The role of coronal leakage in the prognosis of root canal treatment has been known since years and is also an extensively studied topic among various researchers. Marshall and Massler in 1961 was the first to draw attention towards the effect of coronal leakage [1,2]. However, in the present era, coronal as well as apical leakage still remains as an important cause of endodontic failure in spite of presence of advanced endodontic materials, the attributing cause may be different endodontic filling techniques, physical and chemical properties of sealers and presence or absence of smear layer [3]. Many a time these failures lead to other pulpal and periradicular diseases which results due to contamination of these tissues caused by microorganisms and/or their by-products. The root canal system, once contaminated, may conceal many species of microorganisms along their antigenic by-products and as a consequence, variable amounts of inflamed or necrotic tissues. Thus, preventive and restorative dentistry aims to prevent access of microorganisms into the coronal pulpal space and root canal system [4]. The root canal filling material should provide a barrier that prevents bacteria from the oral cavity to travel down the root canal [5].
Gutta percha is the most widespread used root canal obturation material. It is compressible and inert in nature, dimensionally stable, radiopaque, tolerated by tissues and is converted into plastic when heated. Different techniques for the purpose of root canal filling have been devised of which cold lateral condensation being the most commonly used method followed by the warm vertical, use of thermoplasticized gutta percha [6]. Various methods such as bacterial leakage, electrochemical, fluid filtration and penetration of tracers has been implied in the past to evaluate the sealing ability of different restorative techniques and materials to prevent penetration of microorganisms [6,7]. Bacteria used as a tracer can be considered as better method because bacteria closely mimics what happens clinically in oral cavity in terms of leakage in endodontically treated teeth where as fluid filtration and dye extraction methods are simple and has high reproducilbility [3].
The present study was undertaken to evaluate the leakage in endodontically treated teeth using four different methods of obturation and analysing the leakage by using two in vitro tracer methodologies i.e. bacteria and dye penetration utilising clearing technique.
Materials and Methods
The present study was carried out in the Department of Conservative Dentistry and Endodontics, in co-ordination with Department of Oral Pathology at Mahatma Gandhi Dental College, Jaipur from December 2013 to May 2014 after the approval by the ethical committee of the institute. The present study comprised of 90 extracted permanent single rooted anterior human teeth selected randomly which were cleaned of calculus, bone or any soft tissue by placing in 5.25% sodium hypochlorite for two weeks followed by removal of the crown at the cement-enamel junction or below using a diamond disc and standardizing the root lengths to 16 mm. Root canals were evaluated for apical patency with a file of size 10 and were instrumented using the ProTaper hand files, in concurrence with 2.5% sodium hypochlorite (NaOCl) irrigation. Working length was determined by subtracting 0.5 mm from the length at which the file tip extruded apically. The ProTaper instruments [Table/Fig-1] were used according to the manufacturer’s instructions in a crown-down manner. After root canal preparation was completed to a size F3 ProTaper instrument, the teeth were placed in an ultrasonic bath with 17% ethylene diamine tetraacetic acid (EDTA) for 30 sec followed by 5.25% NaOCl to remove the smear layer and then in physiological saline to remove the left over EDTA and NaOCl. Teeth were then randomly distributed into five groups consisting of 20 each in four groups and fifth group having 10 teeth as controls.
| Armamentarium/Materials | Manufacturer | Type/Composition |
|---|
| K-files | Dentsply | Stainless steel filesSize- 10Taper- 0.02 |
| Protaper hand files | Dentsply | Nickel titanium filesSize- Sx, S1,S2,F1,F2,F3 |
| E&Q PLUS | Meta | |
| Incubator machine | | |
| Thermafil oven | Dentsply | |
| Stereo microscope | | |
| Sodium hypochlorite | Vishal India | 5.25% concentration |
| 17% EDTA | Sybron Endo | |
| Thermafil carrier obturators | Dentsply | |
| Gutta percha points | Sure-endo | F3 Size |
| Trypticase soy broth | | |
| Trypticase soy broth | | |
| Proteus vulgaris bacteria | | |
| Tubli seal | Sybron endo | Zinc oxide based sealer |
| Methylene blue | Loba chemicals ltd. | |
| Nitric acid | Shandong Fengyuan Chem Co. | 10% concentration |
| Ethyl alcohol | Changshu Yang yuan chemical | 70, 80%, 90%, 100% concentrations |
| Methylsalicylate | Sol fine-chem Ltd. | Winter green oil synthetic |
In group 1, teeth were obturated using F3 thermafil gutta percha carriers and tubliseal sealer. After placement of a thin layer of sealer at the coronal orifice, thermoplasticized gutta percha was delivered into canal. After gutta–percha cooled, excess was removed using DG-16. Group 2 comprised of teeth obturated using lateral condensation. The process included first checking the size F3 cone fitted with tugback. Sealer was introduced into the canal with a paper point. The master apical cone tip was dipped in sealer, and then seated apically. Two fine accessory cone and master cone were compacted 1mm short of working length. No vertical compaction was performed. Group 3 comprised of teeth obturated using vertical condensation or warm gutta percha technique. Master cone was selected on the basis of working length. Sealer was placed in canal with master cone. A heat carrier (plugger) was heated and was carried into the canal vertically which caused flow of guttapercha. After packing gutta – percha within 4- 5 mm of apex, gutta percha is back packed until it is at the orifice of the canal. Group 4 comprised of teeth obturated using lateral and vertical condensations. Primary cone was inserted slowly and gently into the canal to measured length. A spreader was inserted apically alongside the primary cone wedging it against the canal wall by applying lateral and apical pressure, additional guttapercha was inserted in the space created. Guttapercha mass was vigorously packed apically using preselected cold pluggers. Group 5 comprised of control group which consisted of five teeth with patent apices without a guttapercha filling as positive controls. Negative controls consisted of five teeth with guttapercha filling but with all orifices sealed with glass ionomer cement.
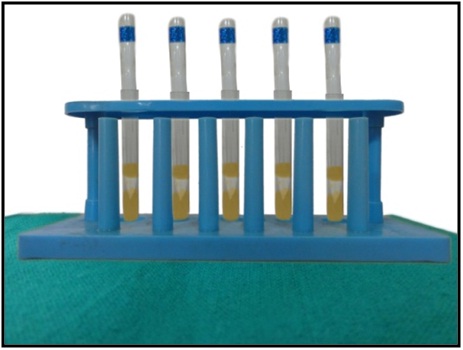
After obturation, teeth were kept in 100% humidity for 90 days and then were assembled in the testing apparatus [Table/Fig-2] consisting of two tubes of different sizes. The larger diameter external tube was chosen to coincide with the circumference of the coronal portion of the test tooth. The external tube was affixed to the tooth with glass ionomer cement. The second tube, which was designed to fit appropriately within the lumen of the first tube, was placed directly over the opening of the canal and was used to utter the bacteria and ink directly to the coronal canal orifice. After assembling this delivery system, two coats of nail varnish was applied on the remaining part of the root, 1mm short of the apex. Then sterile test tubes were filled with 0.5 ml of motility medium followed by filling with 0.25 ml of Proteus vulgaris in Trypticase soy broth. The tubes were agitated to ensure that bacteria reaches the orifice. The racks of teeth were oriented vertically and placed in an incubator at 370C for 21 days. The reservoirs of motility media in test apparatus were inspected daily to check for turbidity as an indicator for the presence of bacterial leakage. Then to retain continuity between the bacterial groups and methylene blue, the test apparatus was positioned in new sterile tubes with fresh agar at the apex. Methylene blue (0.25 ml) was kept in coronal reservoir and was shaken down to make sure that the dye reaches the orifice of the canal. All five groups were placed into the incubator and the testing apparatus was disassembled after 21 days, nail varnish was removed and the teeth were placed in glass container for clearing. The teeth were cleared by placing in 10% nitric acid for 3 days, followed by dehydration by sequential placing in 70,80,90 and 100% ethyl alcohol. After dehydration, the teeth were cleared by placing in methyl salicylate. After that, each tooth was photographed with stereomicroscope at 6x magnification. Photographs were examined and calibrated to the scoring given in [Table/Fig-3].
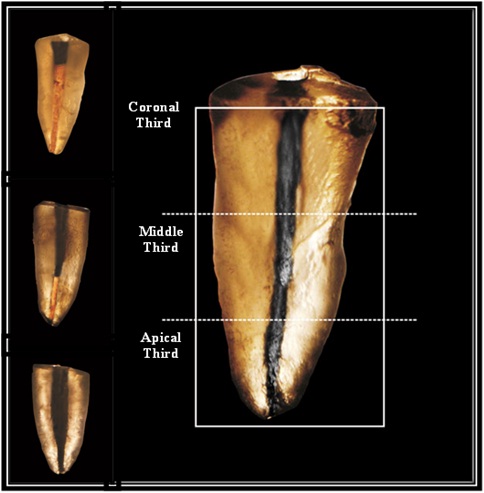
Scoring criteria for coronal leakage
| Scoring Criteria |
|---|
| Score 1 | Ink staining within coronal and one thirds of Obturated canal space |
| Score 2 | Ink staining within the coronal and middle of Obturated canal space |
| Score 3 | Ink staining within the coronal, middle and apical third of the Obturated canal space |
Statistical Analysis
The data so obtained were collected and entered into a Microsoft Excel Worksheet and analyzed using SPSS (version 7.5) statistical package. Chi-square test was used for statistical analysis and p value <0.05 was considered as significant value.
Results
Results of the leakage data recoded for a span of 21 days from the four groups, showed that all the groups showed bacterial leakage. As summarised in [Table/Fig-4], lateral condensation group showed the maximum leakage in about nine out of the 20 teeth, thermafil group showed leakage in six of the 20 teeth, vertical condensation group five out of 20 and the least leakage was observed in case of teeth obturated using lateral and vertical condensations that showed leakage in three out of the 20 teeth evaluated. The bacterial leakage values, showed statistically significant difference.
Data summarising bacterial leakage in relation to obturation method
| Groups | Obturation Method | Total specimen | Bacterial Leakage | Scores | p-value |
|---|
| | | | No leakage | 1 | 2 | 3 | |
|---|
| Positive control | 5 | 5 | | | 3 | 2 | |
| Negative control | 5 | 0 | 5 | | | | |
| Group 1 | Thermafil Carrier | 20 | 6 | 14 | 4 | 2 | | 0.038(significant) |
| Group 2 | Lateral Condensation | 20 | 9 | 11 | 2 | 5 | 2 | 0.223 (not significant) |
| Group 3 | Vertical Condensation | 20 | 5 | 15 | 3 | 2 | | 0.121 (significant) |
| Group 4 | Vertical And Lateral Technique | 20 | 3 | 17 | 1 | 2 | | 0.046 (significant) |
There were no statistically significant results for the dye penetration among the four obturation techniques when methylene blue was used to measure the leakage. It was observed that the lateral condensation group showed the maximum penetration with eight out of 20 teeth showing penetration upto the apical level, 10 teeth to the middle levels, followed by the vertical condensation group showing four teeth with dye penetration to the middle third of the root, 16 teeth restricted to the coronal level, followed by the vertical and lateral condensation group only one tooth showing leakage, one tooth showing penetration upto the apical level, two with dye penetration to the middle third of the root, 16 teeth restricted to the coronal level, and least leakage seen in the thermafil carrier group with six teeth showing no leakage, 4 teeth reaching upto the middle third level [Table/Fig-5,6]. Comparison of both methods showed variation with insignificant p value [Table/Fig-7].
Data showing leakage levels of dye penetration
| Scoring Criteria | Vertical Condensation | Thermafil Carrier | Lateral Condensation | Vertical And Lateral Technique |
|---|
| Coronal | 16 | 10 | 2 | 16 |
| Middle | 4 | 4 | 10 | 2 |
| Apical | 0 | 0 | 8 | 1 |
| No Leakage | 0 | 6 | 0 | 1 |
| p-value | 0.469 | 0.206 | 0.432 | 0.301 |
Schematic representation of the various levels of dye penetration
Data showing comparison of bacterial leakage and dye penetration
| Level | Vertical Condensation | Thermafil Carrier | Lateral Condensation | Vertical And Lateral Technique |
|---|
| Scoring Criteria | Bacterial leakage | Dye leakage | Bacterial leakage | Dye leakage | Bacterial leakage | Dye leakage | Bacterial leakage | Dye leakage |
|---|
| Coronal | 3 | 16 | 4 | 10 | 2 | 2 | 1 | 16 |
| Middle | 2 | 4 | 2 | 4 | 5 | 10 | 2 | 2 |
| Apical | 0 | 0 | 0 | 0 | 2 | 8 | 0 | 1 |
| No Leakage | 15 | 0 | 14 | 6 | 11 | 0 | 17 | 1 |
| p-value | 1.722 (not significant) |
The positive control groups showed complete bacterial and Methylene blue dye penetration to the apex. Whereas, the negative control groups in the bacterial penetration exhibited no bacterial contamination. In the dye leakage groups, no leakage was seen in the canal space.
Discussion
The root canal is a complex system with many surface irregularities, fins, accessory and lateral canals, and isthmuses [6]. Complete obturation of the root canal system and the development of an impervious seal are regarded as important elements of successful endodontic treatment [8]. The coronal seal prevents saliva, bacteria and bacterial byproducts in the oral cavity from invading and harbouring the root canal system and gaining access to the periradicular tissues. Loss of coronal seal may result from leakage of temporary filling, fracturing of restorative material or tooth structure, recurrent caries or failure to have an appropriate provisional restoration replaced after root canal treatment [9].
The present study was undertaken to evaluate the leakage in endodontically treated single-rooted teeth using four different methods of obturation i.e. lateral compaction, vertical compaction, combination of lateral and vertical compaction and thermafil and analysing the leakage by using two in vitro tracer methodologies i.e. bacteria and dye penetration utilising clearing technique.Proteus Vulgaris bacteria and methylene blue dye were used as tracers. Maxillary single rooted anterior teeth were selected for the purpose of the study for their incidence of straight and single canals to the apex in about 99.7% of the cases [10]. All teeth were decoronated at or below the level of the cemento- enamel junction to facilitate straight line access for instrumentation and obturation. The teeth were stored in deionized water following decoronation, to exclude the possibility of cracks in dentine, prior to assembly in the test apparatus and sterilization [11].
Gilbert SD et al., [12] carried a similar study using India Ink as a tracer and demonstrated that vertical compaction leaked significantly less than lateral compaction during bacterial challenge. However, in a review carried by Verissimo DM et al., [3] it has been demonstrated that size and weight of Indian ink molecules are smaller than those of the bacterial molecules that harbour the root canal. Thus this dye used as a tracer may not mimic the molecules of fluid coming from periradicular tissue and thus may present false positive results during leakage evalution. On the other side, methylene blue is inexpensive, easy to manipulate and shows a high degree of staining.
Proteus vulgaris was selected in the present study for its comparable size to endodontic pathogens, ease of growth and viability. This organism’s comparable size to pathogens provides a biologically relevant model. Additionally, the ease it affords in identifying contamination and species identification is useful in experimental management [12].
Tubliseal used in the present study is a two paste system with the composition of zinc oxide, oleo resins, bismuth trioxide, oils, thymol iodide and modifiers. It mixes easily, has ample working time and good flow properties, does not show any technical difficulties during obturation procedures and also confers a superior lubrication in comparison to other sealers [13]. Khyat et al., [14] carried out a study and found that all root canals were recontaminated by bacteria from natural human saliva in less than 30 days after obturation using lateral and vertical condensation techniques. The teeth were stored in 100% humidity for the period of 90 days prior to bacterial penetration in the present study. This was carried out to eliminate the possible bactericidal effects of free eugenol in the sealer and to ensure that the obturated mass becomes dimensionally stable [11].
Lateral condensation remains the most widely accepted and used obturation technique. The irregularity of many root canal systems and canal curvature can complicate its application [15]. In this method, the root filling does not consist of an homogeneous mass of material but rather of a large number of individual points joined by cementing substances [16]. But it has advantages of low cost and to control the length of the fill. However, if there is poor preparation of the canal, mismatch of spreaders, GP cone and canal, this may result in spaces between the GP cones [15].
In the present study, comparison of the bacterial leakage among the groups showed that the combination of vertical condensation with lateral compaction group showed the least leakage patterns among the teeth followed by the teeth obturated with thermafil carriers and maximum leakage seen in case of lateral condensation group. Similarly, Baumgardner et al., [17] also found that using lateral compaction followed by vertical forces decreased leakage with carbon dye.
Gueorgieva T et al., [18] carried out a comparative study to evaluate microleakage of obturated root canals after disinfection with Neodymium:yttrium-aluminum-garnet (Nd:YAG Laser), Photodynamic therapy(PDT) and NaOCl and EDTA, teeth were dried with sterile paper points and obturated with gutta-percha and AH26 sealer by warm condensation. The leakage was shown using dye penetration test with methylene blue for a period of three days at 37°C and it was observed that microleakage was observed in all studied groups. De Oliveira SG dias et al., [19] carried out a study to investigate the coronal microleakage of endodontically treated teeth exposed to contamination by fresh human saliva and reported an index of 90% of microleakage in root canals after 24 hours for root canals instrumented, obturated, and prepared to receive an intracanal post and 70% of microleakage in samples at the end of 40 days for root canals with cemented posts but without coronal sealing.
Studies have shown that plasticized guttapercha can be easily moved into the canal irregularities, thus replicating the intricacies of the root canal system. Warm condensations techniques produced a higher guttapercha to sealer ratio than the cold lateral condensation technique [20]. Thus, to improve the homogenicity as well as surface adaptation of GP, there was a need to introduce a technique that can seal the inconsistencies and coarseness of the canal space, thus thermoplasticized injectable obturation techniques were introduced [6]. Budd et al., [21] compared the quality of obturation using high and low temperature thermoplastic injectable GP techniques with lateral condensation and proved both the thermoplasticized injectable techniques were significantly better than lateral condensation. On the contrary, Lares et al., [22] found that root canals obturated with the thermafil technique leaked more than those obturated with lateral condensation. The present study also aimed to compare both the methods and found that bacterial leakage and dye leakage demonstrated considerable variability.
Limitation
Within the limitation of the study, it seems that experimental model cannot mimic the in vivo situation completely. On the other hand, it enables the observation of dye penetration but whether that is associated with porosities in the gutta percha or the presence of empty spaces, or changes in the structure of thermoplasticized gutta percha that remains a mistry. The bacterial method requires vitality and activity of bacteria, the process is complex and requires the need of a skilled microbiologist and inconsistency among these factors can result in variability among the results. Thus, although both methods assessed the same substrate, but results showed variation which emphasise that there is a need of further studies to standardize a method for the assessment of coronal and apical leakage of endodontic obturating methods.
Conclusion
Within the parameters of this study, it was concluded that combination of lateral and vertical condensation group showed least bacterial leakage, thermafil carrier group showed more leakage than vertically condensed group and lateral condensation group showed the maximum leakage. In case of dye penetration leakage evaluation thermafil carrier group showed the least leakage and lateral condensation group showed the maximum leakage. Thus, due to the presence of variability among the results obtained by two different analytic methods used in the present study, the study emphasizes the need of standardization of methods, as the lack of standardization hinders the comparison of different endodontic filling techniques.