Osteoarthritis (OA) is the most common degenerative joint disorder and a major contributor to the functional impairment and dependency in older adults throughout the world [1–3]. About 40% of population aged over 65 years are reported to have symptomatic OA of the knee [4,5]. Early detection and intervention is of paramount importance in decreasing the morbidity and disability for a better independent living. Radiography is the first investigation of choice for OA patients presenting with knee pain. Community based studies have shown that 40% to 80% of subjects with radiographic knee OA are symptomatic [6] and severe radiographic knee OA is associated with greater pain. However there is a high degree of discordance between clinical and radiographic findings and the radiological classification of OA is imprecise in the early stages [7–12]. The reason for discordance between pain and radiography can be explained by the multifactorial origin of pain [8,9,13]. Direct assessment of the articular cartilage by arthroscopy [12] allows a more detailed description to be made regarding depth and extent of the lesions, subtle changes such as cartilage softening, fibrillation and tangential flaking. Though arthroscopy aids in accurate diagnosis of OA knee and facilitates joint debridement to be carried out simultaneously [12,14], it cannot be routinely carried out in all the patients. The existing literature comparing clinical, radiographic and arthroscopic grading was discordant. In view of the conflicting reports in the literature the present study was undertaken to study the correlation among radiographic, arthroscopic and pain findings in knee OA patients to facilitate early and precise diagnosis so that appropriate and timely treatment modalities can be instituted [2,7,8].
Materials and Methods
A cross-sectional analysis of 28 cases (14 males and 14 females) of primary OA knee (seven each from grade 1 to 4), screened and selected from the out-patient department of Orthopaedics was carried out. Patients who are unfit for surgery from anaesthesia stand point and cases with secondary causes of OA, other arthropathies, metabolic bone disease, neoplasms were excluded from the study. Institutional review board has accepted the study. The patients were enrolled by their will after a written informed consent was taken.
Detailed history including the demographics were recorded and thorough physical examination of the affected joints was done. Weight bearing antero-posterior (AP) - and lateral knee radiographs were recorded for both the knees for the assessment of radiological changes [Table/Fig-1].
Original photos- Antero-posterior radiographs representing each grade of osteoarthritis in ascending order
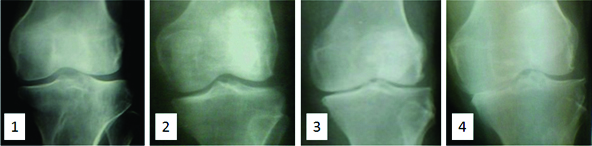
Kellgren Lawrence (K-L) staging of the radiographs was used after testing the interobserver reliability [15]. In view of its validity and reliability this method was accepted by the World Health Organisation (WHO) and was widely used for studies on OA of knee [8].
Apley’s pain score [16] equated to Visual Analogue Score was used for the assessment of pain associated with OA.
Under spinal anaesthesia and tourniquet control diagnostic arthroscopy, lavage and debridement were carried out as per the requirements of the case [Table/Fig-2].
Original photos-Depiction of arthroscopic findings in the ascending order of severity of articular cartilage damage
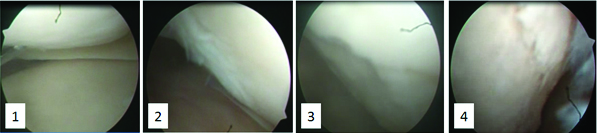
Outer bridge classification system [17] was used to assess the articular damage.
Statistical Analysis
All statistical analyses were performed using Graph pad prism and Excel for Windows. Descriptive statistics were used to describe demographic characteristics. Spearman’s rank Correlation Coefficients (Rho estimate/r) were calculated to determine the relationships between clinical radiographic and arthroscopic grades in patients with knee OA.
Results
A total of 28 OA patients, 14 males and 14 females were evaluated with seven patients each in radiographic grades 1, 2, 3 & 4.
The mean age and BMI of the study population as given in [Table/Fig-3] shows that the higher age group did manifest greater degree of articular damage radiologically. It’s also seen that grade 3 and grade 4 damage was associated with higher BMI.
Demographic characteristics of the study population
| Radiological grade(n) | Age in years(Mean ± S.D) | BMI in Kg/m2(Mean ± S.D) |
|---|
| 1 (7) | 39.85 ± 11.42 | 22.54 ± 4.81 |
| 2 (7) | 46.85 ± 12.83 | 24.49 ± 3.33 |
| 3 (7) | 49.57 ± 9.84 | 26 ± 4.56 |
| 4 (7) | 56 ± 6.48 | 25.22 ± 4.71 |
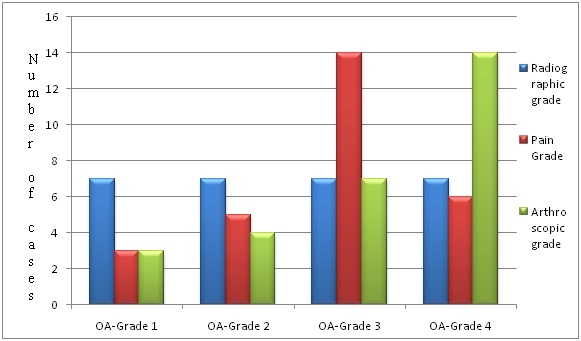
Among 28 patients, 10.71% had arthroscopic grade 1 findings, 14.28% had arthroscopic grade 2 findings, 25% had arthroscopic grade 3 findings and 50% had arthroscopic grade 4 findings as shown in [Table/Fig-4].
Bar diagram depicting the number of patients in each grade
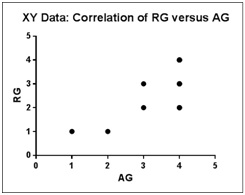
Overall correlation between radiographic, arthroscopic and pain grades was done using Spearman Rank correlation coefficient. Across all the four radiographic and arthroscopic grades in 28 OA patients, there was a good correlation between radiographic and arthroscopic grades with Spearman’s coefficient of rank correlation (rho or ‘r’) = 0.8077. Further, this association was statistically significant at p < 0.0001 (two tailed) & 95% Confidence Interval (CI) for rho/r was at 0.6149 to 0.9094 [Table/Fig-5].
Spearman’s correlation coefficient graph for radiographic and arthroscopic grades (overall)
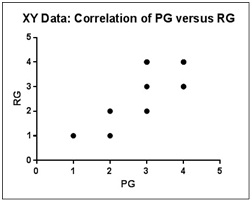
Across all the four radiographic and pain grades in 28 OA patients, there was a good correlation between pain and radiographic grades with r = 0.8212. Further, this association was statistically significant at p< 0.0001 & 95% CI was at 0.6392 to 0.9161 [Table/Fig-6].
Spearman’s correlation coefficient graph for pain and radiographic grades (overall)
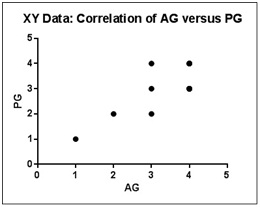
Across all the four arthroscopic and pain grades in 28 OA patients, there was a good correlation between arthroscopic and pain grades with r = 0.7634. Further, this association was statistically significant at p < 0.0001(two tailed) & 95% CI was at 0.5376 to 0.8871 [Table/Fig-7].
Spearman’s correlation coefficient graph for arthroscopic and pain grades (overall)
RG- Radiographic grade, PG-Pain grade, AG-Arthroscopic grade
As the patients under study were divided into four grades by radiological criteria, correlation of specific radiographic grades with arthroscopic and pain grades could not be computed by Spearman or Pearson’s method as the standard deviation was zero.
The following [Table/Fig-8] depicts the individual radiographic, arthroscopic, pain grade comparison and percentage correlation. [Table/Fig-9] depicts the correlation of radiographic grade with Mean±SD of corresponding arthroscopic and pain grading.
Table depicting percentage correlation statistics of RG, AG and PG
| Radiographic grade | Total No. of cases | Arthro-scopic grade | No. of cases | Percentage |
|---|
| 1 | 7 | 1 | 3 | 42.8% | Correlating |
| 2 | 4 | 57.2% | Non correlating |
| 2 | 7 | 3 | 4 | 57.2% | 100% Non correlating |
| 4 | 3 | 42.8% |
| 3 | 7 | 3 | 3 | 42.8% | Correlating |
| 4 | 4 | 57.2% | Non correlating |
| 4 | 7 | 4 | 7 | 100 % Correlating |
| Radiographic grade | Total No. of cases | Pain grade | No. of cases | Percentage |
|---|
| 1 | 7 | 1 | 3 | 42.8% | Correlating |
| 2 | 4 | 57.2% | Non correlating |
| 2 | 7 | 2 | 1 | 14.3% | Correlating |
| 3 | 6 | 85.7% | Non correlating |
| 3 | 7 | 3 | 5 | 71.5% | Correlating |
| 4 | 2 | 28.5% | Non correlating |
| 4 | 7 | 3 | 3 | 42.8% | Correlating |
| 4 | 4 | 57.2% | Non correlating |
| Pain grade | Total No. of cases | Arthro-scopic grade | No. of cases | Percentage |
|---|
| 1 | 3 | 1 | 3 | 100% | Correlating |
| 2 | 5 | 2 | 4 | 80% | Correlating |
| 3 | 1 | 20% | Non correlating |
| 3 | 14 | 3 | 5 | 35.7% | Correlating |
| 4 | 9 | 64.3% | Non correlating |
| 4 | 6 | 4 | 5 | 83.3% | Correlating |
| 3 | 1 | 16.6% | Non correlating |
Table depicting correlation statistics (Mean) of RG, AG and PG
| Radiographic grade (RG) | Mean ± SD of Arthroscopic grade (AG) | Mean ± SD of Pain grade (PG) |
|---|
| 1 | 1.57±0.49 | 1.57±0.49 |
| 2 | 3.42±0.49 | 2.57±0.72 |
| 3 | 3.57±0.49 | 3.28±0.45 |
| 4 | 4±0 | 3.57±0.49 |
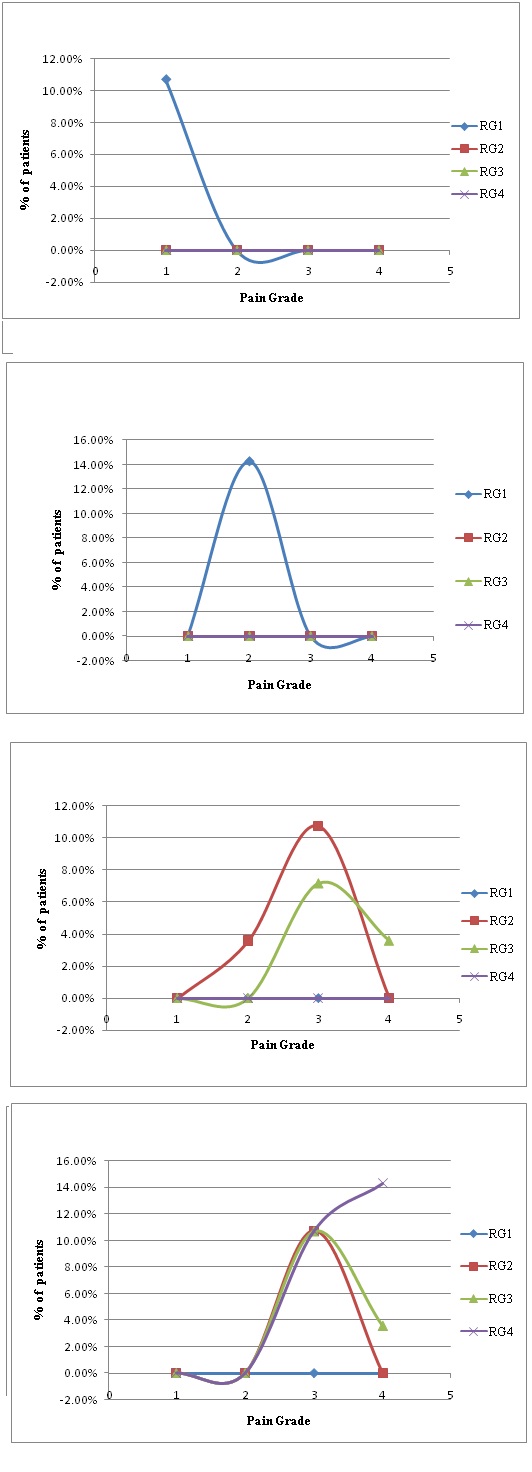
A systematic correlation of the pain expressed by the patient and radiographic observation with corresponding % population of patients expressing arthroscopic grade 1 to 4 were plotted as a scatter plot and shown in [Table/Fig 10a-d].
(a) Arthroscopic Grade 1. (b) Arthroscopic Grade 2. (c) Arthroscopic Grade 3. (d) Arthroscopic Grade 4
Scatter plots for correlation of radiographic, pain grade and percentage of patients with different arthroscopic grades (1to 4)
Discussion
Pain is the most common presentation of osteoarthritis of knee [9]. Pain being a subjective entity accurate measurement of pain is difficult. Visual Analogue Score (VAS) is commonly used to measure the subjective pain with a scale of 1 to 10. As radiographic and arthroscopic scoring/ grading systems have 1 to 4 grades it was felt that VAS should better be extrapolated to Apley’s pain scoring system [16] with 1 to 4 grade scale for ease and convenience of comparison and calculations.
Radiography is the key and primary investigation of choice for the diagnosis and grading of osteoarthritis of knee. Standard weight bearing antero-posterior and lateral view of knee in extension are routinely used. K-L system is the most often used and WHO accepted radiological classification system for the diagnosis of OA of knee [15,18,19].
Arthroscopic findings represent the exact extent and degree of the pathology of OA knee. Outerbridge classification system is used to quantify the same [17,20]. It is difficult and improper to subject all the cases of OA knee to arthroscopic examination just for the detection of the extent of articular damage except in cases of degenerative meniscal tears, persistent pain with or without locking, OA with effusion and loose bodies which require direct examination, lavage and debridement. Hence it is imperative to formulate guidelines for the exact diagnosis and staging of OA knee by clinical examination and conventional radiography keeping in mind the probable arthroscopic findings in a given case.
Kiran Gaonkar et al., [2] studied the overall correlation of K-L grade of OA knee with Outerbridge classification of arthroscopic OA grade in 53 cases and reported r =1.0. Razak et al., [7] reported the overall correlation of radiographic and arthroscopic grades as r=0.32 in 119 cases (number of cases in grade 4 was only eight). Shivananda et al., (180 cases) and Cubukcu D et al., (114 cases) studied the overall correlation of pain and radiographic features in OA knee and reported the (r) as 0.174 and 0.172 with p<0.05 suggesting poor correlation [8,18]. The MARS group [19] recommends the use of IKDC (International Knee Documentation Committee) grading scale of OA knee with Rosenberg radiographs (standing posterio-anterior view of knee in 45° of flexion) to decrease the interobserver variability of diagnosis in comparison with the K-L grading scale read with standard standing A-P knee radiographs and improve the correlation of radiographic grading with arthroscopic findings. It was observed that the difference in (r) for K-L with A-P radiograph (0.30) and IKDC with A-P radiograph (0.32) was 0.02 and the same with Rosenberg view was 0.05. It may be noted that the above conclusions/recommendations were made by clubbing all the grades of OA knee.
There is a paucity of literature pertaining to the systematic comparison/correlation of radiographic, pain and arthroscopic findings in a given grade of OA knee to precisely guide the categorisation of patients for diagnosis and management. Meagre correlation studies were carried out in the past by clubbing all the grades of patients and an overall correlation coefficient was arrived, which may not correctly represent the correlation in individual group of cases. It was obvious from the review of literature that the results seem to differ when unequal number of cases in each grade were clubbed together and compared [2,7,8,18,19]. In our opinion, such a correlation arrived at by clubbing all the grades do not convey any meaningful conclusion on correlation of radiographic, arthroscopic and pain criteria to alleviate imprecise diagnosis. To obviate such fallacy and to bridge this gap equal numbers of cases in each grade were considered for comparison and correlation of various parameters in our study in contrast to all the reported studies in the literature.
Analysis of the preliminary data from our study shows sequential progression of osteoarthritis with age and body mass index i.e. higher age groups with increased body mass index had higher grade of osteoarthritis which was concurrent with the existing literature [1–3] [Table/Fig-3]. From our study, it can be noted that radiographic, arthroscopic and pain grades appear to correlate well when all the grades were clubbed. But the results depicted in [Table/Fig-4] compared with [Table/Fig-5,6 and 7] were contradictory. When the individual radiographic grades were compared with the arthroscopic and pain grades the results were different in contrast to the ones obtained by clubbing all the grades of OA. Though equal number of patients in each radiographic grade were studied there was an apparent increase in the number of patients with higher arthroscopic and pain grades [Table/Fig-4]. It was observed that the discrepancy was more in early stages of OA than in late stages and the radiological findings lag behind the arthroscopic findings in a given case of OA knee [Table/Fig 8,9 and 10a-d]. As the radiographic grading significantly lag behind the arthroscopic grading in grades 1, 2, 3 the disease could be more serious than it was expected as per the expression of pain and conventional radiographic observations in a given case.
It was observed in our study that the individual arthroscopic gradings were marginally discordant with the pain grading as well. Hence radiological grading and clinical examination findings (Apley’s pain grading) in combination should be considered in overall grading of OA knee with due consideration of the findings from this study while diagnosing and treating the patients with osteoarthritis of knee.
To further the recommendations in this regard large scale longitudinal and cross-sectional studies comparing the individual grades are required to formulate the protocol for accurate diagnosis of OA knee with a given set of radiographic and clinical criteria.
Conclusion
Patients with OA knee present with pain as the predominant symptom. Plain radiography is the commonest modality of investigation to diagnose, grade and plan the management protocol. Direct examination of inner aspect of the joint by arthroscopy is the gold standard modality to quantify the cartilage loss/OA changes, but arthroscopy being an invasive surgical procedure it is not warranted for routine diagnosis of OA knee. Our study has revealed that (K-L) radiographic grades 1,2,3 lag behind the arthroscopic grading and Apley’s pain grading correlates well in 1,2,4 grades and lags behind in grade 3 with the arthroscopic findings. Hence when a patient of OA presents with pain and has discrepancy in radiographic findings, a combination of clinical and radiological findings should be considered in categorisation of the patient while concluding the diagnosis and formulating the treatment protocol. Better radiological criteria have to be evolved by comparing and extrapolating the grade wise findings of arthroscopy on a large number of knee OA cases in future.
Consent
Informed consent from the patients is obtained for publication of case details including clinical photographs.
Competing interests
The author(s) declare that they have no competing/Conflict of interests.
Ethical committee approval
This study has the ethical committee approval. It was approved on 31-12-2012 by a committee of 11 members unanimously.