Repositioning of Misplaced Central Venous Catheter with Saline Injection Under C-Arm Imaging
Parshotam Lal Gautam1, Sandeep Kundra2, Krishan Jain3, Hitika Monga4
1 Professor and Head, Department of Critical Care Medicine, DMC & H, Ludhiana, Punjab, India.
2 Associate Professor, Department of Anaesthesia, DMC & H, Ludhiana, Punjab, India.
3 Post Graduate Resident, Department of Anaesthesia, DMC & H, Ludhiana, Punjab, India.
4 Post Graduate Resident, Department of Anaesthesia, DMC & H, Ludhiana, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sandeep Kundra, 305 – E, Shaheed Bhagat Singh Nagar, Pakhowal Road, Ludhiana-141013, Punjab, India
E-mail: Sandeepkundra07@gmail.com
Malposition of central venous catheter is a well known technical complication. Misplaced catheter often requires reinsertion for proper placement of the catheter in the superior vena cava (SVC) to support safe delivery of care and minimize complications. But reinsertion exposes the patient once again to risks of complications related to the procedure including potential of misplacement. Literature describes only a few techniques for repositioning a misplaced central venous catheter (CVC). We tried old simple method of saline injection with force under image intensifier using hydrostatic force of intravenous fluid to straighten the CVC. We could successfully reposition two misplaced CVC’s using this method.
Central venous catheter, Malposition, Misplacement
Case Reports
Case-1
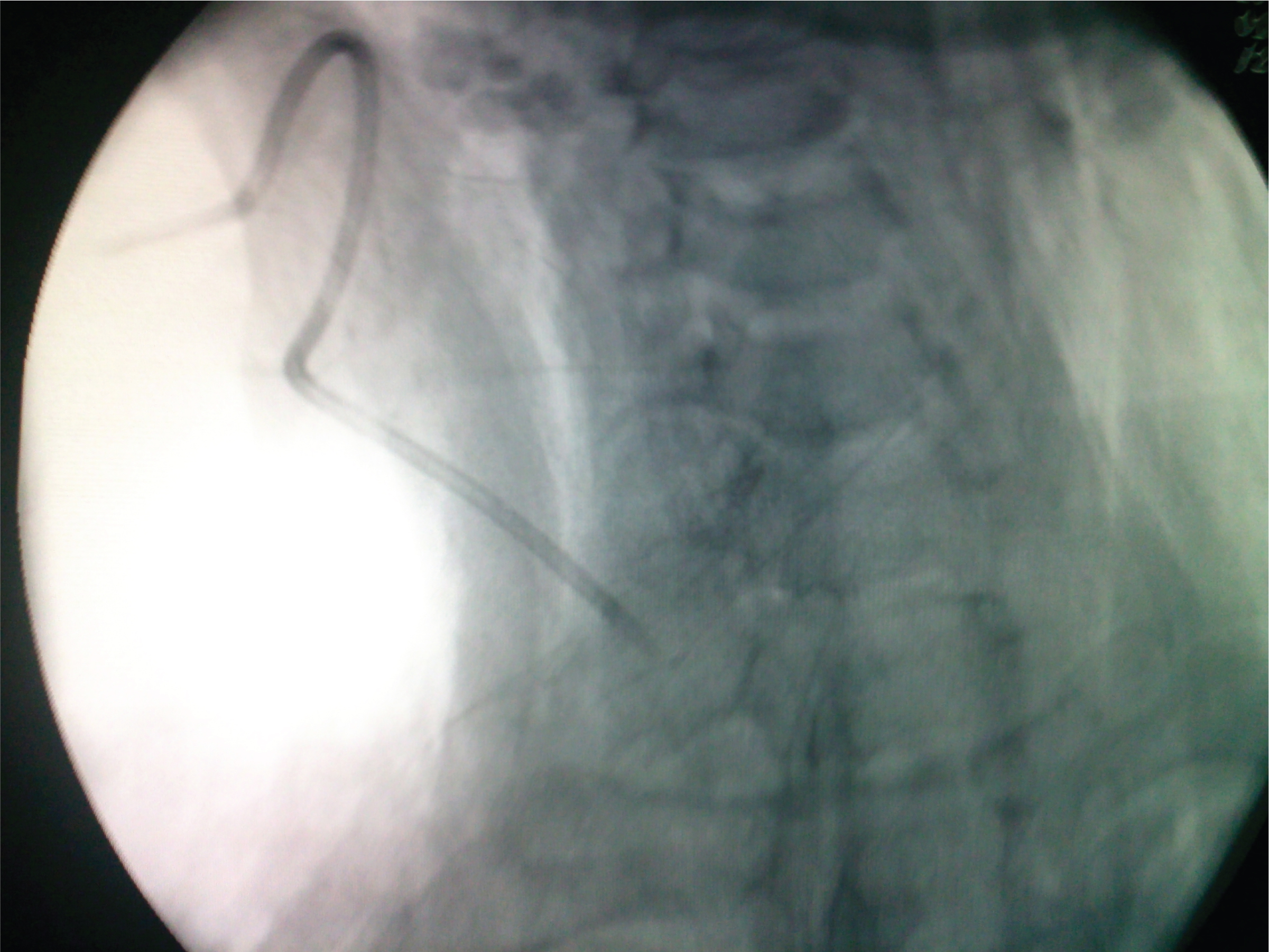
A 55-year-old male patient was admitted with acute pyelonephritis & had difficult venous access. So decision was taken to insert central line for intravenous (IV) access & central venous pressure (CVP) monitoring. Initial trial of central line insertion in ward had failed so plan was made to insert central line under ultrasound guidance. After standard aseptic precautions, under ultrasound guidance, right internal jugular vein (IJV) was pierced with 16 G cannula, guide wire inserted and right IJV cannulated with a double lumen catheter using Seldinger’s technique. Increased resistance was felt while removing the guide wire; however, blood could be aspirated from both ports of the catheter. Post procedure chest X-ray revealed that central line was lying in Right IJV but coiled on itself like a hair pin [Table/Fig-1]. We decided to reposition the central line using hydrostatic method under flouroscopic guidance. Patient was taken to operation table; neck was painted with povidone iodine & sterile draping done. Sutures holding the central venous catheter (CVC) were removed & catheter withdrawn by 5cm under C- arm guidance. Then a syringe containing 10ml of normal saline was connected to the 16 G lumen & a sudden push of saline was given & this was repeated four times. After each saline push, the central line tip was visualized under C-arm. We could see the U-turn of central venous catheter straightening with each saline push [Table/Fig-2]. When the catheter had fully straightened, it was inserted another 6cm and fixed at 12cm at skin level and the tip of central line could be visualized just above superior vena cava. Blood could be aspirated from both ports.
CVC coiled upon itself in the IJV,

Misplaced CVC getting corrected by the use of saline push,
Case-2
A 12-year-old male was planned for central line re-insertion because the previous CVC got dislodged accidently. Left sided subclavian vein (SCV) was cannulated using Seldinger’s technique, guide wire was removed and blood aspirated from both ports. However, post procedure chest X-ray revealed that the tip of catheter had gone into the left internal jugular vein [Table/Fig-3]. Plan was made to reposition the central line using hydrostatic method. After painting & sterile draping, sutures holding the central venous catheter was removed & catheter withdrawn by 4cm. A 10cc syringe filled with Normal saline was connected to 16 G port and sudden push of saline given, this was repeated 5 times and we could visualize the catheter to be straightening [Table/Fig-4]. Then the catheter was inserted without inserting guide wire and the tip visualized in superior vena cava under C-arm guidance.
Misplaced subclavian venous catheter entering ipsilateral IJV,

Misplaced CVC being corrected

Discussion
Central venous cannulation is a commonly performed procedure in critically ill patients requiring central venous pressure (CVP) monitored fluid therapy or infusion of vasoactive drugs. However central venous cannulation is associated with certain complications, common ones of which are haematoma, pneumothorax and infections [1]. Malposition of CVC is a well known technical complication which is often diagnosed on post procedure check X-ray chest. Ultrasound guided central line placement has revolutionized the technique of central line insertion. The advantage of ultrasound guided CVC insertion is that it provides visualization of vein, thus it improves success rate of veni-puncture and decreases the complications rate [2]. However, it does not guide the subsequent positioning of catheter tip, thus incidence of misplacement is not reduced to a significant extent [3].
Literature reports a 2% incidence of malposition in post-cannulation chest radiographs [4]. The common locations for misdirected catheters include the ipsilateral and contralateral internal jugular veins and contralateral subclavian vein. Malposition has been found to be significantly more common with subclavian approach as compared to jugular approach [3]. Its incidence during SCV puncture is reported to vary from 1.8% to 9.3% [4]. Commonly right SCV gets malpositioned to ipsilateral IJV [3,4]. Malpositioned catheter may provide erroneous CVP readings resulting in mismanagement and thus may be a poor predictor for fluid and vasoactive drug infusion therapy. Although it has remained subject of debate for long, increasing evidence has shown that correct tip placement is of paramount importance for safe & effective use of central line [5].
It is controversial and debatable whether to reposition a misplaced CVC or not. While some authors opine that clinical use of malpositioned catheters is associated with a few complications and it may be used [6], others argue that improper catheter tip position increases the risk of venous thrombosis, venous wall perforation due to abutting at angle and other related complications [3].
Hence, the malpositioned central line have to be sometimes repositioned, removed & reinserted at another site. Reinsertion, however, again exposes the patient to procedure related complications including potential of malpositioning of catheter.
Various techniques have been introduced in the past to reposition the catheter with merits and demerits [7–10]. Schaefer used a flow directed method using 2F Fogarty balloon-tipped catheter for this purpose [8]. Hawkins & Paige described the use of a deflector to correct a malpositioned central line [8]. Percutaneous transfemoral approach offers a minimally invasive option for repositioning of the malpositioned catheter wherein, CVC tip is directly manipulated by use of tip-deflecting wires [11]. The authors have no direct experience with the said techniques but it has been suggested that increased risk of infections is the drawback of direct manipulation by tip deflecting guide-wire [12]. Hartnell repostioned misplaced CVC 91 times in 83 patients via the transfemoral vein approach [9]. The transfemoral approach is an attractive and reliable method but its limitation is that it requires a skilled operator and specialized angiographic suite, which may not be universally available [6].
We describe a new method of an old technique that uses forceful saline injection under image intensifier for correction of malpositioned CVC [12]. In this technique, first catheter is withdrawn under aseptic conditions to a favorable position and then a force is given using jet of saline to straighten the bend in the central line. After straightening the catheter, we reinserted & repositioned the CVC under fluoroscopic guidance and visualized the tip in SVC. Misplacement into both IJV and subclavian vein can be corrected using this technique.
Since only saline flush is being used, the technique is safe and technically easy to perform. We have successfully used this technique in two of our patients and have not encountered any problem. Strict aseptic precautions need to be taken when employing this technique. There are concerns of introducing infection when the CVC is removed from the skin puncture site and then reinserted again. Chances of catheter colonization increase with the passage of time, there being a linear relationship between duration of CVC placement and colonization rate [13] Post central line Chest X-ray is routinely done at most places so malposition is usually noticed within first few hours. Another concern is that sometimes vigorous injection of saline may be unsuccessful because sufficient force may not be transmitted for repositioning large caliber central venous catheters or the position of catheter may not be favorable for repositioning. We repositioned both CVC’s within first four hours and chances of colonization and infection are least at that time. In our case, both patients showed no evidence of infection even after the lines were kept for 15 days.
Conclusion
Correct placement of the central venous catheter is an essential prerequisite for accurate monitoring of CVP and long-term use of catheter. Hydrostatic method, as described above is a safe and effective method, but is not commonly practiced due to lack of awareness about it. We recommend that it should be used more frequently.
[1]. Bowdle A, Vascular complications of central venous catheter placement: evidence-based methods for prevention and treatmentJ Cardiothorac Vasc Anesth 2014 28(2):358-68. [Google Scholar]
[2]. Costello JM, Clapper TC, Wypij D, Minimizing complications associated with percutaneous central venous catheter placement in children: recent advancesPediatr Crit Care Med 2013 14(3):273-83. [Google Scholar]
[3]. Gibson F, Bodenham A, Misplaced central venous catheters: applied anatomy and practical managementBr J Anaesth 2013 110(3):333-46. [Google Scholar]
[4]. Pickwer A, Baath L, Davidson B, Perstoft I, Akenson J, The incidence and risk of central venous catheter malpositioning: a prospective cohort study in 1619 patientsAnaesth Intensive care 2008 36(1):30-37. [Google Scholar]
[5]. Vessely TM, Central venous catheter tip position: A continuing controversyJ Vasc Intervent Radiol 2003 14(5):527-34. [Google Scholar]
[6]. Gerbaur B, Teichgraber UK, Podrabsky P, Werk M, Hanninin EL, Felix R, Radiological interventions for correction of central venous port catheter migrationsCardiovasc Intervent Radiol 2007 30:216-21. [Google Scholar]
[7]. Schaefer CJ, Geelhoed GW, Redirection of Misplaced Central Venous CathetersArch Surg 1980 115:789-91. [Google Scholar]
[8]. Hawkins IF, Paige RM, Redirection of Malpositioned Central Venous CathetersAJR 1983 140:393-95. [Google Scholar]
[9]. Hartnell GG, Gates J, Suojanen JN, Clouse ME, Transfemoral repositioning of malpositioned central venous cathetersCardiovasc Intervent Radiol 1996 19(5):329-31. [Google Scholar]
[10]. Thalhammer A, Jacobi V, Balzer J, Vogl TJ, Repositioning of malpositioned or flipped central venous cathetersEur Radiol 2002 12:698-700. [Google Scholar]
[11]. Iovino F, Pittiruti M, Buononato M, Central venous catheterization: complications of different placementsAnn Chir 2001 126:1001-06. [Google Scholar]
[12]. Olcott EW, Gordon RL, Ring EJ, The injection technique for repositioning central venous catheters: technical noteCardiovasc Intervent Radiol 1989 12(5):292-93. [Google Scholar]
[13]. Morreti E, Ofstead C, Kristy R, Wetzler H, Impact of central venous catheter type and methods on catheter-related colonization and bacteraemiaJournal of Hospital Infection 2005 61(2):139-45. [Google Scholar]