Bilateral Multiple Variations in Carotid Arteries-A Case Report
Sulabha Hanumant Deshpande1, Ashwini Balasaheb Nuchhi2, Balappa Murigeppa Bannur3, Babasaheb Gurusiddappagouda Patil4
1 Assistant Professor, Department of Anatomy, BLDEU’s Shri B M Patil Medical College, Hospital Research Centre, Vijaypur, Karnataka, India.
2 Assistant Professor, Department of Anatomy, BLDEU’s Shri B M Patil Medical College, Hospital Research Centre, Vijaypur, Karnataka, India.
3 Professor and Head, Department of Anatomy, BLDEU’s Shri B M Patil Medical College, Hospital Research Centre, Vijaypur, Karnataka, India.
4 Professor, Department of Anatomy, BLDEU’s Shri B M Patil Medical College, Hospital Research Centre, Vijaypur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sulabha Hanumant Deshpande, Assistant Professor, Department of Anatomy, BLDEU’s Shri B M Patil Medical College, Hospital Research Centre, Vijaypur-586103, Karnataka, India. E-mail : drsulabhahd@gmail.com
The common carotid arteries are the largest bilateral arteries of the head and neck. The common carotid arteries may bifurcate higher or lower than the usual levels. A higher bifurcation is more common. Tortuous arteries if present may be asymptomatic if it is mild but may lead to ischaemia of the organs if severe. The cause could be genetic, or may be thickening of the arteries. During routine dissection of an adult male cadaver in the department of Anatomy, BLDEU’s Shri BM Patil Medical college, Vijaypur, we found the bilateral multiple variations in the carotid arteries regarding the bifurcation level of common carotid arteries, tortuous external and internal carotid arteries and the number of branches arising from external carotid arteries. The knowledge of such variations of carotid arteries is of great importance in radiological examinations especially per cutaneous carotid angiography. It is necessary to understand the anatomy of these vessels and its variations to carry out surgeries with minimum complications.
Higher bifurcation, Supernumerary, Tortuous, External carotid artery, Internal carotid artery
Case Report
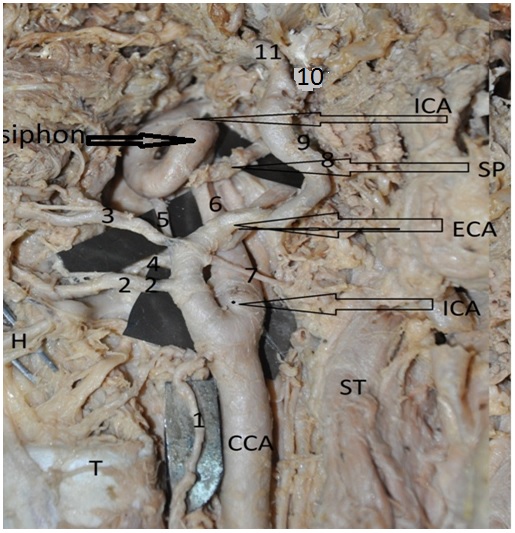
During routine dissection of an adult male cadaver, we found the following bilateral multiple variations in the carotid arteries. The left common carotid artery [Table/Fig-1] bifurcated at the level of hyoid bone. The right [Table/Fig-2,3] bifurcated in between the upper border of thyroid cartilage and hyoid bone. We found both the external and internal carotid arteries were tortuous in their course. The internal carotid was showing siphon at the level of tip of styloid process on both sides. The kinking was graded as grade 3 with angulation less than 300 . The left was relatively more tortuous than the right. The length of left external carotid was 8cm and right was 7cm. The measurements were taken from the point of bifurcation of common carotid artery upto the point where the external carotid artery gave the terminal branches namely maxillary artery and superficial temporal arteries. The length of internal carotid arteries were 7.3cm on right side and 7cm on left side. They were measured from point of bifurcation of common carotid artery up to the entry of internal carotid into carotid canal on the base of skull. Branches from the external carotid also showed variations. The superior thyroid artery arose from the common carotid much below the level of bifurcation on left side and at the level of bifurcation on right side. Supernumerary branches were arising from both the sides, namely, Arteries to Sternocleidomastoid muscle, tonsillar branches, Total 9 branches from right side of which 2 were branches to sternocleidomastoid muscle and 11 branches from left side of which 2 were branches to sternocleidomastoid muscle and one branch to tonsil. The branches to Sternocleidomastoid were crossing the internal carotid artery superficially and supplying the muscle. The tonsillar branch on left side passed along with internal carotid artery and then turned medially to enter the oropharynx to supply the palatine tonsil.
Dissected specimen of neck region on left side showing higher division of left common carotid at the level of hyoid bone with tortuous course of external carotid artery and internal carotid arteries. CCA-Common carotid artery, ECA-External carotid artery, ICA-Internal carotid artery, H- Hyoid bone, T- Upper border of thyroid cartilage, C7 ST-Sternocleidomastoid muscle, SP- Styloid process, 1-superior thyroid, 2-lingual, 3-facial, 4-ascending pharyngeal branch, 5-posterior auricular, 6-branch to tonsil, 7,8-sternocleidomastoid branches, 9-occipital, 10,11-maxillary and superficial temporal arteries.
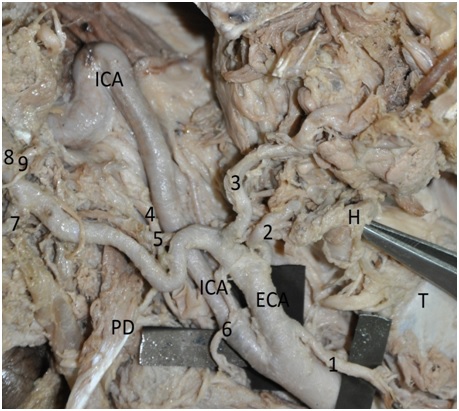
Dissected specimen of neck region on Right side showing Higher division of Right common carotid at the level in between hyoid bone and upper border of lamina of thyroid cartilage with tortuous course of external carotid artery and internal carotid arteries
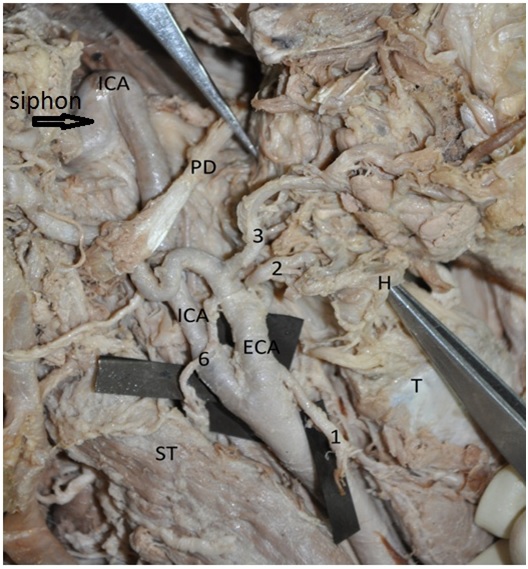
Dissected specimen of neck region on Right side showing Higher division of Right common carotid at the level in between hyoid bone and upper border of lamina of thyroid cartilage with tortuous course of external carotid artery and internal carotid arteries. CCA-Common carotid artery, ECA-External carotid artery, ICA-Internal carotid artery, H- Hyoid bone, T- Upper border of thyroid cartilage, ST-Sternocleidomastoid muscle, PD-Posterior belly of digastric, 1-superior thyroid artery, 2-lingual, 3-facial, 4-ascending pharyngeal, 5-posterior auricular, 6-sternocleidomastoid branch, 7-occipital, 8-superficial temporal, 9-maxillary artery. tonsillar branch was unilateral finding not seen on right side
Discussion
Anatomical variations occur throughout the course of carotid arteries. Variations may occur in origin, branching pattern and level of bifurcation.
The percentages of various levels of division of common carotid artery [1] are enumerated in [Table/Fig-4].
Percentages of various levels of division of common carotid artery
| Levels of bifurcation of common carotid artery | Percentage | Levels of bifurcation of common carotid artery | Percentage |
|---|
| C2 | <1% | C4 | 35% |
| C2-C3 | 4% | C4-C5 | 12% |
| C3 | 12% | C5 | 5% |
| C3-C4 | 30% | C5-C6 | 1% |
Ambali et al., studied 200 formalin fixed cadaveric specimens of carotid arteries. He observed the point of bifurcation of common carotid arteries, extra branches from common carotid arteries. The results were as follows. Normal level of bifurcation i.e. at the upper border of thyroid cartilage was observed in 44 specimens out of 100 on right side and 70 specimens out of 100 on left side, total 114 out of 200 i.e. 57%. Higher bifurcation i.e. above the upper border of thyroid cartilage was observed in 54 specimens out of 100 on right side and 30 specimens out of 100 on left side, total 84 out of 200 specimens i.e. 42%. Lower bifurcation i.e. below the upper borber of thyroid cartilage was observed in 2 specimens out of 100 on right side and none on left side i.e. 1%. [2].
Avadhani et al., reported a rare case of bilateral higher bifurcation of common carotid arteries, above the hyoid bone, superior to the posterior belly of digastrics muscle deep to mandible. Presence of bilateral unusual tortuosity (“S” shaped) of common carotid artery, tortuous external carotid artery, anomalous origin of the superior thyroid arteries [3]. Desai et al., reported a unique case of anomalous origin of bilateral linguofacial trunk from external carotid arteries with relative higher division of right common carotid arteries at C3 vertebral level [4].
Chaitra et al., reported a case with higher division of bilateral common carotid arteries and trifurcation of right common carotid into external carotid artery, internal carotid artery and occipital artery [5]. Ribeiro et al., studied 46 heads from male embalmed human cadavers [6]. He found that on right side 40% of the specimens showed bifurcation of Common carotid artery at C3 Level and 60% at C2 level. On left side 20% of the specimens showed the bifurcation of Common carotid artery at C3 level, 78% at C2 level and 2% at C4 level. Lo et al., commented that higher bifurcation of common carotid artery makes the hypoglossal nerve more vulnerable to injury during surgeries (iatrogenic injuries) [7].
Many studies have reported tortuous course of common and internal carotid arteries. We have found few studies in the literature with tortuous external carotid arteries. Internal carotid artery tortuosity is known to cause dizziness, vertigo, syncopes, blackout or persistent tinnitus [8].
Tortuosity may lead to arterial kinking which causes artery occlusion and is associated with severe symptoms including transient ischaemic attack, stroke, hemiplegia. According to classification done by Metz et al., in the present case the kinking was graded as grade 3 with angulation less than 300 [9].
Gupta et al., reported a case of 82-year-old female with 8 weeks of dysphagia. MRI of the neck revealed the tortuous course of common carotid arteries, which could have been the cause of dysphagia lusoria [10]. Deterling reported an additional 21 cases of tortuous carotid arteries [11]. In adults, carotid artery tortuosities are considered a risk factor for stroke but are not treated unless symptomatic. Course, variations and angulation of the carotid arteries produce changes in the laminar flow that lead to swirls which usually evolve all the way to strictures and stenosis [12].
Normally superior thyroid artery arises from external carotid artery. It may directly arise from common carotid artery. The various studies done and percentage of superior thyroid artery arising from common carotid artery are shown in [Table/Fig-5].
Percentage of superior thyroid artery arising from common carotid artery
| No | Authors | Percentage |
|---|
| 1 | Bergman et a., [13] | 18% |
| 2 | Ambali et al., [2] | 39% |
| 3 | Rimi et al., [14] | 8.8% |
| 4 | Hayashi et al., [15] | 30% |
| 5 | Lo et al., [7] | 52.3% |
In our case the superior thyroid artery was arising from the common carotid artery much below the level of bifurcation on left side and at the level of bifurcation on right side.
Embryological significance: Normally the internal carotid artery develops from the third aortic arch and the dorsal aorta further up. In foetal life and in infants the tortuousity of carotid arteries is common. With the descent of heart and elongation of the neck, the arteries assume the normal position. If the embryological state persists it leads to tortuosity or kinking of the arteries. (Agarwal and Agarwal, Shanley) [16,17]. Probably similar developmental anomaly has resulted in tortuous external carotid artery and internal carotid artery siphoning in the present case.
Supernumerary branches were arising from both the sides, namely, Artery to Sternocleidomastoid muscle, tonsillar branch, Total 9 branches from right side and 11 branches from left side. Normally they arise from occipital artery and facial artery respectively. Occasionally they may directly arise from external carotid artery [1]. Keirner et al.,) the incidence of strnocleidomastoid branches from external carotid artery was 23% [18].
Conclusion
Variations in the branching patterns may increase the risk of accidental vascular accidents during surgical procedures in the neck. Hence it is necessary to understand the anatomy of these vessels and its variations for interpretation of diagnostic and interventional vascular procedures and to carry out surgeries with minimum operative and postoperative complications. Tortuous arteries are dangerous as they may increase the chance of dysphagia, or evolving strictures and stenosis. Supernumerary branches from external carotid artery have got surgical importance. Hence such a case needs documentation.
[1]. Standring S, Collins P, Healy JC, Wigley C, ch: Neck. In: Gray’s AnatomyThe Anatomical basis of clinical practice 2008 40th edEdinburgElsevier Churchill Livingstone:444-45. [Google Scholar]
[2]. Ambali M, Jadhav S, Variations in bifurcation point and branching pattern of common carotid arteries: A cadaveric studyJ Pharm Biomed Sci 2012 25(25):147-51. [Google Scholar]
[3]. Avadhani R, Chakravarthi KK, Multiple bilateral anomalies of carotid arteries- a case reportNUJHS 2012 2(3):21-23. [Google Scholar]
[4]. Desai SD, Nuchhi A, Karjagi SB, Bilateral linguofacial trunk, A case reportNational J of Clinical Anatomy 2012 1(4):193-95. [Google Scholar]
[5]. Chitra R, Trifurcation of the right Common Carotid arteryIndian J Plast Surg 2008 41(1):85-88. [Google Scholar]
[6]. Ribeiro RA, Ribeiro JA, Filho OAR, Caetano AG, Fazan VPS, Common Carotid Artery Bifurcation Levels Related to Clinical Relevant Anatomical LandmarksInt J Morphol 2006 24(3):413-16. [Google Scholar]
[7]. Lo A, Oehley M, Bartlett A, Adams D, Anatomical variations of the common carotid artery bifurcationANZ J Surg 2006 76(11):970-72. [Google Scholar]
[8]. Aleksic M, Schütz G, Gerth S, Mulch J, Surgical approach to kinking and coiling of the internal carotid arteryJ Cardiovasc Surg 2004 45(1):43-48. [Google Scholar]
[9]. Metz H, Murray-Leslie RM, Bannister RG, Bull JW, Marshall J, Kinking of the internal carotid arteryLancet 1961 1:424-26. [Google Scholar]
[10]. Gupta A, Winslet MC, Tortuous common carotid artery as a cause of dysphagiaJ R Soc Med 2005 98:275-76. [Google Scholar]
[11]. Deterling RA, Tortuous right common carotid artery simulating aneurysmAngiology 1952 3:483-92. [Google Scholar]
[12]. Leipzig TJ, Dohrmann GJ, The tortuous or kinked carotid artery:pathogenesis and ‘clinical considerations. A historical reviewSurg Neurol 1986 25:478-86. [Google Scholar]
[13]. Bergman RA, Afifi AK, Miyauchi R, Illustrated encyclopaedia of human anatomic variations: Opus II: Cardiovascular system: alphabetical listinghttp://www.anatomy atlases.org/Anatomic variants/cardiovascular/Directory/Alphabetical/S.shtml [Google Scholar]
[14]. Rimi KR, Ara S, Hossain M, Postmortem study of thyroid arteries in Bangladesh peopleBangladesh J Anat 2009 7:26-33. [Google Scholar]
[15]. Hayashi N, Hori E, Ohtani O, Surgical Anatomy of the cervical carotid artery for carotid endarterectomyNeurol Med Chir 2005 45(1):25-29. [Google Scholar]
[16]. Agrawal R, Agrawal S, Dangerous anatomic variation of internal carotidartery – a rare case reportInt J Anat Variat 2011 4:174-76. [Google Scholar]
[17]. Shanley DJ, Bilateral aberrant cervical internal carotid arteriesNeuroradiology 1992 35:55-56. [Google Scholar]
[18]. Kierner AC, Aigner M, Zelenka I, Riedl G, Burian M, The blood supply of the sternocleidomastoid muscle and its clinical implicationsArch Surg 1999 134(2):144-47. [Google Scholar]