Rare Co-existence of Squamous Cell Carcinoma with Infiltration of Renal Vein and Xanthogranulomatous Pyelonephritis
K.V. Kanodia1, A.V. Vanikar2, R.D. Patel3, L. K. Nigam4, H. L. Trivedi5
1 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, India.
2 Professor and Head, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, India.
3 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, India.
4 Junior Lecturer, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, India.
5 Professor, Department of Nephrology and Transplantation Medicine and Director, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. K.V. Kanodia, Professor, Department of Pathology, Lab Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases & Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, Gujrat, India.
E-mail: kamalkanodia@yahoo.com, ikdrcad1@sancharnet.in
Primary renal squamous cell carcinoma is a very rare malignancy of the upper urinary tract. Most patients have history of chronic urolithiasis, analgesics abuse, radiotherapy or infection. Co-existence of SCC with xanthogranulomatous pyelonephritis is exceedingly rare with only few reports in the literature. We report a case of a 60-year-old male presented with right flank pain and mild tenderness of abdomen. Computed tomography of the abdomen revealed gross hydronephrosis with parenchymal thinning and irregular thick enhancing wall of pelvicalyceal system with multiple calculi in right kidney. Right renal vein appeared distended, filled with hypo dense material. Right nephrectomy was performed and sent for pathological examination. Histological evaluation revealed keratinizing squamous cell carcinoma with infiltration of renal vein and xanthogranulomatous pyelonephritis.
Hydronephrosis, Kidney, Pelvicalyceal system
Case Report
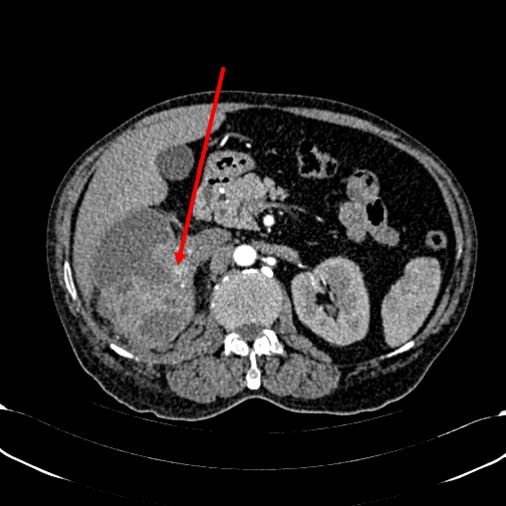
A 60-year-old man presented in urology outpatient department with right flank pain and tenderness on abdominal examination. The patient had no history of haematuria or pyuria. Ultrasonography and computed tomography (CT) of the abdomen revealed gross hydronephrosis with parenchymal thinning and irregular thick enhancing wall of pelvicalyceal system favouring malignancy. CT scan examination also showed no evidence of excretion of contrast after 4 hours suggestive of nonfunctioning kidney. Multiple calculi were observed in the mid and lower calyces. Right renal vein appeared distended, filled with hypo dense material of size 23x14 mm suggesting the possibility of thrombus. The right and left kidney measured 12.8x 8.5 cm and 11.2 x 5.8 cm respectively [Table/Fig-1,2 and 3].
Axial CT scan image of arterial phase shows enhancing irregular thickening of wall of pelviccalyceal system of right kidney (↑)
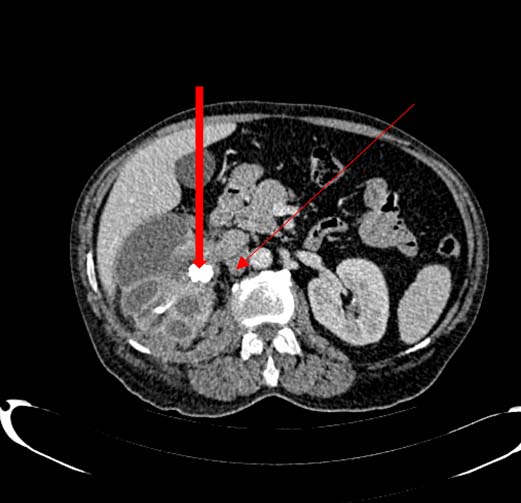
Axial CT scan image of venous phase shows enhancing irregular thickening of wall of pelvic calyceal system (↑) and renal pelvis of right kidney with calculus (↑) in renal pelvis
Coronal CT scan image of venous phase show enhancing irregular thickening of wall of pelvic calyceal system, renal pelvis, upper ureter (↑) on right side with calculi (↑)

On investigation, urine examination revealed 25 mg/dL protein with occasional pus cells /high-power field. Serum creatinine was 1.51 mg/dL, haemoglobin, 7.5 gm/dL and a total leucocyte count of 9120/cmm. The liver function test was within normal limits. Right nephrectomy was performed and sent for pathological examination.
Gross pathological examination revealed enlarged kidney weighing 290 gm, measuring 10×8×7 ccm in size. The outer surface appeared greyish white, with irregular scars and focal yellowish areas. Cut surface showed moderately dilated pelvicalyceal system filled with purulent, necrotic material and multiple calculi, largest staghorn calculi measuring 3×2×2 ccm.
Microscopic examination revealed a malignant tumour comprising of squamous cells arranged predominantly in sheets and nests with areas of keratinization and formation of keratotic pearls. Focal areas of necrosis and lymphocytic infiltration were also evident. The adjacent parenchyma showed focal areas of foamy histiocytes, giant cells, lymphocytes and fibrocollagenous tissue. No normal cortical tissue was identified. Tumour was seen infiltrating the renal vein, however ureter and surgical margins appeared free from tumour invasion [Table/Fig-4,5]. Thus, diagnosis of moderately differentiated keratinizing squamous cell carcinoma of kidney with focal xanthogranulomatous pyelonephritis associated with stone disease was offered.
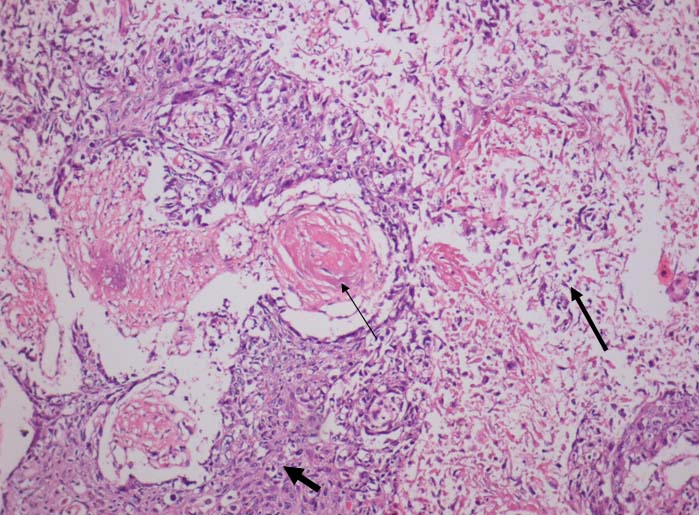
Malignant squamous cells (↑) arranged predominantly in sheets and nests with keratotic pearls (↑) and focal areas of necrosis and lymphocytic infiltration (↑). (H&E,X 100).
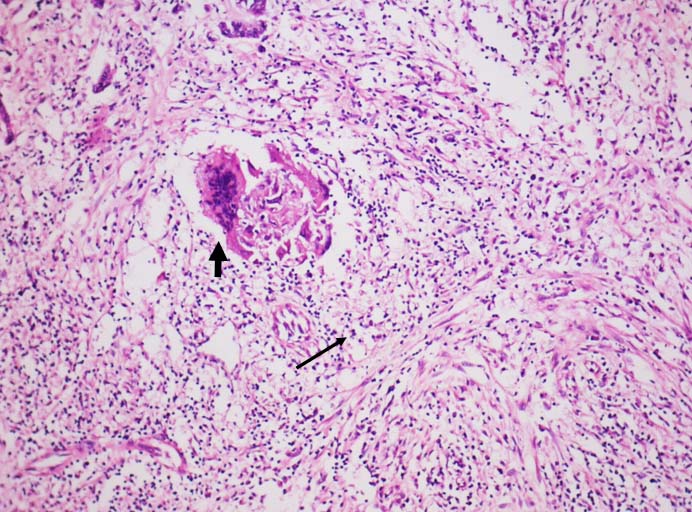
Parenchyma shows focal area of foamy histiocytes (↑) with giant cells (↑), lymphocytic infiltration and fibrocollagenous tissue suggestive of xanthogranulomatous pyelonephritis. (H&E, X 100)
Discussion
Primary malignancies of renal collecting system are rare and account for 4-5 % of all urothelial tumours [1]. Urothelial carcinoma is observed in more than 90% of cases [2]. Primary squamous cell carcinoma (SCC) of kidney is rare with an incidence ranging from 0.5-8% [3,4]. These tumours are moderately to poorly differentiated [2,3].
SCC of urinary tract is commonly seen in urinary bladder and male urethra and is rarely seen in renal pelvis [5,6]. SCC of renal pelvis is rare of all malignancies with an incidence of 1.4% [1,6]. These tumours are usually of high grade and highly aggressive. Most of the cases present as locally advanced or metastatic at the time of presentation with poor prognosis [5]. SCC is frequently associated with stone disease and hydronephrosis [3,7]. Chronic irritation of urothelium leads to squamous metaplasia and SCC [7,8]. The common causes of irritation are chronic renal calculi, phenacetin consumption, radiotherapy or infection [3,9]. Staghorn calculi are most frequently associated with SCC of renal pelvis [10,11]. Solid mass, hydronephrosis and calcification are common but non-specific findings, so the diagnosis of SCC is difficult and is mostly based on histopathological examination as observed in the present case [7,8]. Co-existence of SCC and xanthogranulomatous pyelonephritis (XGP) is rarely reported in literature [3,11,12]. XGP is known to be secondary to lithiasis and rarely leads to SCC [11–13].
Current primary treatment of renal SCC is nephrectomy. Chemotherapy and radiotherapy are indicated in metastatic disease [5,15]. A combination of Cisplatin, Methotraxte and Bleomycin is used for metastatic disease [14,15].
Conclusion
Primary SCC is an aggressive tumour as these tumours have strong association with renal stones and so a non-functioning kidney should be carefully examined with advanced modalities for early diagnosis and management of tumour. Biopsy from the renal pelvis or calyceal wall should be considered during the treatment of stone disease in patients having long standing staghorn calculus. Such patients are susceptible of harboring occult or overt malignancy along with the renal stone disease.
[1]. Murphy DM, Zincke H, Furlow WL, Primary grade I transitional cell carcinoma of the renal pelvis and ureterJ Urol 1980 123:629-31. [Google Scholar]
[2]. Khader FN, Primary Renal Squamous Cell Carcinoma: A Case ReportJCDR 2012 6(4):720-22. [Google Scholar]
[3]. Li MK, Cheung WL, Squamous cell carcinoma of the kindeyJ Urol 1987 138:269-71. [Google Scholar]
[4]. Blacher EJ, Johnson DE, Abdul–Karim FW, Squamous cell carcinoma of renal pelvisUrology 1985 25:124-26. [Google Scholar]
[5]. Karabulut A, Emir L, Gonultas NI, Squamous cell carcinoma located in the renal caliceal system: A case report and review of the literatureTurkish J of Cancer 2002 32(1):20-24. [Google Scholar]
[6]. Odabas O M, Yilmaz Y, Squamaous cell carcinoma of kidneyEastren J of Medicine 2000 5(1):35-36. [Google Scholar]
[7]. Busby JE, Brown GA, Tamboli P, Kamat AM, Dinney CPN, Upperurinary tract tumours with non-transitional histology: a single-centre experienceUrology 2006 67:518-23. [Google Scholar]
[8]. Holmang S, Lele SM, Johansson SL, Squamous cell carcinoma of therenal pelvis and ureter: incidence, symptoms, treatment and outcomeJ Urol 2007 178:51-56. [Google Scholar]
[9]. Lee TY, Ko JF, Wan YL, Renal squamous cell carcinoma: CT findings and clinical significanceAbdom Imaging 1998 23:203-08. [Google Scholar]
[10]. Kaur P, Chauhan A, Singh G, Kataria S, Kalra R, Primary Squamous Cell Carcinoma Of Kidney - A Case Report And Review Of LiteratureThe Internet Journal of Nephrology 2009 6(1) [Google Scholar]
[11]. Mardi K, Kaushal V, Sharma V, Rare Co-existence of keratinizing squamous cell carcinoma with xanthogranulomatous pyelonephritis in the same kidney: report of two casesJ Cancer Res Ther 2010 Jul-Sep 6(3):339-41. [Google Scholar]
[12]. Dhingra KK, Sukard S, Shyama J, Rare Co-existence of keratinizing squamous metaplasia with xanthogranulomatous pyelonephritis: Report of a case with the role of immunocytochemistry in the differential diagnosisActa Cytol 2007 51:92-94. [Google Scholar]
[13]. Yousof A, Alamer A, Fahad A, Renal Squamous Cell Carcinoma Presented With Bone Metastasis and Co-existence with Xanthogranulomatous Pyelonephritis: A Case ReportUrology case report 2014 2(2):35-37. [Google Scholar]
[14]. Lone AR, Aziz SA, Mir MH, Qadri SK, Case Report: Primary Squamous Cell Carcinoma of Kidney-An Unusual MalignancyJournal of Cancer Research Updates 2013 2:220-23. [Google Scholar]
[15]. Corral DA, Sella A, Pettaway CA, combination chemotherapy for metastatic of locally advanced genitourinary squamous cell carcinoma: A phase II study of methotrexate, cisplatin and bleomycinJ Urol 1998 160:1770-74. [Google Scholar]