, inferior vermian agenesis and ventriculomegaly. Every effort should be made in the cases with occipital encephalocele for the accurate prenatal diagnosis, counseling and management choices.
[1]. Padget DH, Lindenberg R, Inverse morphogenetically related to Dandy-Walker and Arnold-Chiari syndromes: bizarre malformed brain with occipital encephaloceleJohns Hopkins Med J 1972 131:228-46. [Google Scholar]
[2]. Friede RL, Uncommon syndromes of cerebellar vermis aplasia. II: Tecto-cerebellar dysraphia with occipital encephaloceleDev Med Child Neurol 1978 20:764-72. [Google Scholar]
[3]. Lemire RJ, Loeser JD, Lecch RW, Elsworth CA, Cerebellum in Normal and Abnormal Development of the Human Nervous System 1975 Hagerstown, MDHarper and Row:144-63. [Google Scholar]
[4]. Nakatsu T, Uwabe C, Shiota K, Neural tube closure in humans initiates multiple sites: evidence from human embryos and implications for the pathogenesis of neural tube defectsAnat Embryol 2000 201:455-66. [Google Scholar]
[5]. Naidich TP, Altman NR, Braffman BH, McLone DG, Zimmerman RA, Cephaloceles and related malformationsAJNR Am J Neuroradiol 1992 13:655-90. [Google Scholar]
[6]. Krishnamurthy S, Kapoor S, Sharma V, Prakash A, Tectocerebellar dysraphia and occipital encephalocele: an unusual association with abdominal situs inversus and congenital heart diseaseIndian J Pediatr 2008 75:1178-80. [Google Scholar]
[7]. Chowdhary UM, Ibrahim AW, Ammar AS, Dawodu AH, Tecto-cerebellar dysraphia with occipital encephaloceleSurg Neurol 1989 31:310-14. [Google Scholar]
[8]. Agrawal A, Joharapurkar SR, Khan AU, Tecto-cerebellar dysraphia manifesting as occipital meningocoele associated with congenital melanocytic nevi and pectus excavatumIran J Pediatr 2010 20:118-22. [Google Scholar]
[9]. Anik I, Koc K, Anik Y, Yildiz DK, Ceylan S, Tectocerebellar dysraphism with vermian encephaloceleJ Child Neurol 2010 25:1411-14. [Google Scholar]
[10]. Wininger SJ, Donnenfeld AE, Syndromes identified in fetuses with prenatally diagnosed cephalocelesPrenat Diagn 1994 14:839-43. [Google Scholar]
[11]. Poretti A, Singhi S, Huisman TA, Meoded A, Jallo G, Ozturk A, Tecto-cerebellar dysraphism with occipital encephalocele: not a distinct disorder, but part of the Joubert syndrome spectrum?Neuropediatrics 2011 42:170-74. [Google Scholar]