Multiple Compond Odontomas in the Jaws: A Rare Case Report
Pavan Kumar Gujjar1, Priya Sahni2, Treville Pereira3, Jyoti Zingade4
1 Senior Lecturer, Department of Oral and Maxillofacial Pathology, Narsinhbhai Patel Dental College and Hospital, Visnagar, Gujarat, India.
2 Professor and HOD, Department of Oral and Maxillofacial Pathology, Narsinhbhai Patel Dental College and Hospital, Visnagar, Gujarat, India.
3 Professor, Department of Oral and Maxillofacial Pathology, D.Y Patil School of Dentistry, Navi-Mumbai, India.
4 Post-Graduate Student, Department of Oral Medicine and Radiology, Narsinhbhai Patel Dental College and Hospital, Visnagar, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pavan Kumar Gujjar, Senior Lecturer, Department of Oral and Maxillofacial Pathology, C-S/2, S.K Campus, Narsinhbhai Patel Dental College and Hospital, Ambaji Road, Visnagar, Gujarat- 384315, India.
E-mail: jyopavan2612@gmail.com
Odontomas are tumours of odontogenic origin. In these tumours both the epithelial and mesenchymal cells undergo differentiation to form enamel and dentin with variable amounts of cementum and pulp tissue. The odontomas represent a hamartoma rather than a neoplasm. When the enamel and dentin are laid down in an organized manner it is termed as a compound odontoma wherein the tumour forms a collection of small structures resembling teeth. On the other hand, an irregular mass with no similarity to teeth is termed as a complex odontoma. There are cases of extensive and multiple compound odontomas which have been identified in either of the jaws. The present case is rare with multiple compound odontomas involving both the jaws of 45-year-old male patient. A review of seven such cases reported so far has been presented.
Hamartoma, Mandible, Maxilla, Odontogenic, Tumour
Case Report
A 45-year-old male patient reported to the Department of Oral Medicine and Radiology with a chief complaint of difficulty in chewing due to missing teeth in upper and lower back tooth region of both the jaws since 20 years duration. The patient’s medical, family and social history were non-contributory. General physical examination showed a healthy-looking male. On intraoral examination, many teeth were lost with remaining root stumps. Bony hard swellings were noticed in the anterior and posterior region of both the jaws with vestibular obliteration. Patient did not complain of any pain and paraesthesia intraorally as well as extraorally. Pigmentation was predominantly observed in the anterior region of both the jaws. Overlying mucosa of the swellings was normal and non-tender on palpation [Table/Fig-1].
Intraoral photograph showing bony hard swellings in the anterior and posterior region of both the jaws.

Panoramic radiography showed diffuse tooth like radio-opacities occupying the medial, lateral wall and floor of the right side of the maxillary sinus, along with similar radio-opacities on the lateral wall and floor of left side of the sinus. In the mandibular region, tooth like radio-opacities were seen overlying each on the right and left inferior alveolar nerve canal and on the symphysis region of the jaw which were surrounded by radiolucent areas and was clearly demarcated from bone [Table/Fig-2].
On panoramic view tooth like radio-opacities seen in both the jaws.

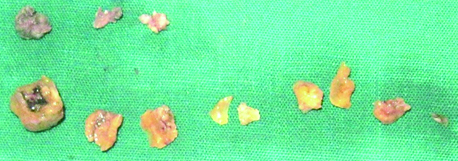
On the basis of clinical and radiographic features, the initial diagnosis of multiple odontomas was made and surgical treatment was indicated. The patient was made aware of the existing pathology and was convinced for surgery. Haematological investigations were within normal range. The biochemical investigations (serum calcium, phosphorus and alkaline phosphatase) levels were also within normal limits. Written informed consent from the patient was obtained prior to the surgical procedure. After the surgical procedure which was performed under general anaesthesia, eleven teeth like structures were removed [Table/Fig-3].
Gross specimen showing eleven tooth like structures.
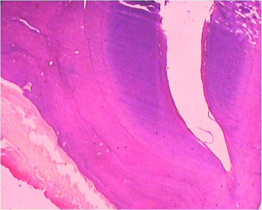
The specimen received for histopathological evaluation were decalcified and showed deposition of dentine and cementum like structures of irregular thickness, along with some areas of pulp tissue [Table/Fig-4]. The patient was followed up for a year, with no evidence of recurrence.
H&E (10x) stained section showing dentin and cementum like structures with small pulp tissue
Discussion
Odontomas are tumours in which complete functional discrepancy of ameloblasts or odontoblasts occur with the development of enamel and dentin but in an irregular arrangement due to the lack of association of these cells to reach a usual state of morpho differentiation. This may be congenital or may occur due to an altered gene or intervention postnatally in the genetic pattern of tooth development. Some studies have focused on the remnants of dental lamina as the major etiological factor, however the exact aetiology of odontomas remains unknown [1]. There are two types of odontoma: complex and compound. A compound odontoma comprises of many separate, small tooth like structures, while a complex odontoma forms an irregular mass of dentin and enamel without likeness to a tooth [2]. Genetic incongruities like Gardner’s syndrome, Hermann’s syndrome, local trauma, infectious or inflammatory processes and numerous other pathological circumstances have been accredited to the causes of odontomas. Abnormalities like oesophageal, pulmonary, aortic stenosis, pneumonia, hepatomegaly and bronchiectasis were described by various authors [3]. Erdogan × et al., reported a patient with mild mental retardation and severe myopia [2]. No definite aetiology was identified in this case. Odontomas are appreciated generally in the second decade of life, but incidentally, it can be found at any age [4–6]. Less than 10% are found in patients over 40 years of age [7]. However, the literature of seven reported cases with multiple compound odontomas showed the age range between first and third decade [Table/Fig-5]. In the present case the patient was in the fifth decade.
Literature review of eight cases including the present case of Multiple compound odontomas involving both the jaws
| Authors | Year | Age (yrs) | Gender | Location | Systemic symptoms | Treatment |
|---|
| Bader G [10] | 1967 | New born | F | Both Jaws | Yes | Surgical excision |
| Malik SA et al., [11] | 1974 | 7 | F | Both Jaws | No | Surgical excision |
| Mani NJ [12] | 1974 | 19 | M | Both Jaws | No | Symptomatic |
| Schimidseder R et al., [13] | 1975 | 4 | M | Both Jaws | Yes | Surgical exicison |
| Ajike SO et al., [4] | 2000 | 15 | F | Both Jaws | No | Surgical exicison |
| Bordini J Jr et al., [3] | 2007 | 17 | M | Both Jaws | No | Surgical exicison |
| Erdogan × et al., [2] | 2014 | 27 | M | Both Jaws | Yes | Symptomatic |
| Gujjar P et al., | 2015 | 45 | M | Both Jaws | No | Surgical excision |
With a slight preponderance of males, the ratio differs between 1.2:1 and 1:1 for compound odontomas [8]. The literature of multiple compound odontomas involving both the jaws have reported three cases in females and five cases including the present case in males [2–4].
The most frequent location of compound odontoma is the anterior region of maxilla [3]. In all the cases, including the present case multiple compound odontomas were seen in both the jaws [Table/Fig-5]. Odontomas are generally asymptomatic lesions that are revealed incidentally during routine radiography. Radiographic aspects of compound odontomas are characteristic. A well-defined radiolucency is usually seen surrounding the calcified structures which resemble teeth. The compound odontomas are associated more often with unerupted teeth [3]. In the present case, similar features were appreciated in the compound odontomas which were revealed in the lower jaw. However, the odontomas located in the maxilla were calcified tooth like structures without the radiolucent periphery occupying the right and left maxillary sinus. Odontomas involving the maxillary sinus may lead to complications such as orbital infections, epidural and subdural emphysema, meningitis, cavernous sinus thrombosis, brain abscess and death [8]. However, in the present case we did not find any such symptoms.
The conservative surgical removal of compound odontomas continues to be the treatment of choice. Out of eight reported cases, two were symptomatically treated to avoid the major reconstruction. Patients were kept under observation and followed up for any symptomatic development, the remaining six cases were treated with complete surgical removal [2]. In the present case eleven odontomas were surgically removed completely. The patient was followed up for a year without any uneventful observation.
As odontomas are often associated with unerupted impacted teeth there could be a possibility of tooth eruption after surgical removal of the lesion. The eruption could occur depending on the presence of tooth buds in the jaw bones. But the prognosis of the eruption of teeth has remained poor. Till date the literature has not reported recurrences. However the lesion may recur if it is incompletely removed at its early soft tissue stage [9].
Conclusion
Odontomas are usually revealed on routine radiography, subsequent growth of odontomas can be related with displacement of teeth, and also the related probable complications like cystic transformation. Although compound odontoma frequently involves a single location and is found in anterior portion of maxilla, they may have multiple and bi-maxillary involvement. The present case shows 11 compound odontomas involving all the four quadrants. Surgical treatment of choice should be conventional, monitored by patient’s follow-up to evade any recurrence.
[1]. Serra-Serra G, Berini-Aytés L, Gay-Escoda C, Erupted odontomas: a report of three cases review of the literatureMed Oral Patol Oral Cir Bucal 2009 14(6):E299-303. [Google Scholar]
[2]. Erdogan ×, ×ztunc H, Evlice B, Altug HA, Günhan ×, Compound odontoma involving the four quadrants of the jaws: a case report and review of the literatureQuientessence Int 2014 45(4):341-44. [Google Scholar]
[3]. Bordini J Jr, Contar CM, Sarot JR, Fernandes A, Machado MA, Multiple compound odontomas in the jaw: case report and analysis of the literatureJ Oral Maxillofac Surg 2008 66(12):2617-20. [Google Scholar]
[4]. Ajike SO, Adekeye EO, Multiple compound odontomas in the facial bones: A case reportInt J Oral Maxillofac Surg 2000 29(6):443-44. [Google Scholar]
[5]. de Oliveira BH, Compound odontoma—diagnosis and treatment: three case reportsPediatr Dent 2001 23(2):151-57. [Google Scholar]
[6]. Yeung KH, Cheung RCT, Tsang MMH, Compound odontoma associated with an unerupted and dilacerated maxillary primary central incisor in a young patientInt J Pediatr Dent 2003 13(3):208-12. [Google Scholar]
[7]. Salgado H, Mesquita P, Compound odontoma- Case reportRev Port Estomatol Med Dent Cir Maxilofac 2013 54(3):161-65. [Google Scholar]
[8]. Guledgud MV, Degala S, Patil K, Keshari D, Multiple extensive complex odontomas of the jawsInt J Dent Sci Res 2014 2(6):128-32. [Google Scholar]
[9]. Reichart PA, Philipsen HP, Odontogenic tumours and Allied lesions 2004 LondonQuintessence Publishing Co Ltd:150-53. [Google Scholar]
[10]. Bader G, Odontomatosis (multiple odontomas)Oral Surg Oral Med Oral Pathol 1967 23(6):770-73. [Google Scholar]
[11]. Malik SA, Khalid M, Odontomatosis (multiple odontomas) - A case reportBr J Oral Surg 1974 11(3):262-64. [Google Scholar]
[12]. Mani NJ, Odontoma syndrome: Report of unusual case with multiple multiform odontomas of both jawsJ Dent 1974 2(4):149-52. [Google Scholar]
[13]. Schimidseder R, Hausamen JE, Multiple odontogenic tumours and other anomaliesOral Surg Oral Med Oral Pathol 1975 39(2):249-58. [Google Scholar]