Background
Dental anxiety is a widespread phenomenon and a concern for paediatric dentistry. The inability of children to deal with threatening dental stimuli often manifests as behaviour management problems.
Nowadays, the use of non-aversive behaviour management techniques is more advocated, which are more acceptable to parents, patients and practitioners. Therefore, this present study was conducted to find out which audio aid was the most effective in the managing anxious children.
Aims and Objectives
The aim of the present study was to compare the efficacy of audio-distraction aids in reducing the anxiety of paediatric patients while undergoing various stressful and invasive dental procedures. The objectives were to ascertain whether audio distraction is an effective means of anxiety management and which type of audio aid is the most effective.
Materials and Methods
A total number of 150 children, aged between 6 to 12 years, randomly selected amongst the patients who came for their first dental check-up, were placed in five groups of 30 each. These groups were the control group, the instrumental music group, the musical nursery rhymes group, the movie songs group and the audio stories group.
The control group was treated under normal set-up & audio group listened to various audio presentations during treatment. Each child had four visits. In each visit, after the procedures was completed, the anxiety levels of the children were measured by the Venham’s Picture Test (VPT), Venham’s Clinical Rating Scale (VCRS) and pulse rate measurement with the help of pulse oximeter.
Results
A significant difference was seen between all the groups for the mean pulse rate, with an increase in subsequent visit. However, no significant difference was seen in the VPT & VCRS scores between all the groups. Audio aids in general reduced anxiety in comparison to the control group, and the most significant reduction in anxiety level was observed in the audio stories group.
Conclusion
The conclusion derived from the present study was that audio distraction was effective in reducing anxiety and audio-stories were the most effective.
Introduction
Despite major advances in dentistry in terms of techniques, technologies and materials, anxiety related to the dental environment and specific procedures is a significant and common problem faced by child patients worldwide and considered as an obstacle in providing quality dental care.
Various aspects and factors are involved in the acquisition and development of dental anxiety in children. It not only concerns fear of pain or of invasive procedures, but also entails separation from the parents, confrontation with unfamiliar people and surroundings and the experience of loss of control [1].
In the Indian population, an estimated 6.3-9.4% of children between the age groups of 10-15 years suffer from dental fear [2]. A vicious cycle has been proposed in relation to dental fear whereby dental fear leads directly to the avoidance of dental visits, resulting in deterioration in oral health, leading to more problem-oriented visiting, which serves to maintain or exacerbate the person’s level of dental fear. This avoidance creates feelings of shame, guilt and inferiority, further maintaining this negative spiral by reinforcing one’s fear and avoidance behaviour [1].
AAPD has outlined a series of behaviour management techniques to deal with the problem, ranging from voice control, to distraction, to physical restraint. When all else fails, sedation with drugs such as nitrous oxide has been advocated [3]. Behaviour management techniques are meant to reduce the need for excessive and potentially unsafe use of medications. There is evidence to indicate that an integration of good behavioural techniques leads to better results, lessened drug requirements, greater patient safety and reduced side-effects [4].
The present trend advocates the use of non-aversive behaviour management techniques which may be equally effective and more acceptable to parents, patients and practitioners. In distraction, the patient’s attention is diverted from what may be perceived as an unpleasant situation [5]. Audio distraction is a non-aversive distraction technique in which patients listen to music or stories during a stressful procedure. The accomplishment of audio distraction technique has been affirmed in medical setups however scanty literature is available to gauge the potency of this technique in terms of paediatric population [2].
Researchers have identified several mechanisms by which music works to reduce anxiety. The first is the Gate Control Theory of Pain, proposed by Ronald Melzack and Patrick Wall in 1965 [6]. This theory states that pain signals are transmitted from the place of injury, via nerve receptors in the spinal cord, to synapses that receive the pain information in the brain. Music is believed to send enough competing sensory inputs through pathways descending from the brain to cause the brainstem to signal some of the gates shut, thereby reducing the amount of pain that the patient listening to the music perceives [7].
A second mechanism is distraction. Noguchi defines this as “any technique which diverts attention from a noxious stimulus, such as the sound of the dentist’s hand instrument scraping across a rough tooth surface”. A final mechanism is masking: music is able to “mask” unpleasant sounds such as the noises of the dental drill thereby averting the patient’s anxiety [8].
Therefore, the aim of this present study is to compare the effect of different audio distraction aids with normal dental set-up and to find out which aid is the most effective in the managing anxious paediatric dental patients.
Materials and Methods
Study Design
The present study was conducted in the Department of Pedodontics and Preventive Dentistry in Saraswati Dental College, Lucknow. It is a comparative interventional study undertaken to compare the effectiveness of various audio distraction aids in reducing anxiety in the dental paediatric patients. The study protocol was approved by the ethical committee. Informed consent was obtained from the parents along with a brief medical & dental history of the child. The duration of the study was 6 months and the sample collection was conducted during the Department’s OPD timings by random sampling method.
Study Population: The present study was carried out in a total number of 150 children, aged between 6 to 12 years, and were selected amongst the patients who came for their first dental evaluation.
Inclusion Criteria
No previous dental experience & hospitalization.
No learning disability.
Not having experienced any harmful events (severe accidents, eye witnessing a crime etc).
Absence of any systemic disease.
Exclusion Criteria
Children with any physical or mental disability.
Children having undergone dental treatment.
Materials Used
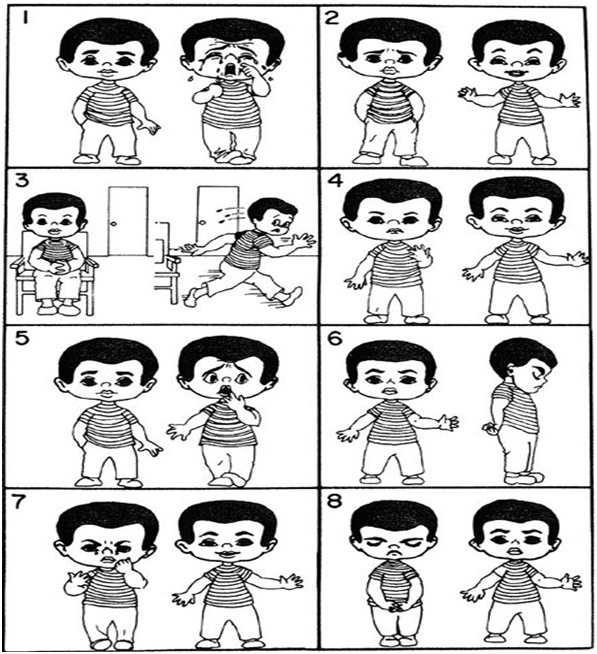
Venham’s Picture Test [Table/Fig-1];
Venham’s Anxiety Rating Scale [9] [Table/Fig-2];
MP3 player [Table/Fig-3];
Headphones [Table/Fig-3];
Audio MP3 files of popular movie songs, instrumental music, nursery rhymes and children stories.
Fingertip Pulse oximeter (NecLife, model number: NL-50D) [Table/Fig-3].
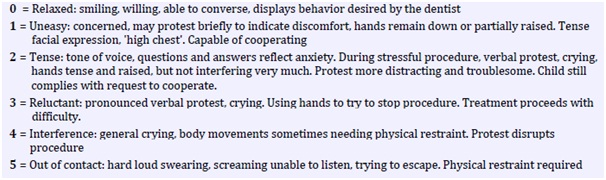
Venham’s Clinical Rating Scale [9]
Materials used for the present study
A. Headphone.
B. Finger Pulse Oximeter (NL-50D).
C. MP3 Player.

Methodology
The patients were randomly assigned to one of the following five groups, in groups of 30 each, on their first visit.
Control group – children treated under normal dental set-up.
Experimental /Audio group – the children were made to listen to various audio presentations throughout the treatment process. This experimental group consisted of four sub-groups including 30 children each :-
Group I – instrumental music group.
Group II – musical nursery rhymes group.
Group III – latest Hindi movie songs group.
Group IV – audio stories group consisting of popular children stories and folk tales.
Treatment Procedure: Each child had four dental visits – first was the screening visit, second oral prophylaxis visit, third cavity preparation and restorative visit and the fourth included procedures performed under local anaesthesia, like extractions, pulpotomies and pulpectomies.
Assessment of Anxiety: Child’s anxiety level in each visit was assessed using a combination of three measures:
Venham’s picture test (VPT) – It’s is a projective, psychometric, self-measure test which is used to measure the state anxiety of the young child. It permits the child to respond non-verbally, minimizing the distortion produced by the subject’s attempt to give socially desirable responses.
It comprises of eight cards, with two pictures in each card, one “anxious” figure and one “non-anxious” figure. The child was asked to point the picture they felt most like at that moment. All the cards were shown in their numbered order. If the child pointed at the “anxious” figure, a score of one was recorded, if the child pointed at the “non-anxious” figure, a score of zero was recorded [10]. Therefore, the scale has a range of zero (minimum score) to eight (maximum score). It is quick to administer in 2 to 3 minutes.
Venham’s clinical anxiety rating scale (VCRS) - used to measure the situational anxiety of the child by the clinician. It is an interval rating scale in which the rating procedure is reliable, valid and can be easily integrated in clinical or research activities. It is a six-point scale, with scale points anchored in objective, specific and readily-observable behaviour [11].
Finger pulse oximeter (NL-50D) – for pulse rate measurement, which is a direct measure of physiological arousal since its increase is attributed to stress during dental procedures [12].
The values were tabulated & subjected to statistical analysis.
Statistical Analysis
The statistical analysis was done using SPSS (Statistical Package for Social Sciences) Version 15.0 statistical Analysis Software. The values were represented in Number (%) and Mean ± SD.
The statistical tests used were Chi square test, Analysis of variance (ANOVA), Student t-test, Paired t-test, Kruskall Wallis H-test & Mann-Whitney U-test.
Results
In the inter-group comparison of the pulse rate [Table/Fig-4] at all the visits, a significant difference in different groups was observed (p<0.001). Except for Group II in which a decrease in mean pulse rate was observed between first and second visits, in all the groups with each subsequent visit an increase in pulse rate was observed which was also significant statistically.
Intergroup comparison of pulse rate at different visits
| Visit No. | Control | Group I | Group II | Group III | Group IV | Statistical significance |
|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | F | p |
|---|
| First visit | 91.27 ± 2.70 | 93.13 ± 0.78 | 92.77 ± 1.76 | 90.33 ± 3.92 | 91.30 ± 2.93 | 5.782 | <0.001 |
| Second visit | 94.13 ± 3.85 | 94.20 ± 2.04 | 92.30 ± 1.49 | 91.50 ± 3.63 | 92.27 ± 3.59 | 4.708 | 0.001 |
| Third visit | 99.10 ± 3.99 | 95.90 ± 2.47 | 96.57 ± 2.65 | 95.17 ± 2.91 | 93.77 ± 3.76 | 11.303 | <0.001 |
| Fourth visit | 106.90 ± 4.79 | 102.47 ± 1.20 | 101.40 ± 2.16 | 102.33 ± 2.94 | 96.93 ± 5.12 | 29.547 | <0.001 |
In the inter-group comparison of VPT [Table/Fig-5], the difference was not statistically significant. In the inter-group comparison, no significant difference in VCRS scores [Table/Fig-6] was observed at any of the visits (p>0.05). At all the visits, mean scores of Control group were maximum.
Intergroup comparison of venham’s picture test at different visits
| Visit No. | Control | Group I | Group II | Group III | Group IV | Statistical significance(Kruskal-Wallis test) |
|---|
| Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | H | p |
|---|
| First visit | 1.70 | 1.44 | 1.00 | 1.73 | 0.94 | 1.00 | 1.50 | 0.82 | 1.50 | 1.60 | 0.93 | 2.00 | 1.53 | 0.90 | 2.00 | 0.517 | 0.972 |
| Second visit | 1.63 | 1.27 | 1.00 | 1.77 | 0.68 | 2.00 | 1.47 | 0.51 | 1.00 | 1.63 | 1.00 | 1.50 | 1.37 | 0.76 | 1.00 | 4.702 | 0.319 |
| Third visit | 1.90 | 1.35 | 2.00 | 1.80 | 0.96 | 2.00 | 1.60 | 0.72 | 2.00 | 1.77 | 1.04 | 2.00 | 1.47 | 0.97 | 1.00 | 1.983 | 0.739 |
| Fourth visit | 2.43 | 1.25 | 2.00 | 2.20 | 1.06 | 2.00 | 2.00 | 0.91 | 2.00 | 2.13 | 0.94 | 2.00 | 1.67 | 1.12 | 2.00 | 7.002 | 0.136 |
Intergroup comparison of venham’s clinical rating scale at different visits
| Visit No. | Control | Group I | Group II | Group III | Group IV | Statistical significance(Kruskal-Wallis test) |
|---|
| Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | Mean | SD | Md | H | p |
|---|
| First visit | 0.80 | 0.76 | 1.00 | 0.83 | 0.79 | 1.00 | 0.77 | 0.63 | 1.00 | 0.83 | 0.75 | 1.00 | 0.90 | 0.71 | 1.00 | 0.526 | 0.971 |
| Second visit | 0.70 | 0.75 | 1.00 | 0.90 | 0.40 | 1.00 | 0.70 | 0.47 | 1.00 | 0.90 | 0.66 | 1.00 | 0.70 | 0.60 | 1.00 | 4.671 | 0.323 |
| Third visit | 0.90 | 0.66 | 1.00 | 0.90 | 0.61 | 1.00 | 0.87 | 0.43 | 1.00 | 1.00 | 0.74 | 1.00 | 0.80 | 0.71 | 1.00 | 1.537 | 0.820 |
| Fourth visit | 1.20 | 0.66 | 1.00 | 1.20 | 0.66 | 1.00 | 1.10 | 0.66 | 1.00 | 1.37 | 0.56 | 1.00 | 1.00 | 0.69 | 1.00 | 4.427 | 0.351 |
Discussion
In the Indian population, very few studies have been undertaken to evaluate the efficacy of audio distraction in the management of dental anxiety. These studies used instrumental music or nursery rhymes, either separately or together. There is a deficit of literature on the use of popular movie songs to which the children are more familiar with or children stories.
Anxiety measurement was done by both objective and subjective means. The subjective measures used were the Venham Picture test and Venham Clinical Anxiety Rating scale. The objective measure of anxiety was done by measuring pulse rate with the help of a pulse oximeter.
The pulse rate is governed by the nervous system, especially the autonomic nervous system (ANS) which reflects negative emotions in terms of physiological parameters such as heart rate, respirations and body temperature [13]. Therefore, physiological responses of the ANS are indicators used to tell if a person is under stress or relaxation.
In the present study when the self-reported anxiety between control group and audio distraction groups was compared, statistically no significant difference in VPT score was observed in all the visits [Table/Fig-5]. When anxiety was measured with Venham’s clinical rating scale, again no significant difference was found between different groups [Table/Fig-6]. Thus the observations from this study indicated that Venham’s picture test and Venham’s clinical rating scale gave statistically inconclusive results. Despite the inconclusive results, the picture test was an effective measure of the emotional state of the child at that particular instance. This observation was similar to the earlier observations made by Venham et al., and Alwin et al., [14,15].
In addition to psychological measures, a physiological measurement of anxiety was also made by recording pulse rate using pulse oximeter. Since vasoconstriction or pain can cause a change in heart rate, it is important to compare pulse rate during each visit/immediately after the treatment session. Pulse rate is a direct measure of physiological arousal and its increase is attributed to stress during dental procedures because of which it is an index of patient’s response to dental stimuli [16].
Statistically significant results were observed with the pulse rate measured [Table/Fig-4]. When both the control and audio groups were compared, the increase of the anxiety level for the audio groups was less than the control group. For nursery rhymes, songs and stories group, statistically significant difference was found as compared to the children treated in normal dental set-up [Table/Fig-7]. Our findings are partially concurrent with the study of Prabhakar et al., in which audio music distraction was slightly better in managing anxiety, though, not to a statistically significant level [17]. However, they did not mention the type of music employed in their study.
Intergroup comparison for combined visits
| Visit No. | Control A | Group I B | Group II C | Group III D | Group IV E | Statistical Significance ("p" value) |
|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | A-B | A-C | A-D | A-E | B-C | B-D | B-E | C-D | C-E | D-E |
|---|
| Pulse rate | 97.85 | 7.09 | 96.43 | 4.03 | 95.76 | 4.20 | 94.83 | 5.77 | 93.57 | 4.43 | 0.218 | 0.018 | <0.001 | <0.001 | 0.861 | 0.129 | <0.001 | 0.648 | 0.011 | 0.333 |
| VPT | 1.92 | 1.35 | 1.88 | 0.93 | 1.64 | 0.78 | 1.78 | 0.99 | 1.51 | 0.94 | 0.394 | 0.318 | 0.924 | 0.056 | 0.100 | 0.637 | 0.083 | 0.257 | 0.237 | 0.381 |
| VCRS | 0.90 | 0.73 | 0.96 | 0.64 | 0.86 | 0.57 | 1.03 | 0.70 | 0.85 | 0.68 | 0.693 | 0.851 | 0.143 | 0.680 | 0.246 | 0.441 | 0.203 | 0.060 | 0.796 | 0.058 |
Instrumental music was ineffective in reducing anxiety in the children when compared with the control group receiving no audio distraction. Similar finding was also observed by Aitkin et al., where the relaxing music consisting of slow, lulling instrumental music had no effect in reducing anxiety in the children [18]. Our results did not agree with that of Parkins’ who found a reduction in anxiety with “light orchestral popular music” [19].
Songs and nursery rhymes were more effective as compared to the instrumental music in the present study, even though not to a statistically significant level. The probable reason could be that the children are more familiar with the songs and nursery rhymes, therefore listening to them were not a new experience. Only the latest popular Hindi movie songs to which children are more exposed and musical nursery rhymes were used in the present study. Children are usually not familiar to the instrumental music since it is not a popular style of listening to music in our society, moreover, it could have been uninteresting, dull and monotonous without lyrics for the child. These explanations might reveal less significant impact of instrumental music in reducing anxiety as compared to songs and nursery rhymes.
Audio stories distraction was most effective in reducing anxiety for children undergoing dental treatment in the current study. It is difficult to compare our investigation with the previous studies because scanty literature is available on the use of audio-stories for anxiety reduction in dental settings. One study, conducted by Ingersoll et al., found that audio-stories significantly reduced the un-cooperative behaviour of the paediatric dental patient; however no considerable effect on the anxiety level was found [20]. They proposed that since their study subjects were not highly anxious, substantial changes in the anxiety by distraction was not possible.
The superior results with the audio-stories can be explained on the fact that while listening to stories, children becomes more engrossed & concentrate more on the audio story presentations, thus diverting their attention from the anxiety causing dental stimuli. Since they often close their eyes to concentrate more on the story, the sights and sounds of the dental treatment are screened out, leading to further reduction of anxiety.
A pattern of increase in the anxiety of the children was observed as the severity and invasiveness of the dental procedure increased but to a lesser level in audio distraction groups particularly in the audio-stories group. For all the groups, increased level of anxiety was observed in the third and the fourth visit i.e. restoration visit and the visit involving local anaesthesia, respectively. The reason for increased anxiety in the restorative visit is the sight, sound and sensation of the air-rotor hand-piece while doing cavity preparation. For the fourth visit, the sight and prick of the needle, the feel of the anaesthetic solution inside the mucosa, the endodontic as well as extraction procedure were the most anxiety causing factors. Similar observations were obtained in the previous studies [2,21,22]. Baldwin also witnessed extraction to be the most stressful dental procedure [23].
However, further research is required with greater sample size, involving younger age group children, giving choice of the audio to the subjects and efficacy of other distraction methods such as audio-video distraction.
Limitations
Like any other technique, certain limitations are also faced by the clinician while using audio distraction procedure. The audio presentation may hamper communication and interaction between the patient and the dentist. This may prevent building of proper rapport between the clinician and patient. However, this can be avoided if the volume of the audio presentation is adjusted to such a level that proper masking of the sound of the dental operatory instruments occurs and the patient is also able to properly receive the instructions from the dentist. Thus audio distraction should be used as an adjunct along with other well established behaviour management techniques.
Conclusion
Various conclusions were drawn from the study. Dental anxiety was commonly observed during all the dental procedures. Stories, songs and nursery rhymes were significantly more effective in managing anxiety as compared to the children treated in normal setup. Amongst these, audio-stories distraction was most effective. Within all the groups and with the visit progression, a pattern of an increase in the anxiety of the children was observed as the severity and invasiveness of the dental operating procedures increase but to a lesser level in audio distraction group, particularly in the audio stories group as compared to the control group.
[1]. Ten Berge M, Dental fear in children: prevalence, etiology and risk factors [PhD thesis] 2001 AmsterdamUniversity of Amsterdam[cited 2001 July 5]. Available from: Digital Academic Repository of University of Amsterdam [Google Scholar]
[2]. Naithani M, Viswanath D, Child’s Dental Anxiety: Management by Audio and Audiovisual Distraction Technique - A Comparative StudyUniv Res J Dent 2014 4(2):101-07. [Google Scholar]
[3]. Aartman IHA, van Everdingen T, Hoogstraten J, Schuurs AHB, Appraisal of Behavioral Measurement Techniques for Assessing Dental Anxiety and Fear in Children: A ReviewJ Psychopathol Behav Assess 1996 18(2):153-71. [Google Scholar]
[4]. Foreman PA, Practical patient management: The integrated approachAnesth Prog 1988 35(1):19-25. [Google Scholar]
[5]. American Academy of Paediatric Dentistry: Guideline on behaviour guidance for the paediatric dental patient. Reference manual;36(6):14/15. Available from : http://www.aapd.Org/media/Policies_Guidelines/G_BehavGuide.pdf [Google Scholar]
[6]. Melzack R, Wall PD, Pain mechanisms: a new theoryScience 1965 150(3699):971-79. [Google Scholar]
[7]. Hus A. Music: An Analgesic? The relationship between music therapy & post-operative pain management [internet]. 2007 [cited 2007 Sept 24]. Available from: http://healthpsych.psy.vanderbilt.edu/web2007/MusicPain.htm [Google Scholar]
[8]. Terpack S, Granbois A, Soothing dental anxiety: Music therapy & the dentally anxious patientAccess 2014 28(1):14-15. [Google Scholar]
[9]. Afsar H, Nakhjawani YB, Mahmoudi-Gharaei J, Paryab M, Zadhoosh S, The effect of parental presence on the 5 year old children’s anxiety & cooperative behaviour in the first & second dental visitIran J Paediatr 2011 21(2):193-200. [Google Scholar]
[10]. Shetty RM, Khandelwal M, Rath S, RMS Pictorial Scale (RMS-PS): An innovative scale for the assessment of child’s dental anxietyJ Indian Soc Pedod Prev Dent 2015 33(1):48-52. [Google Scholar]
[11]. Venham LL, Gaulin-Kremer E, Munster E, Bengston-Audia D, Cohan J, Interval rating scales for children’s dental anxiety and uncooperative behaviorPaediatr Dent 1980 2(3):195-202. [Google Scholar]
[12]. Marwah N, Prabhakar AR, Raju OS, Music distraction – It’s efficacy in management of anxious paediatric dental patientsJ Indian Soc Pedod Prev Dent 2005 23(4):168-70. [Google Scholar]
[13]. Kreibig SD, Autonomic nervous system activity in emotions: a reviewBiol Psychol 2010 84(3):394-421. [Google Scholar]
[14]. Venham LL, Quatrocelli S, The young child’s response to repeated dental proceduresJ Dent Res 1977 56(7):734-38. [Google Scholar]
[15]. Alwin NP, Murray JJ, Britton PG, An assessment of dental anxiety in childrenBr Dent J 1991 171(17):201-07. [Google Scholar]
[16]. Yelderman M, New W, Evaluation of pulse oximetryJ Anesth 1983 59(4):349-52. [Google Scholar]
[17]. Prabhakar AR, Marwah N, Raju OS, A comparison between audio and audio-visual distraction techniques in managing anxious paediatric dental patientsJ Indian Soc Pedod Prev Dent 2007 25(4):177-82. [Google Scholar]
[18]. Aitken JC, Wilson S, Coury D, Moursi AM, The effect of music distraction on pain, anxiety and behavior in paediatric dental patientsPaediatr Dent 2002 24(2):114-18. [Google Scholar]
[19]. Parkins SF, The effect of ambient music upon the reactions of children undergoing dental treatmentsASDC J Dent Child 1981 48(6):430-32. [Google Scholar]
[20]. Ingersoll BD, Nash D, Gamber C, The use of contingent audiotaped material with paediatric dental patientsJ Am Dent Assoc 1984 109(5):717-19. [Google Scholar]
[21]. Moore R, Birn H, Kirkegaard E, Brodsgaard I, Scheutz F, Prevalence and characteristics of dental anxiety in Danish adultsCommun Dent Oral Epidermiol 1993 21(5):292-96. [Google Scholar]
[22]. Eitner S, Wichmann M, Paulsen A, Holst S, Dental anxiety – an epidemiological study on its clinical correlation and effects on oral healthJ Oral Rehabil 2006 33(8):588-93. [Google Scholar]
[23]. Baldwin DC, An investigation of psychological and behavioral response of dental extractions in childrenJ Dent Res 1966 45(6):1637-51. [Google Scholar]