Thyroid nodules are common, varieties of benign and malignant lesions of thyroid present as nodules. At our tertiary care centre, we do not have provision for IHC and other higher investigation. Also, the majorities of patients are from lower socio economic class and can’t afford higher investigation in private laboratories. As a result of which our study is based on cytological diagnosis of thyroid lesions according to Bethesda system and it’s histopathological correlation. The Bethesda system of thyroid lesion on FNAC reporting, aims at standardization of reports. It bridges the communication gap between clinicians and pathologists and thus helps the surgeons to take appropriate therapeutic interventions [1].
To elucidate the diagnostic utility of the Bethesda system in reporting thyroid FNAs and to assess the effectiveness of FNAC in the evaluation of thyroid nodules by comparing the results with histopathological evaluation.
Materials and Methods
The present study was carried out in our institute during the July 2012 to September 2014 (Prospective study). The study comprised of 100 patients who presented with the history of swelling of thyroid which were referred from the Departments of Surgery, Medicine & ENT. Patients were explained about the procedure and written consent was taken.
Inclusion criteria: Patient of both gender, age 10 to 80 years, presenting with thyroid swelling in any lobe of thyroid selected by clinical palpation (multinodular, solitary nodules, diffuse goiter, etc) and patients with recurrent thyroid swellings after a previous thyroid surgery.
FNAc was performed in all cases of midline neck swelling by cytopathologist. Proper consent was taken. The patient asked to lie in supine position with their neck stretched up. A 23-24 gauge needle is used to perform the fine needle aspiration. The cytological diagnosis was given according to the Bethesda system. The cytological diagnosis was correlated with clinical presentation, TFT and histopathology, whenever possible [2].
Results
The present study consisted of 100 cases of various thyroid lesions admitted and treated at the tertiary care centre during July 2012 to September 2014. Criteria taken for adequacy of FNA material were:
a) 6 clusters of thyroid follicular cells in at least two slides prepared from separate aspirates.
b) 5 – 6 groups of cells with more than 10 cells/group.
c) Abundant colloid is equally important for a benign diagnosis in solitary nodule.
• FNAC Analysis (According to Bethesda system): The maximum incidence of thyroid lesions, were between the ages of 31-40 years, i.e. 35 cases (35%). In present study 6 cases were Nondiagnostic (category I), because 2 cases have only cystic fluid and 4 cases have extensive blood which obscuring the evaluation of the follicular cells. (Shown in [Table/Fig-1]).
Age and sex distribution of thyroid lesion (Based on FNAC according to Bethesda System)
| Age(in years) | Sex (M/F) | ND/US (Category I) | Benign (Category II) | AUS (Category III) | FN/SFN (Category IV) | SFNHCT /FNHCT (Category IV) | SFM (Category V) | Malig-nant (Category VI) |
|---|
| 0-10 | 00 | 00 | - | - | - | - | - | - | - |
| 11-20 | 00 | 05 | 01 | 04 | - | - | - | - | - |
| 21-30 | 01 | 21 | 01 | 19 | 01 | - | - | - | 01 |
| 31-40 | 03 | 32 | 01 | 27 | 02 | 02 | 01 | 01 | 01 |
| 41-50 | 02 | 19 | 02 | 17 | - | 01 | - | 01 | - |
| 51-60 | 02 | 07 | 01 | 06 | - | 01 | - | 01 | - |
| 61-70 | 00 | 06 | - | 04 | 01 | - | - | - | 01 |
| 71-80 | 00 | 02 | - | 01 | - | - | - | - | 01 |
| Total | 08 | 92 | 06 | 78 | 04 | 04 | 01 | 03 | 04 |
• Histopathological diagnosis of thyroid lesion: In the present study of 100 cases, 60 patients underwent surgery and the histopathological diagnosis of the cases are given below-
Patient who underwent surgery are more common between age group 21-50 years. Showing sex distribution - all Neoplastic lesion were in female.
Distribution of various thyroid lesion on histopathology shown in [Table/Fig-2].
Age and sex distribution of various thyroid lesion (Based on histology)
| Age(in years) | Sex (M/F) | Colloid cyst | Colloid goiter | Hyperplastic thyroid lesion | Subacute graulomatous thyroiditis | Lympho.(Hashimoto’s) thyroiditis | FA | FC | HCA | PC | MC |
|---|
| 0-10 | 00 | 00 | - | - | - | - | - | | | | | |
| 11-20 | 00 | 02 | 01 | 01 | - | - | - | - | - | - | - | - |
| 21-30 | 00 | 10 | - | 04 | 02 | - | 02 | - | - | - | 02 | - |
| 31-40 | 02 | 22 | 01 | 10 | 05 | 01 | 01 | 02 | 01 | 01 | 01 | 01 |
| 41-50 | 01 | 10 | 01 | 04 | 04 | - | - | 02 | - | - | - | - |
| 51-60 | 01 | 06 | 01 | 02 | 01 | 01 | - | 01 | - | - | 01 | - |
| 61-70 | 00 | 04 | - | 01 | - | - | 01 | - | 01 | - | 01 | - |
| 71-80 | 00 | 02 | - | - | 01 | - | - | - | - | - | 01 | - |
| Total | 04 | 56 | 04 | 22 | 13 | 02 | 04 | 05 | 02 | 01 | 06 | 01 |
• Cytohistopathological correlation of thyroid lesion: Cyto-Histopathological correlation of thyroid lesion of present study shown in [Table/Fig-3].
Cyto-Histopathological correlation of thyroid lesion of present study.
| Cytolopathology | Histopathological diagnosis | Total |
|---|
| Benign | Malignant | |
|---|
| I | Non-diagnostic or Unsatisfactory | 04 | 01 | 05 |
| II | Benign | 39 | - | 39 |
| III | Atypia of Undetermined Significance | 03 | 01 | 04 |
| IV | Follicular Neoplasm or Suspicious for a Follicular Neoplasm | 03 | 01 | 04 |
| Follicular Neoplasm, Hurthle cell Type / Suspicious for a Follicular Neoplasm, Hurthle Cell Type | 01 | - | 01 |
| V | Suspicious for Malignancy | 01 | 02 | 03 |
| VI | Malignant | | 04 | 04 |
| Total | | 51 | 09 | 60 |
There were 05 cases of ND/US on FNAC, out of this 1 case was diagnosed as papillary carcinoma of thyroid on histology. There were 04 cases of AUS diagnosed on FNAC. Out of them 01 diagnosed as Colloid goiter, 01 diagnosed as Hyperplastic thyroid lesion, 01 diagnosed as Follicular adenoma and 01 diagnosed as Follicular carcinoma. Out of 4 cases of Follicular neoplasm or suspicious of follicular neoplasm, 3 were diagnosed as Follicular adenoma and 1 was diagnosed as Follicular carcinoma on histology. 01 case of Follicular Neoplasm, Hurthle cell Type/ Suspicious for a Follicular Neoplasm, Hurthle Cell Type was diagnosed as Hurthle cell adenoma on histology. Out of 03 case of Suspicious for Malignancy, 01 diagnosed as Medullary carcinoma of thyroid, 01 diagnosed as Follicular adenoma and 1 was diagnosed as Follicular carcinoma on histology.
Out of 04 cases of Malignancy (Papillary carcinoma of thyroid) was diagnosed as Papillary carcinoma of thyroid on histology. So the accuracy was 100%.
• Rate of Malignancy on Surgical Resection for FNA Diagnostic Categories using TBSRTC: Rate of Malignancy shown in [Table/Fig-4].
Rate of Malignancy on Surgical Resection for FNA Diagnostic Categories using TBSRTC
| Diagnostic Category | Malignancy RateNo. of Cases(%) present study |
|---|
| ND/UNS (n = 5) | 1 (20%) |
| BN (n = 39) | 0 (0%) |
| AUS (n = 4) | 1(25%) |
| SFN (n =5) | 1(20%) |
| SM (n = 3) | 2(66%) |
| MGT (n = 4) | 4(100%) |
• Statistical Data of the present study as Shown in [Table/Fig-5]). Various histopathological and gross findings have been depicted in the following [Table/Fig-6,7,8,9,10,11 and 12].
| SENSITIVITY | 88.89% |
| SPECIFICITY | 84.31% |
| POSITIVE PREDICTIVE VALUE | 50.0% |
| NEGATIVE PREDICTIVE VALUE | 97.7% |
| PERCENTAGE OF FALSE POSITIVE | 15.6% |
| PERCENTAGE OF FALSE NEGATIVE | 11.1% |
Cytology-Colloid globi & follicular cells in Benign follicular nodules consistent with Colloid Goiter (H&Ex40) (Category I)
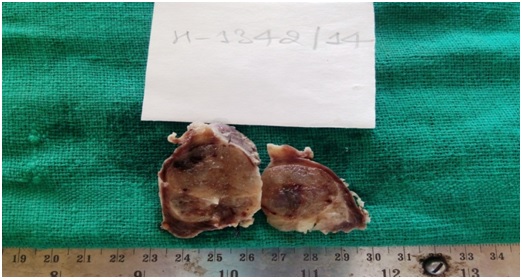
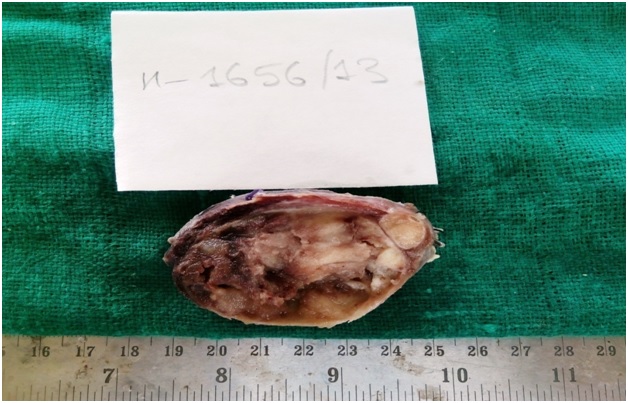
Photograph of Colloid goiter – cut section showing colloid with intact capsule
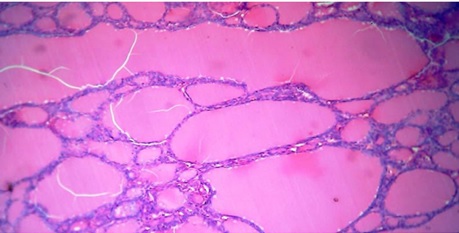
Colloid goitre: Follicles of variable sizes lined by flattened epithelium and containing abundant colloid (H&E; x 100)
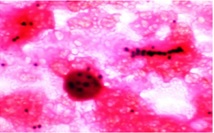
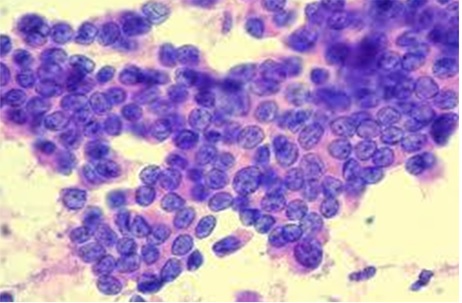
Cytology: Papillary Carcinoma. Cellular smear showing flat, monolayered sheet of cells with enlarged nuclei & intranuclear inclusions (H&E; 400X)(Category VI)
Photograph of Papillary Carcinoma. Showing cystic cavity with papillary growth.
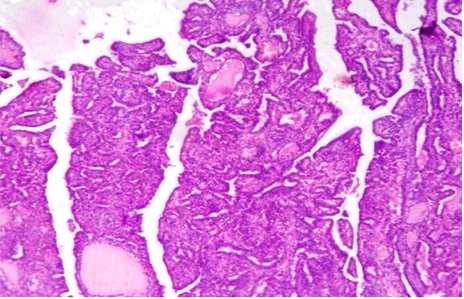
HP- Papillary Carcinoma. Classic Papillary pattern. Papillae have a fibrovascular core and ground glass nuclei. (H&E; 100X)
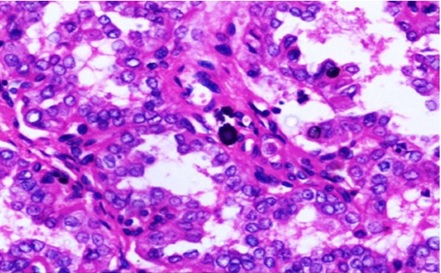
HP- Papillary carcinoma showing ground glass nuclei and nuclear grooving. ocassional psammoma bodies seen. (H&E, 400X).
Discussion
The present study consisted of 100 cases of various thyroid lesions. Out of 100 FNACs, 60 case were biopsied subsequently and subjected for histopathological study and correlate with other studies [Table/Fig-13,14,15,16 and 17].
Age range in different studies in comparison with present study
| Studies | Age range(y) | Mean age in (y) |
|---|
| Handa et al., [3] (2008) | 5-80 yrs | 37.69 yrs |
| Gupta et al., [4] (2010) | 22 – 58yrs | 38.72 yrs |
| Muratli et al., [5] (2014) | 17-89 yrs | 51.24 yrs |
| Present study | 10 -80 yrs | 38.50 yrs |
Sex distribution and male to female ratio of various studies with the present study
| Studies | Total Cases | Male | Female | Male: Female |
|---|
| Silverman JF et al., [2] (1986) | 295 | 25 | 270 | 1:10.8 |
| Handa et al., [3](2008) | 434 | 59 | 375 | 1:6.35 |
| Gupta et al., [4] (2010) | 75 | 6 | 69 | 1:11.5 |
| Muratli et al., [5] (2014) | 1333 | 226 | 1107 | 1:4.89 |
| Present study | 100 | 08 | 92 | 1:11.5 |
Distribution of cases in Bethesda categories in different studies
| Diagnostic categories | Number of cases in each categories |
|---|
| Yassa et al., [6] (2007 | Nayar and Ivanovic [7] (2009) | Jo et al., [8] (2010) | Mufti et al., [9] (2012) | Mondal et al., [10] (2013) | Present study |
|---|
| Non-diagnostic or Unsatisfactory | 181(7%) | 260(5%) | 573(18.6%) | 29 (11.6%) | 12 (1.18%) | 06 (6%) |
| Benign | 1707(66%) | 3324(64%) | 1817(59%) | 194(77.6%) | 893(87.5%) | 78(78%) |
| Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance | 104(04%) | 935(18%) | 105(3.4%) | 02(.8%) | 10(0.98%) | 04(04%) |
| Follicular Neoplasm or Suspicious for a Follicular Neoplasm | 233(09%) | 311(6%) | 299(9.7%) | 10(4%) | 36(3.58%) | 04(04%) |
| Follicular Neoplasm, Hurthle cell Type / Suspicious for a Follicular Neoplasm, Hurthle Cell Type | - | | | | 07(0.69%) | 01(01%) |
| Suspicious for Malignancy | 233(9%) | 104(2%) | 71(2.3%) | 06(2.4%) | 14(1.37%) | 14(1.37%) |
| Malignant | 129(5%) | 260(5%) | 215(7%) | 09(3.6%) | 48(4.7%) | 04(04%) |
| Total | 2587 | 5194 | 3080 | 250 | 1020 | 100 |
Comparison of the percentages of follow-up malignancy of present study with other studies
| Diagnostic Category | Mufti et al., [9](n=84) | Jo et al., [8](n=882) | Yang et al., [11](n=1052) | Yassa et al., [6] | Mondal et al., [10] (n=323) | Present study (n=60) |
|---|
| ND/UNS | 20% | 8.9% | 10.7% | 10% | 0% | 20% |
| BN | 3.1% | 1.1% | 0.7% | 0.3% | 4.5% | 0% |
| AUS | 50% | 17% | 19.2% | 24% | 20% | 25% |
| SFN | 20% | 25.4% | 32.2% | 28% | 30.6% | 20% |
| SM | 80% | 70% | 64.8% | 60% | 75% | 66% |
| MGT | 100% | 98.1% | 98.4% | 97% | 97.8% | 100% |
Comparison of diagnostic value for malignant lesion
| Studies | Year | Sensitivity % | Specificity % |
|---|
| Yang et al., [11] | 2007 | 94 | 98.5 |
| Gupta et al., [4] | 2010 | 80 | 86.6 |
| Bukhari et al., [12] | 2012 | 100 | 82.5 |
| Mondal et al., [10] | 2013 | 86.6 | 87 |
| Muratli et al., [5] | 2014 | 87.1 | 64.6 |
| Mehra et al., [13] | 2015 | 76.92 | 88.46 |
| Present Study | 2014 | 88.89 | 84.31 |
• Shows Age Range in Different Studies In Comparison With Present Study:.
[Table/Fig-13] shows the good correlation of other studies with present study except one study by Muratli et al., In which they observed Mean age 51.24 years.
Muratli et al., showed higher mean because of large sample with varied age groups.
The mean age of present study was 38.50 years.
• Showing Sex distribution and Male to Female ratio of various studies with the present study: There was the predominance of female patients in all studies.
[Table/Fig-14] shows the good correlation of Gupta et al.,, Silverman JF et al., studies with present study. Muratli et al.,, Handa et al., shows some variation because of their large sample size.
In present study Male to Female ratio was 1:11.5.
• Distribution of cases in Bethesda categories in different studies: [Table/Fig-15] shows that there was good correlation of Non-diagnostic or Unsatisfactory categories of present study with Yassa et al., and Nayar and Ivanovic. Except others Jo et al., and Mufti et al., show higher percentage of Nondiagnostic categories. The reason for the lower percentage in the non-diagnostic is that, in our tertiary care center, usually an ultrasound-guided FNAC is performed for small nodules or nodules that appear heterogeneous on palpation and cytopathologist himself performs the procedure of FNAC, a better quality and adequate aspirate can be ensured. For Mondal et al., the reason was same but they used large sample size.
[Table/Fig-15] shows that there was good correlation of Benign categories of present study with Mondal et al., and Mufti et al.,. Others studies Jo et al.,, Yassa et al., and Nayar and Ivanovic show low percentage of Benign categories. The reason for the number of cases in the benign category being higher is that patients usually come directly to our tertiary care centre with out any reference. Hence our study group is a representative of general population. As the benign cases are seen more in general population, thes same is the cases in our study.
It could be seen that there was good correlation of Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance of present study with Yassa et al.,, Jo et al., Nayar and Ivanovic show higher result. The less number of cases diagnosed as AUS in the present study could be explained by the strict adherence to diagnostic criteria and the cytopathologist’s efforts in our practice setting to avoid ambiguity and keep the use of AUS to a minimum. Mondal et al., and Mufti et al., show much lower percentage because they strict adherence to diagnostic criteria and they also have large sample size. From [Table/Fig-15], it can be noted that there was good correlation of Suspicious for a Follicular Neoplasm including Suspicious for a Follicular Neoplasm, Hurthle Cell Type of present study with Nayar and Ivanovic, Mufti et al., and Mondal et al., Yassa et al., and Jo et al., shows some higher percentage because of their large sample size and may be geographical distributation.
[Table/Fig-15] also shows that there was good correlation of Suspicious for Malignancy of present study with Nayar and Ivanovic, Jo et al., Mufti et al., and Mondal et al.
• Comparison of the percentages of follow-up malignancy of present study with other studies other studies: The ND/UNS category in our study was comparable to Mufti et al., Other studies show quite comparable result except Mondal et al., Others studies have large sample size so the denominator is high so the percentage was less.
ND/UNS cytologic findings may also result from poor fixation, preparation, or staining or from excessive blood, necrotic material, or debris obscuring cellular details, misinterpretations. It is, however, important to keep in mind that ND/UNS specimen does not mean negative specimen. The Benign nodule category in our study yielded a malignancy rate of 0% which was quite comparable with other studies.
The AUS category in our study yielded a malignancy rate of 25% which was quite comparable with other studies except Mufti et al., because less number of cases diagnosed as AUS in the that study.
The SFN category in our study yielded a malignancy rate of 20% which was quite comparable with other studies.
The SFM category in our study yielded a malignancy rate of 66% which was quite comparable with other studies.
The Malignant category in our study yielded a malignancy rate of 100% which was quite comparable with other studies.
• Comparison of diagnostic value for malignant lesion: The sensitivity of the present study is 88.89%. In other studies it was 78% to 100% percentage of sensitivity were observed, which is quite comparable. The specificity of the present study is 84.31 %. In other studies it was 64% to 98% percentage of sensitivity were observed, which is quite comparable.
Conclusion
This study is prospective study in which thyroid aspiration smear is reported by TBSRTC using the Bethesda system & also correlated by histopathological examination. TBSRTC bridges the gap between clinician & cytopathologist. It also helps in determining the risk of malignancy in each category of TBSRTC. It is a universal terminology & its use should be encouraged.