Case Series
Case 1
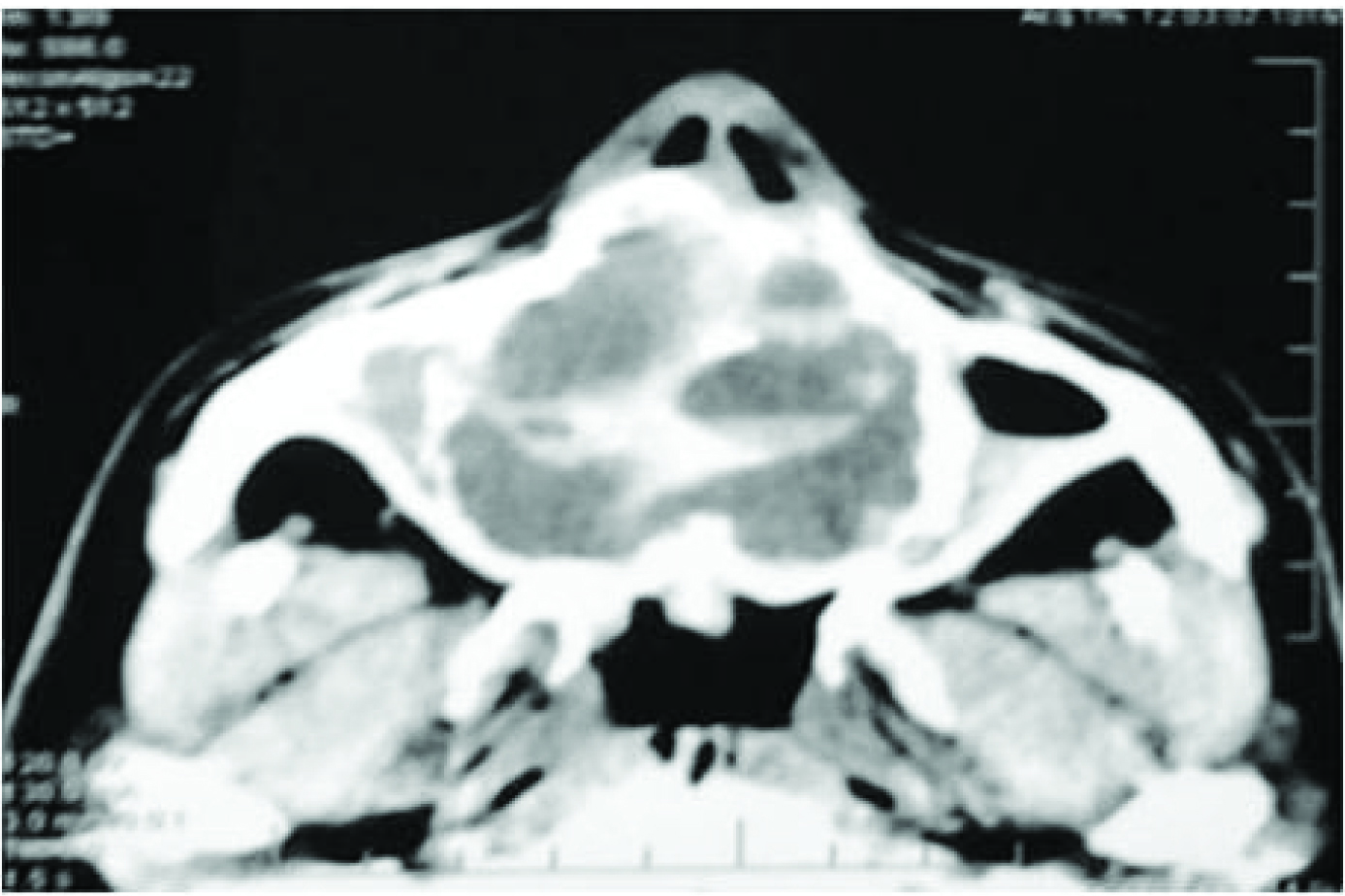
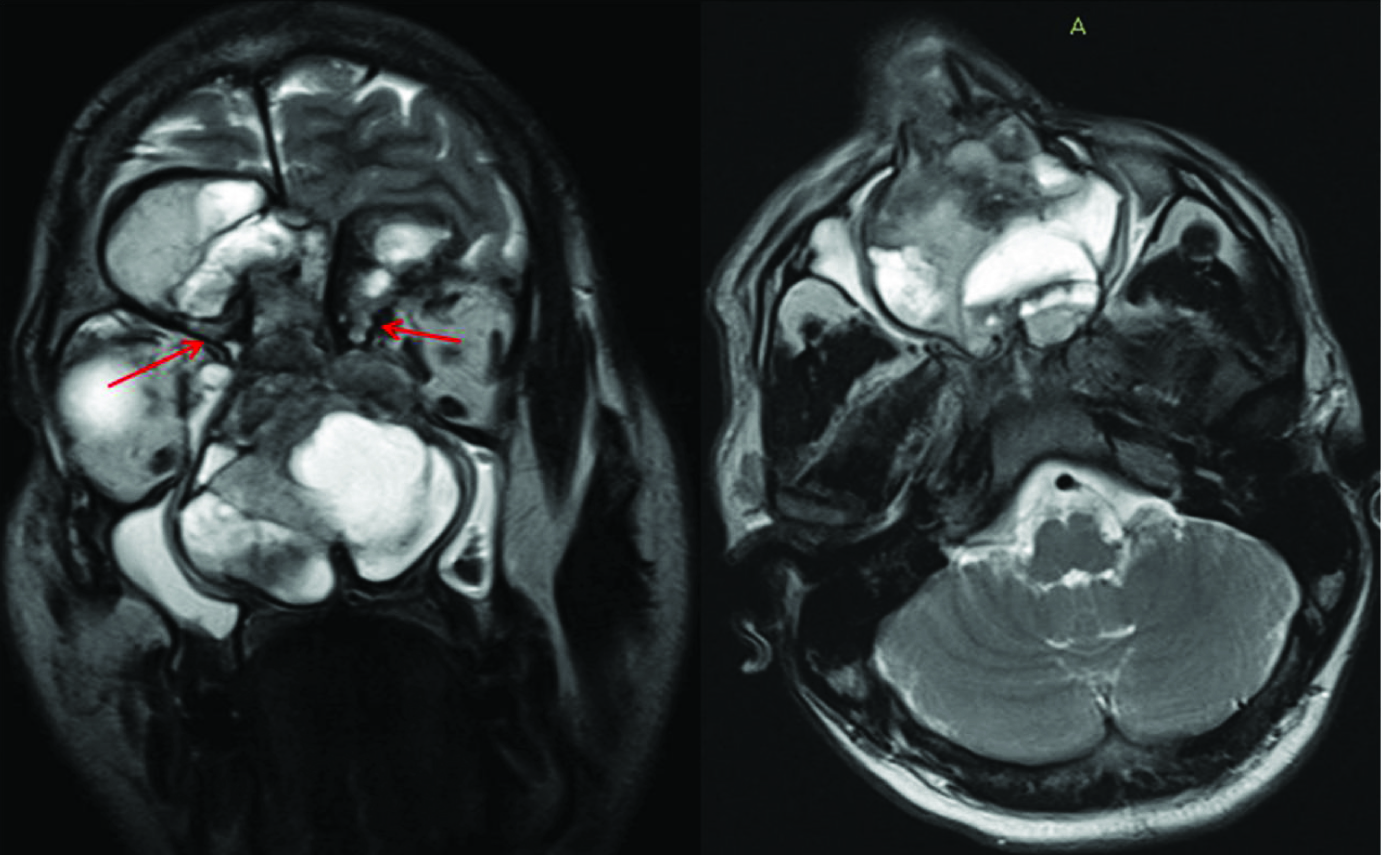
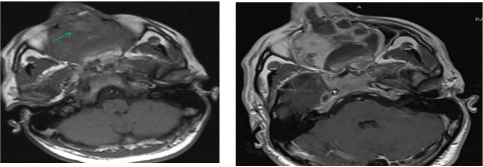
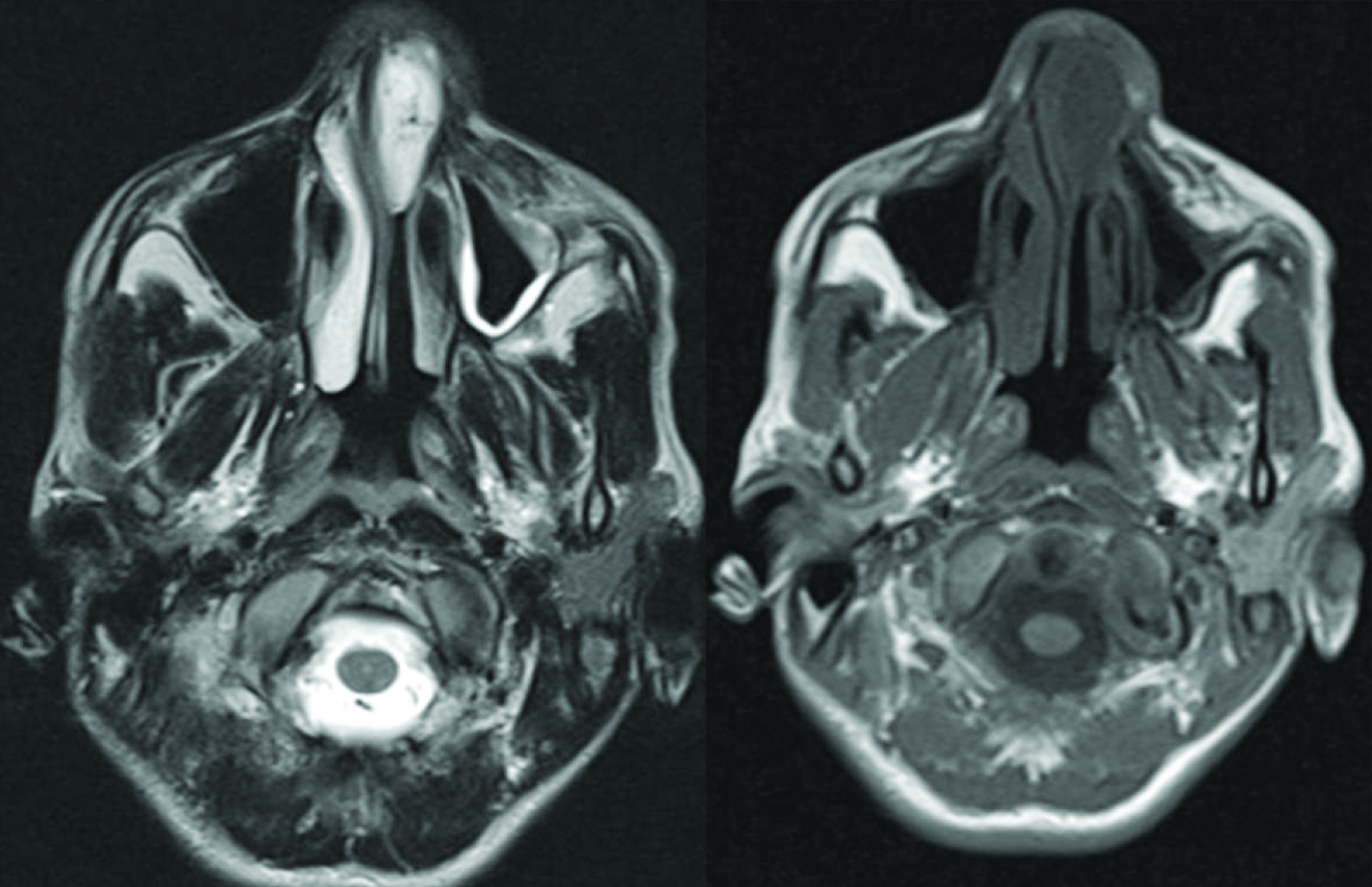
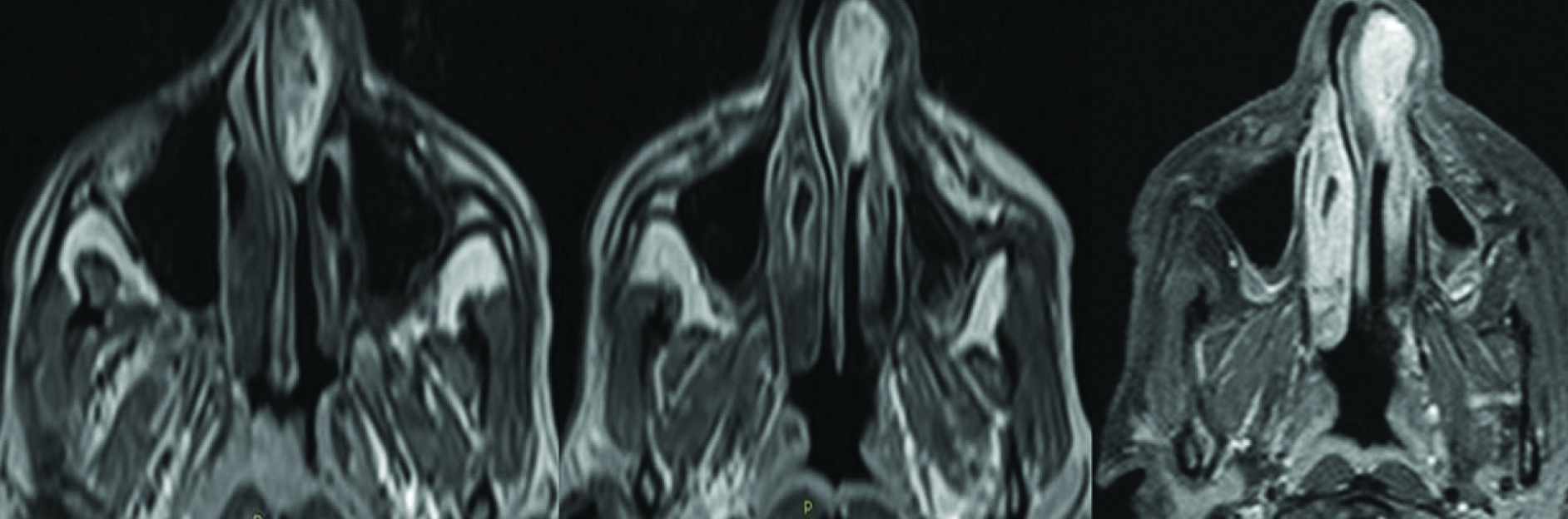
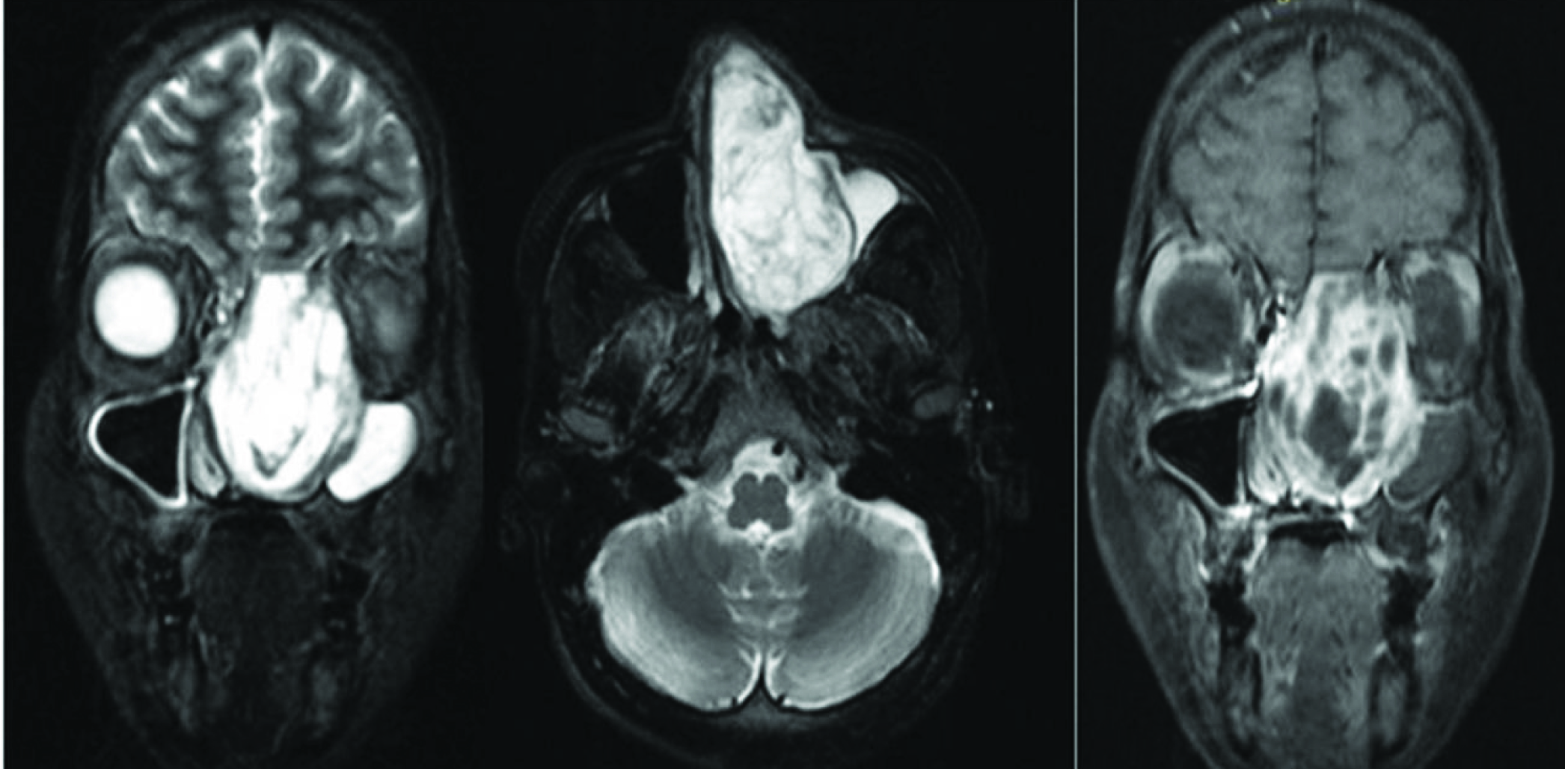
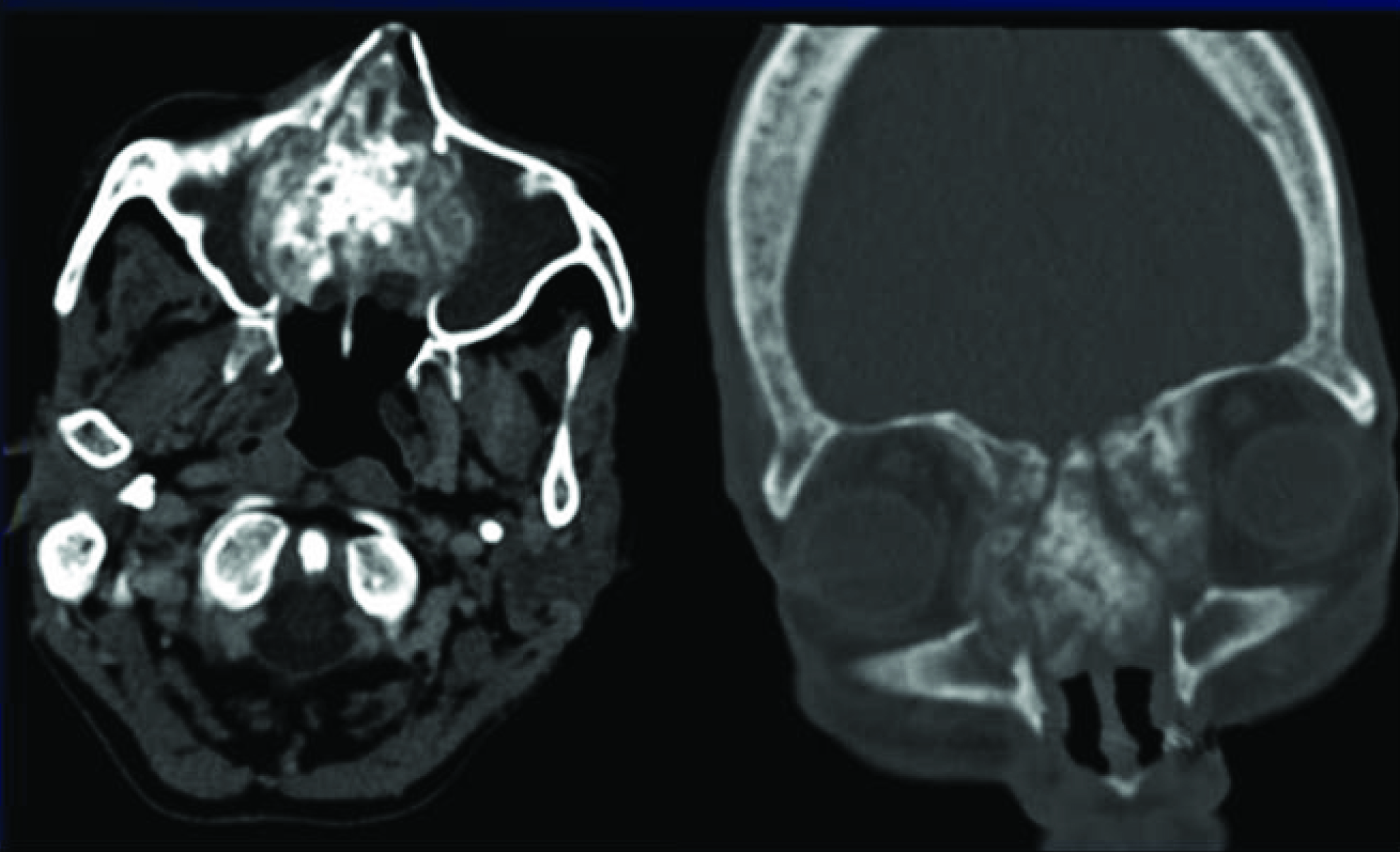
A 25-year-old male presented with pain in eyes, increasingly disfiguring nasal swelling with stuffiness for last 10 months. He also reported two episodes of mild epistaxis in last 10 months which resolved spontaneously. On examination bilateral mild proptosis of eye balls was seen with a large partially necrotic mass seen distending both nasal cavity. There was associated swelling over cheek as well. Noncontrast CT scan [Table/Fig-1] revealed an expansile lytic heterogeneous mass causing gross expansion of the nasal cavity and destruction of the turbinates, nasal septum with multiple high density blood fluid levels. MRI was done subsequently with administration of contrast. The mass revealed a heterogeneous signal on T2W images [Table/Fig-2] involving bilateral nasal cavities with extension into frontal and ethmoid sinuses. There was gross expansion of the sinonasal cavity with preserved peripheral dark cortical line on T2W images (red arrows in [Table/Fig-2]). Fluid fluid levels with signal corresponding to subacute blood product seen within the lesion on T1W images [Table/Fig-3a]. Multiple loculations and septations with heterogenous predominately peripheral enhancement seen on post Gadolinium images [Table/Fig-3b]. Differential diagnoses of Giant cell tumour, Aneurysmal bone cyst and Fibro-osseous tumour were made based on the radiological findings. The patient underwent excision of the mass lesion with reconstruction of the medial wall and roof of the orbit. Histopathological examination revealed fibrovascular rich stroma with occasional fibroblasts and organized thrombuses and fibrin degradation products, features consistent with aneurysmal bone cyst.
Axial CT scan reveals an expansile lytic lesion invoving ethmoid sinuses and nasal acvity with multiple high density fluid levels
Coronal and Axial T2Wimages reveals a heterogeneous signal expansile mass involving ethmoid sinuses and nasal cavities with preserved dark cortical line peripherally (red arrows). Multiple fluids –fluid levels are seen within the lesion
(a) Axial pre contrast T1W reveals multiple blood–fluid levels within the lesion (green arrows). (b) Heterogeneous enhancement of the septations and peripheral rim was seen on post contrast T1W images
Case 2
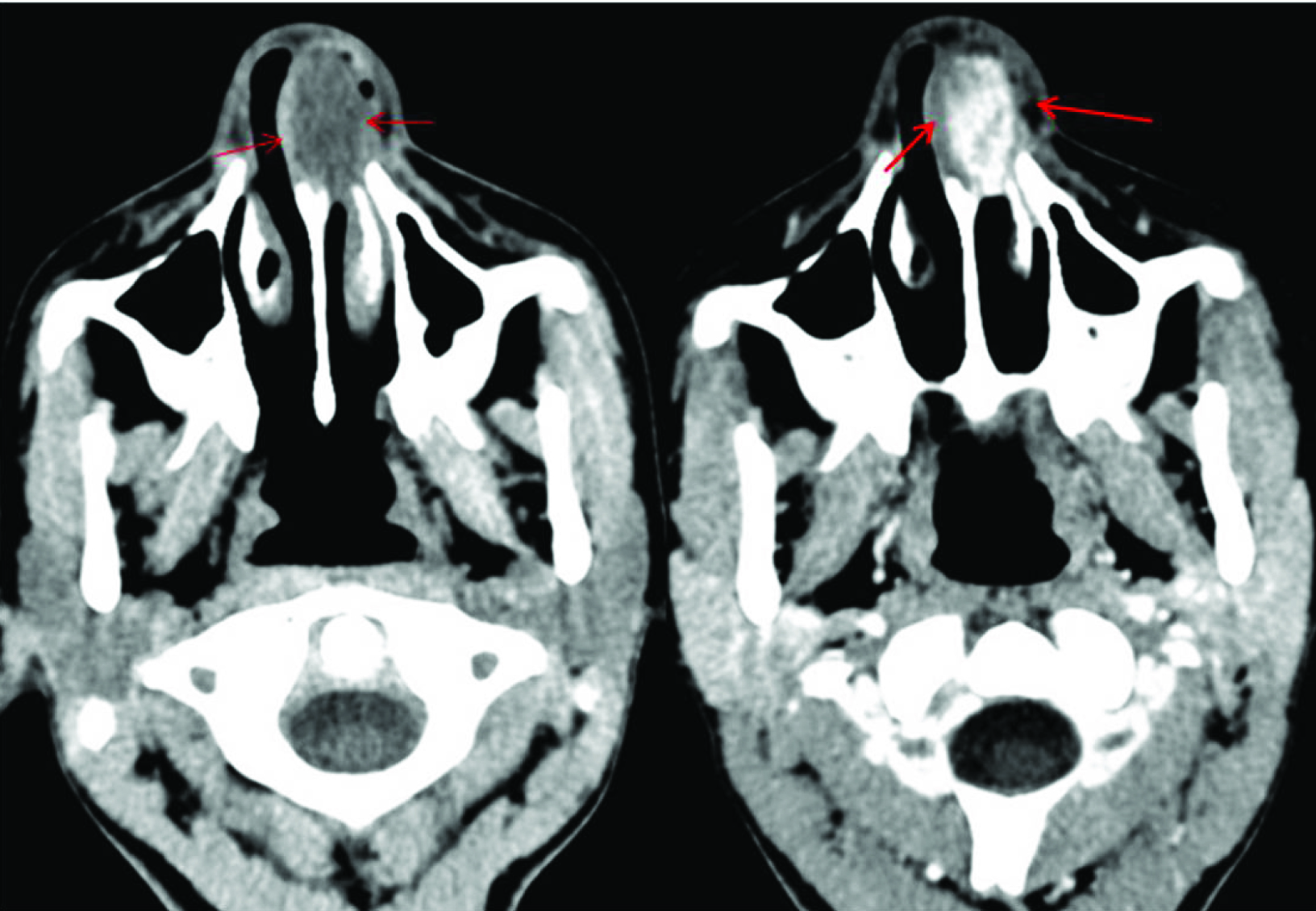
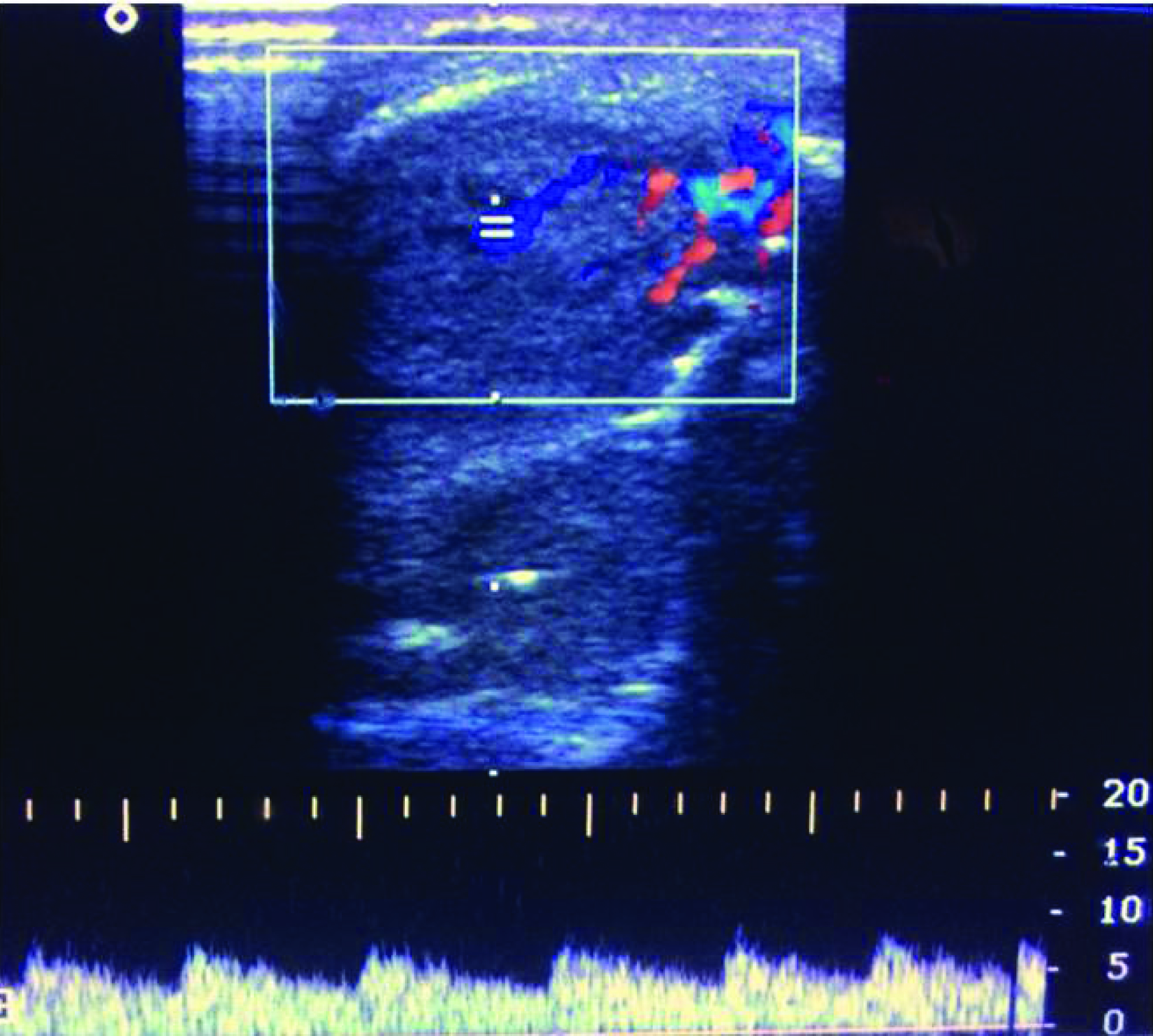
A 17-year-old boy presented with a polypoidal mass lesion prolapsing through the left nostril and with intermittent history of bleed from nose for last 2 years. On anterior rhinoscopy soft friable reddish to brown mass seen filling the left nasal cavity which showed punctuate areas of bleeding on probing. Other biochemical and hematological examinations were unremarkable. Non contrast and contrast enhanced CT scan of the nose and paranasal sinuses [Table/Fig-4] showed a globular soft tissue density lesion in left nasal cavity with avid postcontrast enhancement. Few air foci interspersed over the superficial ulcers on the mass and the nasal alae can also appreciated in the periphery in [Table/Fig-4]. No evidence of destruction of the turbinates or sinonasal bony walls noted with no extension of the mass beyond the nasal cavity. Colour and spectral Doppler of the exposed part of the mass lesion identified few areas of arterial supply with large echogenic soft tissue component [Table/Fig-5]. On MRI the mass showed intrinsic high T2W signal [Table/Fig-6]. Due to high index of suspicion of a presumptive vascular lesion based on CECT images a dynamic contrast study was done in MR which revealed punctuate peripheral enhancement of the lesion on earlier arterial phases with progressive filling in on delayed scans [Table/Fig-7], features in keeping with similar enhancement kinetics of haemangioma identified elsewhere in the body. Based on the enhancement patterns and Doppler findings with clinical history a provisional diagnosis of cavernous haemangioma was made which was confirmed on post surgical Histopathlogical examination.
Axial pre and post contrast CT scan images reveal an avidly enhancing lobulated soft tissue mass within the left nasal vestibule (red arrows)
Colour and spectral Doppler interrogation of the lesion shows arterial type flow with soft tissue component
The mass within the left nasal vestibule demonstrates high T2W and low T1W signal
On dynamic contrast enhanced axial MRI images the mass in left nasal vestibule reveals progressive centripetal enhancement
Case 3
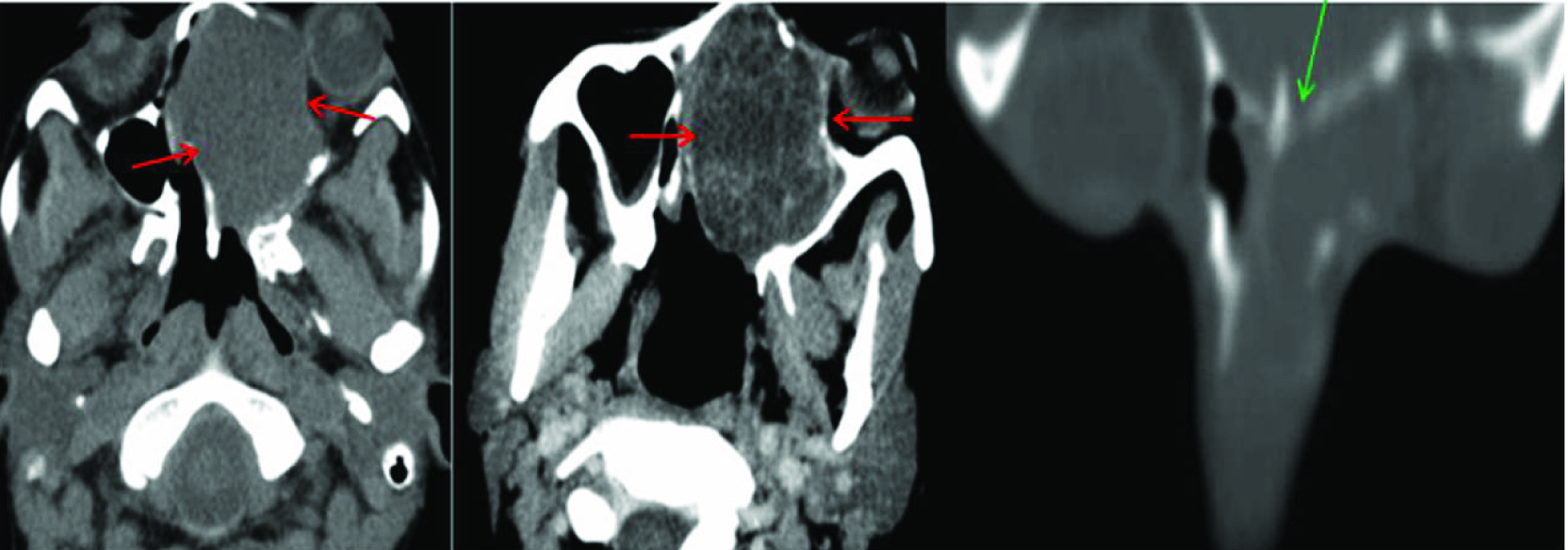
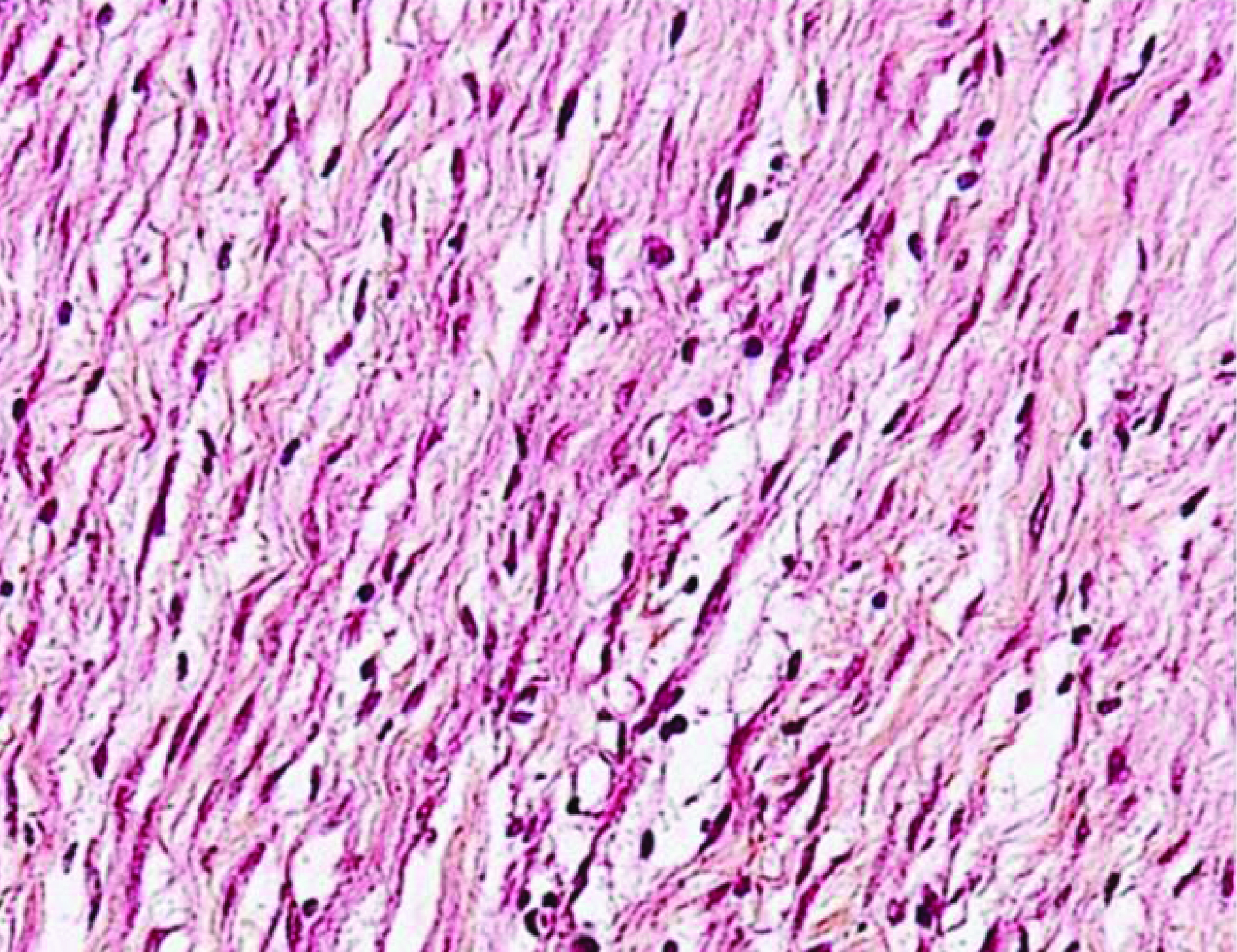
A 24-year-old female presented with slowly progressive nasal obstruction for last one year associated with headache. On examination a smooth polypoidal mass was seen completely filling the left nasal cavity and prolapsing through the left nostril. An area of superficial ulceration seen over the inferior aspect of the mass, however no evidence of bleeding seen on probing. A contrast enhanced CT and MRI examinations were done as preoperative investigations. On CT scan a hypodense mass was seen in left nasal cavity heterogeneously enhancing on post contrast study([Table/Fig-8] red arrows) with cystic spaces inside deviating the nasal septum towards right side and bone remodeling without any intra orbital or intra cranial extensions. Bone window shows no evidence of bone destruction with intact cribriform plate (green arrow in [Table/Fig-8]). On MRI the mass shows bright signal on T2W image, enhancement of the septations on post contrast images with no intra orbital/cranial invasion [Table/Fig-9]. Postoperative histopathology after conservative resection of the mass showed elongated spindle cells arranged in fascicles without encapsulation or any nuclear atypia [Table/Fig-10] and stained positive for S 100 on immunohistochemistry confirming the lesion to be schwannoma.
CT scan shows a hypodense mass in left nasal cavity heterogeneously enhancing on post contrast study (red arrows) deviating the nasal septum towards right side and bone remodelling. Coronal Bone window shows no evidence of bone destruction with intact cribriform plate (green arrow)
The mass shows bright signal on T2W axial and coronal images, showing enhancement of the septations on post contrast coronal images. Fluid collection seen in an obstructed left maxillary sinus
High power microscopy image of histopathological specimen showed uniformly elongated spindle cells in fascicles without nuclear atypia
Case 4
A 60-year-old female presented with nasal swelling with pain in cheek and eyes along with dimness of vision for last 3 months. Anterior rhinoscopy revealed a necrotic mass distending the nasal cavity with destruction of the turbinates. NCCT revealed a heterogeneous solid mass lesion with destruction of the ethmoid sinuses, nasal septum, turbinates and the lamina papyracea laterally with extension on either maxillary sinus [Table/Fig-11] however no intracranial/orbital invasion was seen. Some woven new bone formation was identified within the tumour. Patient underwent an endoscopic biopsy from the lesion which revealed spindle shaped cells with high mitotic index and lobular islands of osteoid consistent with osteosarcoma. MRI was planned to determine the exact extent of the lesion but patient was referred to a dedicated cancer referral centre and was lost to follow up.
Axial and Coronal CT scan shows Heterogeneous mass with abnormal areas of ossification centred in the nasal cavity with permeative lytic destruction of the turbinates, septum, lamina papyracea
CT was performed in all cases in 40 slice Philips Brilliance scanner with 3mm section thickness 5mm collimation, pitch 1.5, Kv 120, mAs100-120. Raw data was reconstructed to 1mm section thickness in dedicated work station. IV contrast material (iohexol, 300/100, 1.5 mg/kg) was administered in 3 patients and all images were studied using both soft-tissue and skeletal window settings.
In 3 out of the 4 cases MRI was performed in a 1.5 Tesla Siemens Magnetom Symphony scanner with 4mm thick slices and 2mm interslice gap. All standard sequences were included including post contrast sequences. Doppler findings have been detailed in regard to the sinonasal haemangioma case. The masses were studied based on their gross and internal morphology, density heterogeneity on CT scan, signal characteristics on MRI with enhancement pattern and locoregional extension [Table/Fig-12]. The morphological characteristics on imaging have been graded in to mild, moderate and diffuse type based on the presence of the particular radiological feature being present in one third, less than two third and more than two–third of the tumour respectively. While aneurysmal bone cyst and Schwannoma exhibited a predominant cystic component, haemangioma and sinonasal Osteosarcoma were largely solid. Internal septaions, fluid-fluid levels were better identified on MRI. Schwannoma, haemangioma showed a uniform bright T2 signal while heterogeneous signal with hypointense areas was seen in aneurysmal bone cyst due to organized chronic blood products. Destruction with variable amount of remodeling was seen in both Osteosarcoma and aneurysmal bone cyst while Schwannoma showed only expansion of the sinonasal cavity and the bony changes in haemangioma was inconspicuous (may be owing to the small size of the lesion).
Comparison of the masses based on CT scan, signal characteristics on MRI.
| Cases | Sinonasal schwannoma | Sinonasal ABC | Sinonasal Hemangioma | Sinonasal Osteosarcoma |
|---|
| Morphological Features | MDCT | MRI | MDCT | MRI | MDCT | MRI | MDCT |
|---|
| 1. Cystic/solid component | Predominantly cystic (fluid attenuation) | Predominatly cystic | cystic> solid | cystic>> solid | solid | solid | solid |
| 2. Internal septations | + | ++ | + | ++ | - | - | - |
| 3. Enhancement pattern | Peripheral and septal | Peripheral and septal | Peripheral and septal | Heterogeneous, Peripheral and septal | ++, diffuse | +++, progressive centripetal | N.A |
| 4. Fluid –fluid levels | - | - | ++ | +++ | - | - | - |
| 5. Calcification | - | - | - | - | - | - | +++ |
| 6. Destruction /Remodelling of sinonasal bony wall/septum/turbinates | Remodelling ++Destruction -ve | Remodelling ++Destruction - | Remodelling ++Destruction + | Remodelling ++Destruction + | Remodelling +Destruction - | Remodelling +/-Destruction - | Remodelling -Destruction +++ |
| 7. Locoregional extent/invasion (F-frontal, E-ethmoid, M-maxillary, S-sphenoid, N-nasalcavity,NP-nasppharynx,O-orbit) | F +,E+,N +,S-,M –,O - | F +,E+,N +,S-,M –,O - | F +,E+,N +,S-,M –,O - | F +,E+,N +,S-,M –,O - |
-ve -Absent, +ve-mild/focal (comprising less than one third of the lesion), ++ve-moderate/intermediate (comprising more than one third but less than two third of the lesion), +++ve-diffuse/severe(comprising more than two third of the lesion), N.A-Not applicable
Discussion
A wide range of tumours may be seen in the sinonasal cavity arising from a variety of tissues (bone, cartilage, muscle, vessel, nerves, lymphoid). The incidence of sinonasal masses is estimated to be 1 in 1,00,000 people per year with half being benign in nature [1,2]. Due to similar clinical presentation of tumours and inflammatory processes, the diagnosis of a mass lesion often requires cross sectional imaging. The purpose of our review is to present special radiological features of few rare sinonasal masses on cross-sectional images, to discuss the differentials, correlate them histopathologically and to familiarize radiologists with these atypical radiological patterns to make more confident and prompt diagnosis.
Sinonasal ABC
Aneurysmal bone cysts (ABC) are benign lesions mostly involving the metaphyses of long bones in immature skeleton with sporadic involvement of head and neck region (2%) [3]. In head and neck most common site is mandible (66%) followed by maxilla (33%) with involvement of sinonasal and orbito ethmoid region being extremely rare and very few cases cited in literature [3,4]. Majority (approximately 90%) lesions occur by first two decades of life with a female preponderance [5].
Histologically, ABC is classified into two main forms: A more common classic form (95%) where the lesion is made up of blood filled clefts among bony trabeculae associated with osteoid matrix and a more rare solid form (5%)-characterized by osteoid production, fibroblastic proliferation and degenerating fibromyxoid calcified elements [6]. The pathogenesis of the lesion over time is divided into three phases by Buraczewski and Dabska et al., namely an intial phase of osteolysis, followed by growth and expansion of the lesion and finally a stabilization phase [6].
ABC appears as a submucosal expansile lesion on clinical and endoscopic examination complicated by areas of haemorrhage and ulceration. Patients may present with a wide varying range of complaints from a disfiguring slowly growing mass with proptosis or dimness of vision (due to mass effect) and occasional episodes of epistaxis [3,7].
Radiological findings in aneurysmal bone cyst closely parallel the macroscopic pathology of the lesion (i.e., multiple cavernous blood filled cavities with remodeling of the host bone) [8].
The key information to be sought by cross sectional imaging besides anatomical localizing and locoregional invasion of the lesion is to determine any coexisting bone pathology and thus exclude any primary neoplastic lesion associated with secondary ABC. CT excels over MRI with regard to assessing areas of complex bone anatomy in sinonasal location whereas intra lesional morphology like presence of fluid fluid levels and content of the locules with varying byproducts of haemoglobin are more evident on MRI owing to its superior soft tissue resolution capability [8,9]. POST contrast enhancement of the peripheral rim and internal septae are better appreciated on MRI however again cortical breaches with destruction of the sinonasal bony wall are better picked up on CT scan [9–11].
Digital Substraction Angiography has both diagnostic and therapeutic role by depicting peripheral hypervascularity, any major vascular supply as well as important for pre surgical workup/embolization [9].
A wide range of pathologies may be considered as a for a expansile multiloculated lesion of sinonasal region with fluid fluid levels including non ossifying fibroma, chondromyxoid fibroma, fibrous dysplasia, giant cell tumour, telengiectatic Osteosarcoma and many of these entities may actually be associated with secondary formation of ABC, hence excluding a primary bony tumour is of prime importance [9,10].
There is a high recurrence rate reported after surgery (upto 20%), hence close radiological and endoscopic follow up is required [8,9].
A wide array of treatment options are considered from Bone grafting, intratumoural sclerotherapy, cryotherapy with surgery, calcitonin administration have all been used but radical excision remains the treatment of choice [9].
Sinonasal Cavernous Haemangioma
Haemangiomas, a commonly seen pathological entity in the head and neck region, however are exceptionally rare and unusual to occur in Sinonasal cavity. They can arise from osseous, mucosal or submucosal tissues of sinonasal region [12].
Cavernous haemangiomas arise from lateral nasal wall or medial wall of maxillary sinus unlike capillary haemangiomas which originate from nasal septum or vestibule [12].
Histologically cavernous haemangiomas are described as large dilated vessels, arranged in a lobular or diffuse pattern, and lined by flattened endothelium [13].
Clinically the locoregional infiltration of the lesion with destruction of bones may pose a quite aggressive picture on imaging. The appearance of substantial bone erosion with nonspecific imaging features may be misleading for the radiologist or primary physician to presume a diagnosis of a malignant tumour. Malignant transformation however has never been reported in literature [13,14].
Clinical features may be quite variable ranging from epistaxis, nasal obstruction, bulging of the eyes or central facial deformity like in our patient.
The features on computerized tomography is very nonspecific with heterogeneously enhancing soft tissue masses with benign appearing bone thinning/remodelling or erosions caused by pressure effect though aggressive destruction of bones have also been reported in literature. Phleboliths, a characteristic of cavernous haemangioma, seen elsewhere are not seen to be reported with haemangioma in the sinonasal region, hence diagnosis is difficult by CT [12,13].
The only consistent radiological sign associated with haemangioma seen on Magnetic resonance imaging is a bright signal on T2- weighted/long TE images [12]. We observed a progressive centripetal fill in enhancement on dynamic MRI contrast study, a feature classical of haemangioma, but not reported in previous case reports of cavernous haemangioma in sinonasal region.
Angiography serves dual purpose of diagnostic and a therapeutic examination, revealing dilated feeding arteries and draining veins, vascularity of the lesion as well as enabling super selective embolization as apre operative work up. Since in our case Contrast CT scan images were highly indicative of haemangioma and no major arterial feeders were identified on CT as well as in Doppler so the patient was directly operated without any pre operative emboliztion. However, angiographic features may be highly valuable as a diagnostic modality as well because typical radiological signs of focal pooling/stagnation of contrast agent, and persistence of the blush on late films which may be a indicator for a vascular entity may be evident only by angiography and hence is always warranted in cases of suspicion [12,13].
Along with polypoid masses, inverted papillomas, mucoceles, neuromas haemangiomas should also be considered as an important entity in the diagnostic work-up of sinonasal masses in the setting of chronic nasal obstruction and repeated epistaxis [13]. Primary treatment of cavernous haemangiomas is surgical with radiation therapy being reserved for inaccessible lesions [15].
Hence haemangioma should be considered with a high index of suspicion in a long standing enhancing sinonasal mass in a young adult with repeated episodes of epistaxis and malignancy should not be presumed as the only diagnosis simply because of associated bone destruction visualized on imaging studies.
Sinonasal Schwannoma
Schwannomas are benign tumours originating from Schwann cells of myelinated nerves. Schwannomas of the sinonasal tract are very rare, comprising less than 4% of the schwannomas of the head and neck [16,17]. In sinonasal region they usually arise from the trigeminal and ophthalmic branches of trigeminal nerve and infrequently from autonomic nerves supplying this region. The site in sinonasal region in decreasing order of origin is nasal septum, ethmoid sinus, maxillary sinus, sphenoid and frontal sinus [17].
Clinical presentation of sinonasal schwannomas is similar to other benign nasal masses with nasal obstruction being the most common symptom followed by epistaxis, anosmia and rhinorrea [16,17]. On nasal endoscopy usually the lesion appears as a smooth polypoid mass with occasional areas of superficial ulceration [16,17]. Although Radiological features are nonspecific, some preoperative diagnostic clues can be obtained from careful observation besides limiting a wide range of differential diagnoses like polyp, papilloma, esthesio neuroblastomas and other infective causes [17,18].
On CT, Schwannomas usually show mild post contrast enhancement and few nonenhancing cystic areas with appreciable bone remodeling and occasional dehiscence of cortical margins in long standing cases. Erosion of sinonasal osseous boundaries with intracranial and intraorbital extensions has been reported though these features do not correlate with malignant potential [18]. The lesions usually show intermediate/hypointense signal on T1W, bright on T2W image (unlike sinonasal polyposis and inspissated secretions which give T2 intermediate signal) with intermediate signal intensity septaes inside which show post contrast enhancement after gadolinium study [18]. MR findings actually indicate the underlying pathological details of the lesion. Lesions with more of Antoni A component (highly cellular) gives intermediate signal on both T1 and T2 whereas Antoni B predominant schwannomas exhibit a more cystic appearance and T2 hyperintense signal due to the presence of intercellular loose myxoid stroma [19].
The tumour cells are mainly composed of elongated spindle cells arranged in fascicles without encapsulation and stain positive for S 100 [20]. The risk of malignant transformation though very low has been observed in patients affected by Von Recklinghausen’s disease [19,20]. Surgical excision (by endoscopic approach) is the treatment of choice. Local recurrences are rare and were and probably related to incomplete resection [21].
Sinonasal osteosarcoma: The incidence of Osteosarcoma involving unusual sites including head and neck is reported to be 8%. Sinonasal Osteosarcoma is a rare entity with a relative incidence 6.5% [22,23]. This malignant tumour is difficult to manage owing to rapid local as well as distant spread, however with the introduction of neo adjuvant chemotherapy five years survival rate has been increased upto 60% [22,23]. Differentiation between Osteosarcoma and chondrosarcoma is crucial as the management of both entities is different [24]. Osteosarcoma is a malignant nonepithleial tumour arising from osteoblasts can mimick chondroblastoma on imaging as well as on histopathology. Osteosarcomas in sinonasal region and those with a predominant chondroblastic component and absence of mature osteoid are particularly difficult to differentiate from chondrosarcoma s even on histopathology [24].
Hence a meticulous and active search for woven new bone should be done on imaging by the radiologist [23,24]. Immunohistochemistry should be used as ancillary diagnostic armamentarium. On Immunohistochemistry lack of positive staining for alpha-1, S-100 & Vimentin with raised alkaline phosphatase can be used as supportive evidence to establish the diagnosis of Osteosarcoma when imaging or HPE are confusing [24,25]. In CT chondrosarcomas typically has a matrix with scattered small rings forming calcifications while areas of abnormal ossification and woven bone formation is the hallmark feature of osteosarcomas. MRI typically demonstrates high-intensity T2 signal for the chondroid matrix [25].
Surgical options available are endoscopic sinus surgery, lateral rhinotomy, medial maxillectomy, maxillectomy, craniofacial resection accomapanied by pre and postoperative chemotherapy [26].
Conclusion
Understanding and recognizing the spectrum of appearances of these rare tumours will allow improved patient assessment and are vital for optimal clinical management including diagnosis, biopsy, staging, treatment, and prognosis. The hallmark or pathognomonic signs of a particular tumour (e.g.-abnormal osteoid in Osteosarcoma, peripheral enhancement with progressive centripetal filling in haemangioma) should be actively sought for as the radiological features of the tumour may be similar as elsewhere in the body and these may be the sole diagnostic clues. CT and MRI serve complimentary roles in identifying the morphological details and locoregional staging of these unusual tumours.
[1]. Yildirim D, Saglam O, Gurpinar B, Ilica T, Nasal Cavity Masses: Clinico-Radiologic Collaborations, Differential Diagnosis by Special CluesOpen Journal of Medical Imaging 2012 2:10-18. [Google Scholar]
[2]. Lathi A, Syed MMA, Kalakoti P, Qutub D, Kishve SP, Clinico-pathological profile of sinonasal masses:a study from a tertiary care hospital of IndiaActa Otorhinolaryngol Ital 2011 31(6):372-77. [Google Scholar]
[3]. Citardi MJ, Janjua T, Abrahams JJ, Sasaki CT, Orbitoethmoid aneurysmal bone cystOtolaryngol Head Neck Surg 1996 114:466-70. [Google Scholar]
[4]. Chateil JF, Dousset V, Meyer P, Cranial aneurysmal bone cysts presenting with raised intracranial pressure: report of two casesSpringer Neuroradiology 1997 39:490-94. [Google Scholar]
[5]. Jaffe HL, Lichtenstein L, Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance, and the pathogenesisArch Surg 1942 44:1004-25. [Google Scholar]
[6]. Buraczewski J, Dabska M, Pathogenesis of aneurysmal bone cyst. Relationship between the aneurysmal bone cyst and fibrous dysplasia of boneCancer 1971 28(3):597-604. [Google Scholar]
[7]. Suzuki F, Fukuda S, Yagi K, Chida E, Inuyama Y, A rare aneurysmal bone cyst of the maxillary sinus: a case reportAuris Nasus Larynx 2001 28:131-17. [Google Scholar]
[8]. Kransdorf MJ, Sweet DE, Aneurysmal bone cyst: concept, controversy, clinical presentation, and imagingAm J Roentgenol 1995 164:573-80. [Google Scholar]
[9]. Maroldi R, Berlucchi M, Farina D, Tomenzoli D, Borghesi A, Pianta L, Benign Neoplasms and Tumour-Like Lesions, Aneurysmal bone cyst. In:Roberto Maroldi, W. Draf, Piero NicolaiImaging in Treatment Planning for Sinonasal Diseases 2004 1st editionSpringer:114-16. [Google Scholar]
[10]. Dubey RB, Tara NP, Desai SM, Giant cell tumour of sinonasal cavity- an uncommon location for a common bone tumourIJRI 2003 13:13-14. [Google Scholar]
[11]. Kendi AK, Kara SA, Altinok D, Keskil S, Sinonasal Ossifying Fibroma with Fluid-Fluid Levels on MR ImagesAJNR 2003 24:1639-41. [Google Scholar]
[12]. Vargas MC, Castillo M, Sinonasal cavernous haemangioma: a case reportDentomaxillofacial Radiology 2012 41:340-41. [Google Scholar]
[13]. Dhanapala N, Ravishankar C, Ramya B, Bhat S, Viswanatha B, A Rare Case of Sinonasal Cavernous HaemangiomaResearch in Otolaryngology 2013 2(1):12-14. [Google Scholar]
[14]. Kim HJ, Kim JH, Kim JH, Hwang EG, Bone Erosion Caused by Sinonasal Cavernous Haemangioma: CT Findings in Two PatientsAJNR 1995 16:1176-78. [Google Scholar]
[15]. Sciarreta V, Pasquini E, Frank G, Endoscopic treatment of benign tumours of the nose and paranasal sinuses: a report of 33 casesAm J Rhinol 2006 20:64-71. [Google Scholar]
[16]. Hong SM, Shin JM, Park IH, Lee SH, Kim YD, Lee HM, Clinical Experience of Sinonasal SchwannomasJ Rhinology 2013 20(1):26-30. [Google Scholar]
[17]. Cheng YUC, Sun POL, Chen HJ, Wang HK, Lee YUC, Benign Schwannoma in the Sphenoid Sinus: two cases reportsChin J Radiol 2010 35:179-83. [Google Scholar]
[18]. Yu E, Mikulis D, Nag S, CT and MR Imaging Findings in Sinonasal SchwannomaAJNR 2006 27:929-30. [Google Scholar]
[19]. Maroldi R, Berlucchi M, Farina D, Tomenzoli D, Borghesi A, Pianta L, Benign Neoplasms and Tumour-Like Lesions. Schwannoma. In: Roberto Maroldi, W. Draf, Piero NicolaiImaging in Treatment Planning for Sinonasal Diseases 2004 1st editionSpringer:149-150. [Google Scholar]
[20]. Buob D, Wacrenier A, Chevalier D, Aubert S, Schwannoma of the Sinonasal Tract A Clinicopathologic and Immunohistochemical Study of 5 CasesArch Pathol Lab Med 2003 127:1196-99. [Google Scholar]
[21]. Lee JT, Thompson LDR, Garg R, Keschner DB, Endoscopic Management of Recurrent Anterior Skull Base SchwannomaIJOHNS 2013 2:52-56. [Google Scholar]
[22]. Heller RM, Dominquez R, Ertel IJ, Winfield AC, Kirchner SG, A review of the unusual appearance or atypical location of osteogenic sarcoma in childhoodRadioGraphics 1984 4(3):507-14. [Google Scholar]
[23]. Mark RJ, Sercarz JA, Tran L, Dodd LG, The osteogenic sarcoma of the head and neck: The UCLA experienceArch Otolaryngol Head Neck Surg 1991 117(7):761-66. [Google Scholar]
[24]. Shahid H, Baharudin A, Halim AS, Biswal BM, Jihan WS, An Extensive Sinonasal Osteosarcoma Mimicking ChondrosarcomaMed J Malaysia 2007 62(2):171-72. [Google Scholar]
[25]. Gopalakrishnan SN, Elango KM, Saravanan S, A case of sinonasal chondrosarcoma–case reportOtolaryngology Online Journal 2014 4(4):1-8. [Google Scholar]
[26]. Watkinson JC, Gaze MN, Wilson JA, Rare tumoursIn: Stell Maran’s Head and Neck Surgery 2000 25Butterworth-Heinemann:504 [Google Scholar]