Double Tension Band Osteosynthesis in Inter-Condylar Humeral Fractures
Santosh Lakshmanrao Munde1, Mohmmed Javed Bhatti2, R.C. Siwach3, Anil Gulia4, Z.S. Kundu5, Sanjeev Bansal6, Sanjay Middha7, Hemlata T Kamra8
1 Associate Professor and HOD, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
2 Senior Resident, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
3 Professor and Director, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
4 Assistant Professor, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
5 Senior Professor, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
6 Assistant Professor, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
7 Assistant Professor, Department of Orthopeadics, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
8 Associate Professor, Department of Pathology, BPS GMC for Women, Khanpur Kalan, Sonepat, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hemlata T Kamra, B-15, BPSGMC Medical Campus, Khanpur Kalan, Sonepat, Haryana-131305, India.
E-mail: hemlatamunde@rediffmail.com
Introduction
Intercondylar humerus fractures are uncommon in orthopaedic practice. The treatment for the same has been described in the literature and include paragonal and orthogonal fixation by using plates. Tension band wiring as a treatment for the same is sparsely described in the literature.
Aim
To evaluate the effectiveness of "Double Tension Band wiring" method for the treatment of intercondylar fractures of humerus and compare the results with studies involving treatment with locked plates.
Materials and Methods
Twenty patients, all presenting with fresh fractures of the distal humerus, treated with double tension band wiring were retrospectively evaluated over a period of three years. Fractures were classified according to Jupiter classification of distal humeral fractures. There were 5 high T fractures, 13 low T fractures and 2 Y fractures. According to AO classification, all were C1 fractures. Average age of the patients was 56.20 years (32-70 years). There were 13 males and 07 females.
Results
Out of 20 cases treated with this method, rigid fixation and union was achieved in all of them. The average tourniquet time was 69 minutes with minimum of 50 minutes and maximum of 120 minutes. Radiological union was achieved at an average of 10.8 weeks (8-14weeks). Average range of motion was 104.5 degrees with maximum range of motion 120 degrees (10-130) and minimum of 70 degrees (30-100). Excellent or good results were obtained in 80% of the patients in our study.
Conclusion
Double tension band is a reliable, less demanding and cost effective method of fixation of intercondylar fractures of humerus.
Cost effectiveness, Distal humerus, Tourniquet time
Introduction
Intra-articular distal humerus fractures pose a considerable challenge to even the most experienced surgeon owing to the complex anatomy of the elbow, small fracture fragments and the limited amount of subchondral bone [1,2]. The functional outcome of distal humerus fractures is related to the ability to restore the normal anatomy and to allow early movement. Various methods of limited internal fixation have been described using Kirchner wires, screw fixation and single plates but stability provided by these methods is not enough to start early mobilisation; which affects the results [3–6]. Recently, with the advent of the anatomical plates, most surgeons fix these fractures by more than one screw in the intercondylar region, but none of these screws has a purchase on opposite cortex, thereby making fixation non-rigid which can dramatically increase nonunion rates [7]. We have described a simple, useful and rigid method of fixing the fractures of intercondylar region and maintaining the anatomy as normal as possible by using double tension band technique and thereby minimising hardware and cost. The condyles are first reduced with lag screws which are later fixed to humeral shaft with double tension bands which are tied across a screw inserted in the midline of humeral shaft. In this technique we utilized the principle of tension band wiring to achieve rigid fixation of both the columns of the fracture. This principle applies to the conversion of tensile forces to compression forces on the convex side of an eccentrically loaded bone [3]. This technique is technically less demanding, cost effective and utilises minimal implant which is easy to place and thus minimises the tourniquet time, an added advantage over double plate osteosynthesis.
Aim
To evaluate the effectiveness of Double tension band wiring method for the treatment of intercondylar fractures of humerus and compare the results with studies involving treatment with locked plates.
Materials and Methods
The present study was a set respective study carried out from February 2012 to March 2015; 20 patients of supracondylar fracture of humerus with intercondylar extension were operated at BPSGMC using this technique. All adult patients having C1 type intercondylar with fracture of the humerus were selected. Standard antero-posterior and lateral radiographs were obtained in the Emergency Department and fractures were classified according to Jupiter classification [4] of distal humeral fractures [Table/Fig-1]. CT scan was not done because CT scan facility was unavailable at our institution and this study was primarily done on poor patients who could not afford locked plates or expensive radiological investigations. There were 5 high T fractures, 13 low T fractures and 2 Y fractures. According to AO classification, all were C1 fractures [5]. Average age of the patients was 56.20 years (32-70 years). There were 13 males and 07 females.
Jupiter classification of distal humerus fractures
| High-T | Transverse fracture proximal to or at upper olecranon fossa |
| Low-T | Transverse fracture just proximal to trochlea |
| Y | Oblique fracture line through both columns with distal vertical fracture line |
| H | Trochlea is a free fragment (risk of AVN) |
| Medial lambda | Proximal fracture line exists medially |
| Lateral lambda | Proximal fracture line exists laterally |
| Multiplane T | T type with additional fracture in coronal plane |
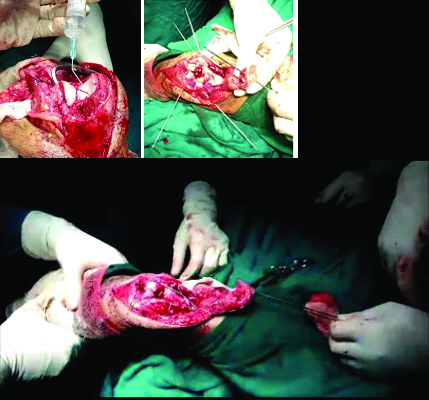
All patients were operated in lateral position under regional block or general anaesthesia. Non-sterile tourniquet was used and was inflated just before making the skin incision. We used posterior approach of elbow with olecranon chevron osteotomy. Ulnar nerve was identified and retracted to avoid injury. Intercondylar portion of fracture was first reduced and held with AO reduction clamp or k-wire as anatomical as possible. Then we passed a guide wire for cannulated cancellous screw from medial side to lateral aspect or vice versa in intercondylar area crossing fracture perpendicularly. A cannulated cancellous drill bit was used to drill over the guide wire and a proper sized 4mm cannulated cancellous screw was inserted over the guide wire to secure the fragments in place. Now the condylar block was attached to the humeral shaft using double tension band. Firstly, after reducing the condylar block to the humeral shaft, two k wires were passed from the lateral condyle across the fracture to engage the medial cortex of humeral shaft and likewise two k wires were passed from the medial condyle across the fracture to engage the lateral cortex of the humeral shaft. Now a 4.5 mm cortical screw with a washer was inserted in the midline of humeral shaft just above the fracture at the level of k wire tips. An 18 gauge stainless steel wire was passed beneath the screw head and across the medial k wire tips distally in figure of 8 manner and tightened using double loop. Similarly a tension band was applied laterally. Stability of the construct was checked under vision and olecranon osteotomy was closed using tension band wiring [Table/Fig-2]. Again the stability of the whole construct was checked by moving the elbow through full range of motion. Ulnar nerve was transposed anteriorly when needed. Tourniquet was deflated and haemostasis achieved. Wound was closed in layers over a suction drain. Drain was removed on second postoperative day and gentle active range of motion exercises was started. Patients were discharged from the hospital after suture removal around 11 or 12 days and followed up in OPD at 3 weeks, 4 weeks, 6 weeks and then monthly up to one year [Table/Fig-3,4,5,6 and 7]. Final result was graded according to criteria laid by Jupiter et al., [Table/Fig-8] [6]. General patient information has been provided in [Table/Fig-9].

Post operative radiograph at 10 weeks follow up

Postoperative radiograph at 4 week follow up

Postoperative radiograph at 6 week follow up

Patient at final follow up showing range of motion

Grading criteria by Jupiter et al., [4]
| Result | Loss of extension | Flexion | Pain | Disability |
|---|
| Excellent | <15° | >130° | None | None |
| Good | <30° | >120° | Slight | Minimal |
| Fair | <40° | >90° | With activity | Moderate |
| Poor | <40° | >90° | Variable | Severe |
General patient information
| Serial No. | Age | Sex | Jupiter class | Tourniquet time (in minutes) | Radiological union(In Weeks) | Extension (in degrees) | Flexion (in degrees) | Result |
|---|
| 1 | 32 | Male | Y | 60 | 8 | -10 | 130 | Excellent |
| 2 | 63 | Female | High T | 50 | 12 | -20 | 120 | Good |
| 3 | 65 | Female | Low T | 120 | 14 | -25 | 120 | Good |
| 4 | 58 | Female | Low T | 80 | 10 | -15 | 120 | Good |
| 5 | 65 | Male | High T | 50 | 12 | -20 | 120 | Good |
| 6 | 70 | Female | Low T | 60 | 10 | -30 | 100 | Fair |
| 7 | 55 | Male | Low T | 110 | 12 | -10 | 125 | Good |
| 8 | 61 | Female | Low T | 90 | 14 | -20 | 110 | Fair |
| 9 | 50 | Male | High T | 60 | 10 | -15 | 130 | Excellent |
| 10 | 45 | Male | Low T | 70 | 9 | -10 | 120 | Good |
| 11 | 55 | Female | Low T | 60 | 10 | -15 | 100 | Fair |
| 12 | 56 | Female | High T | 80 | 12 | -10 | 120 | Good |
| 13 | 68 | Male | Low T | 60 | 8 | 10 | 130 | Excellent |
| 14 | 60 | Male | Low T | 60 | 12 | 15 | 110 | Fair |
| 15 | 56 | Male | Low T | 50 | 10 | 10 | 130 | Excellent |
| 16 | 52 | Male | Low T | 70 | 14 | 10 | 120 | Good |
| 17 | 58 | Male | High T | 50 | 10 | 10 | 120 | Good |
| 18 | 55 | Male | Y | 60 | 9 | 10 | 120 | Good |
| 19 | 50 | Male | Low T | 80 | 10 | 15 | 120 | Good |
| 20 | 50 | Male | Low T | 60 | 10 | 15 | 110 | Fair |
Results
Out of 20 cases treated with this method, rigid fixation was achieved in all. The average tourniquet time was 69 minutes with minimum of 50 minutes and maximum of 120 minutes. Radiological union was achieved at an average of 10.8 weeks [Table/Fig-10]. Average range of motion was 104.5 degrees [Table/Fig-11] with maximum range of motion 120 degrees (10-130) and minimum of 70 degrees (30-100). The loss of range of motion was consistent with the age of the patient and compliance of the patient with physical therapy. One patient had ulnar nerve neuropraxia in the postoperative period which corrected over a period of 3 weeks via conservative approach. One patient had palpable k-wire tips beneath the skin which were removed after radiological union. Overall patients had minimal symptoms related to hardware. Overall 80% patients had excellent or good results [Table/Fig-12].
Histogram showing radiological union in weeks

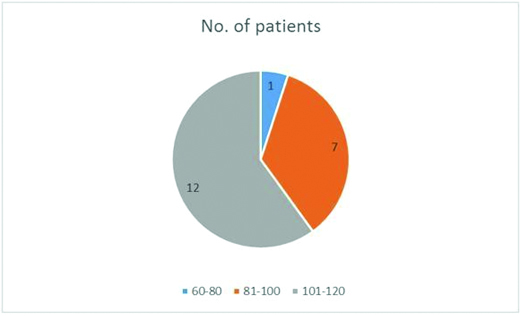
Pie diagram showing range of motion
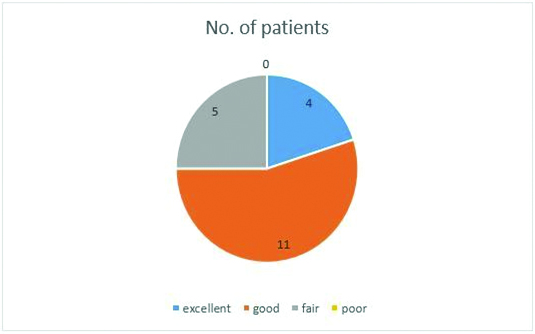
Pie-diagram showing results
Discussion
Distal humerus fractures remain a challenging reconstructive problem for orthopaedic surgeons due to complex anatomy of the distal humerus and difficulty in exposing the fracture. Anatomical reduction, rigid fixation and early mobilisation are required to prevent complications [7]. We have described one such method here which allows good compression at fracture site, rigid fixation utilising minimal hardware. This method has the advantage of early mobilization which can be attributed to the rigid fixation provided by the tension band. The amount of periosteal stripping & soft tissue damage is significantly less than plate fixation. It is a simple procedure and the duration of the surgeries in our series was around 80 minutes. It is cost effective when compared to the costs of plates. Tourniquet time can be minimised with this technique preventing tourniquet related complications. Because of the rigidity and stability achieved in this technique and because the tension band wiring technique acts in dynamic mode when muscles contract, we can mobilise the patient very early. In fractures in osteoporotic bone where large implants can have shattering effect and screw may loosen out, this technique gives good hold without fear of loosening with minimal implants.
Double tension band wiring has been used in past with encouraging results. In a study of 10 patients, Houben et al., reported comparable results, where 5 patients were treated with double tension band and 5 were treated with double plates [8]. Zhao et al., reported 83% excellent or good results in their study of 24 patients treated with double tension band wiring [9]. This method can also be used in combination with other methods of fixation, as reported by Allende et al., [10], where they concluded that the method is good alternative in osteoporotic settings when combined with other methods.
Presently, there is increasing trend towards the use of locked plates in intercondylar fractures of distal humerus. The very design of the locked plates is for osteoporotic fractures [11–13].
There are some disadvantages of these plates like the extensive soft tissue damage, technical expertise required, increased operative time and issues with contouring in some patients. The advantage of these plates, when compared with double tension band osteosynthesis lies in their biomechanical strength, as reported by Dogramacai et al., [14].
We have not studied the biomechanical strength of the tension band but since we were able to start early mobilization, all fractures united & there was no breakage of any wires; it can be postulated that this method has enough biomechanical stability to be used in clinical practice. Dubey et al., described a modification and did transosseous fixation of intercondylar fracture of lower end humerus by tension band wiring technique, and reported excellent results [15].
Our study shows that in inter-condylar fractures in adults, double tension band fixation can be a reliable, easy and cost effective technique for the management of these fractures and should remain an option to be considered when planning the stabilisation of these fractures especially the AO type C1 fractures. Our results are comparable to other studies done using locked plates.
Conclusion
Double tension band is a reliable, more biological, less surgically demanding and cost effective method of fixation of intercondylar fractures of humerus. Rigid fixation and hence, early mobilisation can be achieved with this method. This method avoids extensive soft tissue stripping and bulky hardware. Though locked plates are considered as gold standard in the treatment of fractures of the distal humerus, double tension band technique should be considered as an option while planning fixing these fractures especially AO type C1 fractures. The main limitations of this series are its retrospective nature, not having a control group, having a small number of patients and no experience with communited AO type C2 and C3 fractures.
[1]. Cannada L, Loeffler B, Zadnik MB, Eglseder AW, Treatment of high-energy supracondylar/intercondylar fractures of the distal humerusJ Surg Orthop Adv 2011 20:230-35. [Google Scholar]
[2]. Schmidt-Horlohé K, Wilde P, Bonk A, Becker L, Hoffmann R, One-third tubular-hook-plate osteosynthesis for olecranon osteotomies in distal humerus type-C fractures: a preliminary report of results and complicationsInjury 2012 43:295-300. [Google Scholar]
[3]. Pauwels F, Biomechanics of the Locomotor Apparatus 1980 Berlin Heidelberg New YorkSpringer-Verlag [Google Scholar]
[4]. Jupiter JB, Mehne DK, Fractures of the distal humerusOrthopedics 1992 15:825-33. [Google Scholar]
[5]. Ruedi T, Murphy WM, AO Principles of Fracture Management 2000 Vol. 1ThiemeStuttgart-New York [Google Scholar]
[6]. Jupiter JB, Noff U, Hoizach P, Allgower M, Intercondylar fractures of the humerus: an operative approachJ Bone Joint Surg (Am) 1985 67:226-39. [Google Scholar]
[7]. Gupta R, Khanchandani P, Intercondylar fractures of the distal humerus in adults: a critical analysis of 55 casesInjury 2002 33(6):511-15. [Google Scholar]
[8]. Houben PFJ, Bongers KJ, Wildenberg FAJM, Double band osteosynthesis in supra- and transcondylar humeral fracturesInjury 1994 25:305-09. [Google Scholar]
[9]. Zhao J, Wang X, Zhang Q, Surgical treatment of comminuted intra-articular fractures of the distal humerus with double tension band osteosynthesisOrthopaedics 2000 23:449-52. [Google Scholar]
[10]. Allende CA, Allende BT, Allende BL, Bitar I, Gonzalez GIntercondylar distal humerus fractures—surgical treatment and resultsChir Main 2004 23:85-95. [Google Scholar]
[11]. Gupta RK, Gupta V, Marak DR, Locking plates in distal humerus fractures: study of 43 patientsChinese Journal of Traumatology 2013 16(4):207-11. [Google Scholar]
[12]. Reising K, Hauschild O, Strohm PC, Suedkamp NP, Stabilization of articular fractures of the distal humerus: early experience with a novel perpendicular plate systemInjury 2009 40:611-17. [Google Scholar]
[13]. Greiner S, Haas NP, Bail HJ, Outcome after open reduction and angular stable internal fixation for supra-intercondylar fractures of the distal humerus: preliminary results with the LCP distal humerus systemArch Orthop Trauma Surg 2008 128:723-29. [Google Scholar]
[14]. Dogramaci Y, Esen E, Kürklü M, Kirici Y, Atahan AO, Kömürcü M, Double plate osteosynthesis provides better biomechanical stabilization than double tension band technique in distal humerus fracturesEklem Hastalik Cerrahisi 2010 21(1):44-49. [Google Scholar]
[15]. Dubey R, Sadigale V, Parmar J, Transosseous fixation of intercondylar fracture of lower end humerus by tension band wiring techniqueInternational Journal of Medical Science and Public Health 2014 3(3):305-07. [Google Scholar]