Tubular Ectasia of Rete Testis with Spermatocele
Neeraj Jain1, Udit Chauhan2, Sonali Sethi3, Vandana Goel4, Sunil Kumar Puri5
1 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
2 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
3 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
4 Assistant Professor, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
5 Head of Department, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Neeraj Jain, Senior Resident, Room no 305, NRDH, G B Pant Hospital, Near Delhi Gate, New Delhi-110002, India.
E-mail: jain_neeraj2@yahoo.co.in
Testicular tumour, Testicular varicocele
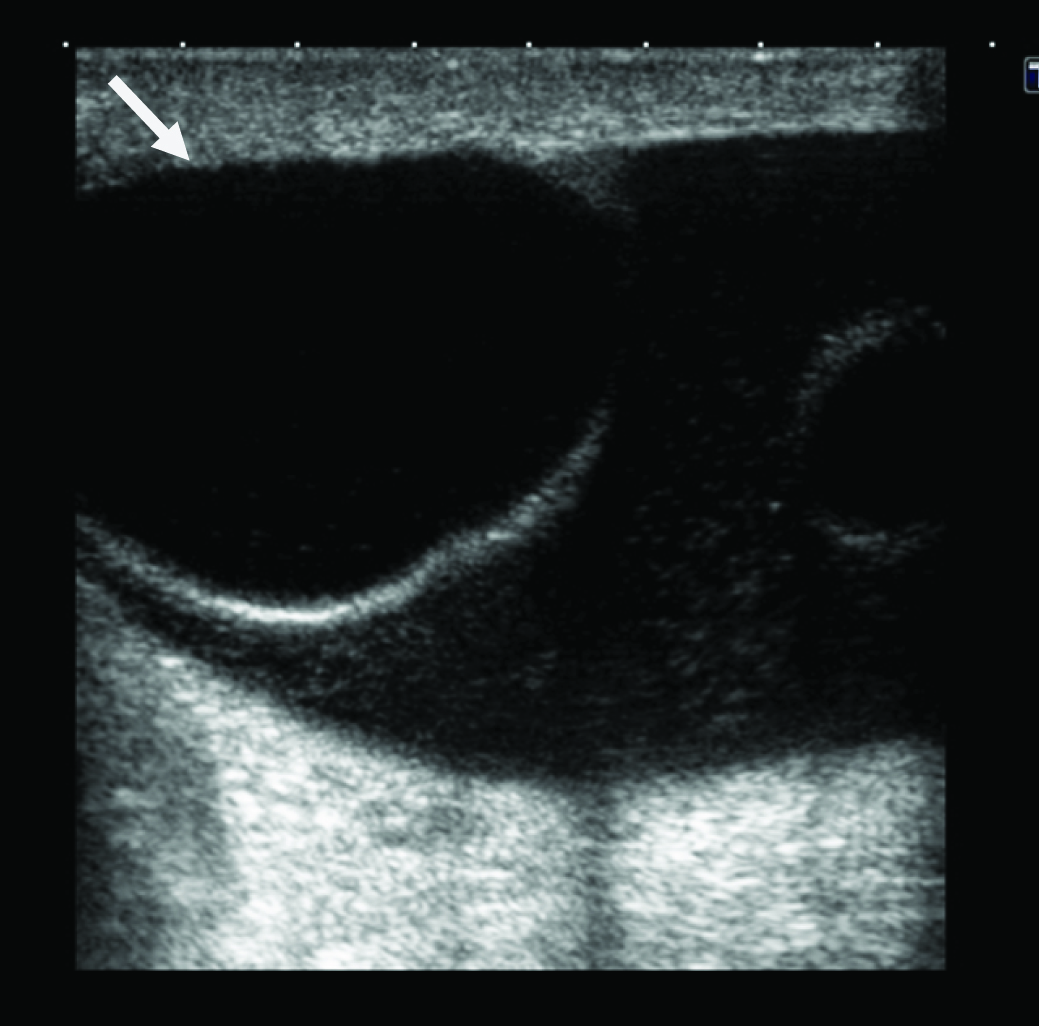
A 55-year-old male patient presented with a slowly enlarging, painless, large soft mass lesion in left scrotal sac for 6 month. On clinical examination the mass lesion could not be separated from testis, hence provisional diagnosis of testicular tumour was made. For further evaluation scrotal ultrasound was performed. In the region of the clinically palpable lump, ultrasound revealed a unilocular, well-circumscribed cystic lesion with moderately thick wall and fine internal echoes [Table/Fig-1]. The size of lesion was approximately 4.5 x 5 cm. It was located cranial to testis, partially replacing left epididymis. No internal or peripheral flow was detected on colour Doppler study. Mild fluid was also noted in scrotal sac, which was consistent with hydrocele. Right testis and epididymis were normal.
Gray scale ultrasound image of left scrotal sac shows a well circumscribed, rounded, unilocular cystic lesion with low level internal echoes located superior to left testis consistent with the diagnosis of spermatocele
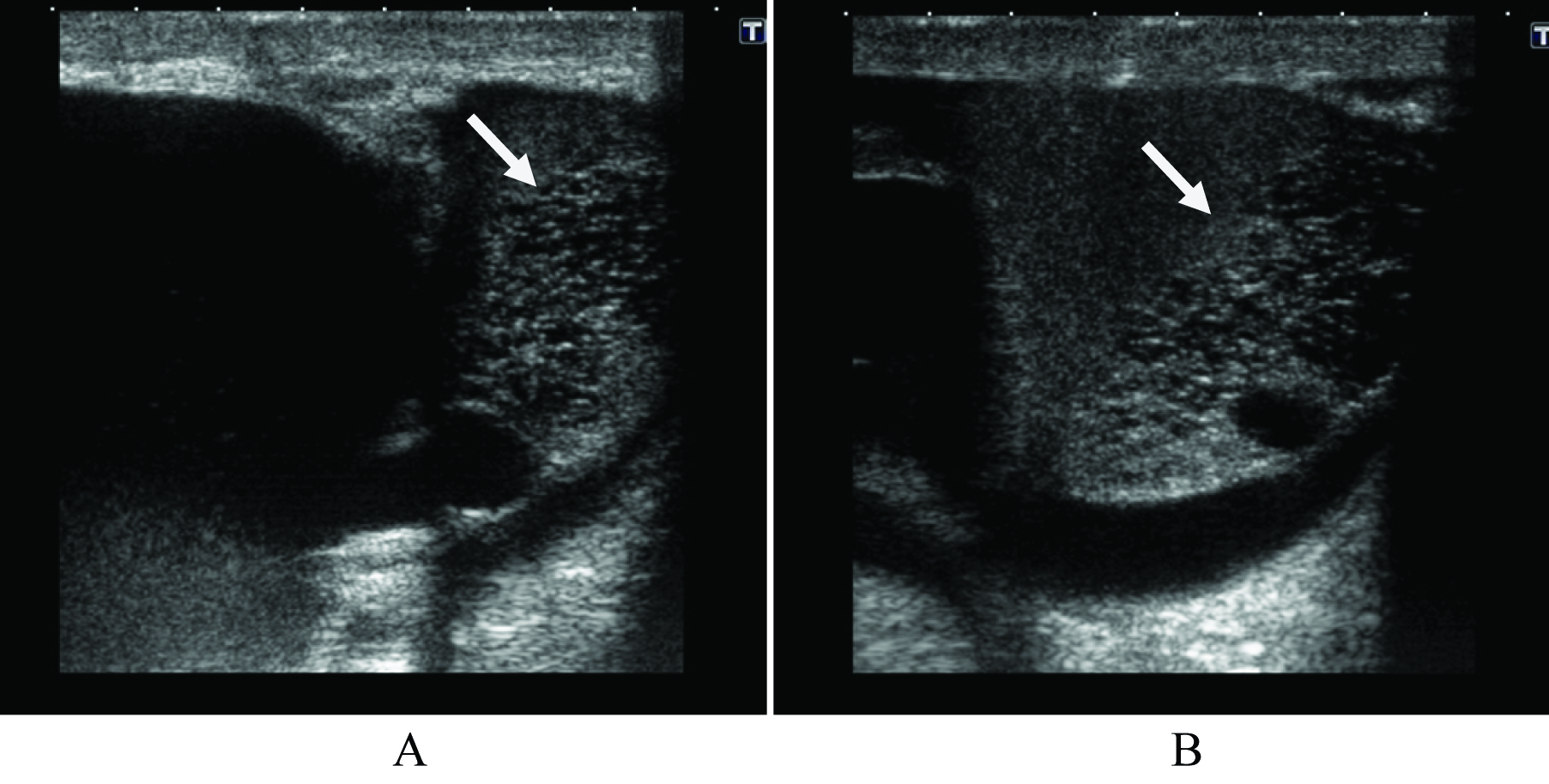
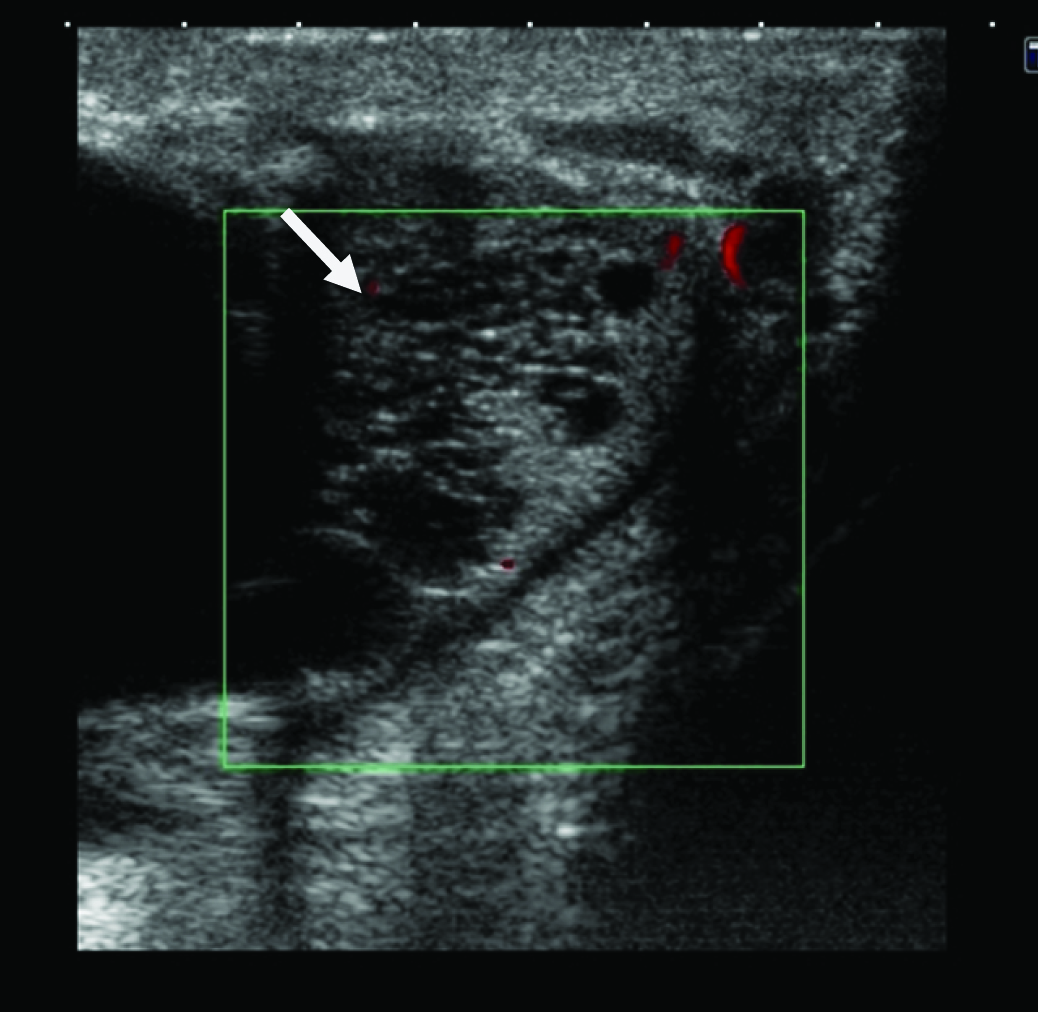
Ultrasound examination also revealed a cluster of multiple, small, anechoic cysts located in the region of testicular mediastinum [Table/Fig-2]. No solid component or calcification was seen. No evidence of any obvious arterial or venous flow was noted in the cysts on colour Doppler study [Table/Fig-3].
Transverse (A), longitudinal (B) gray scale ultrasound images of left testis shows a cluster of multiple small anechoic cystic structures noted in the region of testicular mediastinum with hydrocele
Transverse colour Doppler ultrasound image of left testis shows numerous small cysts with no colour flow
On the basis of characteristic ultrasound and Doppler findings final diagnosis was made of tubular ectasia of rete testis and spermatocele. Because of benign nature of this condition patient was reassured and ask for 6 monthly follow up.
Tubular ectasia of the rete testis is a benign clinical entity in which cystic dilation of rete testis results from partial or complete obliteration of the efferent ducts [1]. The obstruction may occur at different levels and may be classified into intra- or extra-testicular. In testicular lesions, the obstruction generally resulting from previous inflammatory episodes like orchitis, while in extra-testicular lesions, traumatic tearing of epididymis, obstruction from epididymitis, spermatoceles and tunica albuginea cyst and post-vasectomy or other scrotal surgeries are the common causes [2]. Typically this condition affects patients older than 50 year of age. Bilateral lesions have been reported in 29 to 69% of cases [3]. Spermatocele and epididymis cysts are commonly associated with this condition.
Ultrasonography is usually the first and only modality needed to diagnose this condition. Sonographic findings of tubular ectasia of rete testis consists of a cluster of several anechoic rounded and serpiginous tubular structures located in the mediastinum testis without any solid areas or calcific foci. They do not cause mass effect on the adjacent testicular parenchyma. Colour Doppler shows no arterial or venous flow within cystic lesions [4]. Spermatoceles are common extra-testicular lesions caused by cystic dilation of efferent ductules in the region of head of epididymis. On ultrasonography, it appears as a unilocular or multilocular hypoechoic cystic lesion located superior to and separate from testis. It is usually small in size ranging from 1-2cm in size. However large lesions upto 8 cm in size have been reported in the literature [5]. Spermatocele may show low-level echogenic internal echoes due to proteinaceous fluid containing dead sperms. MRI is usually not indicated because of typical appearance on ultrasound. However, if done in doubtful cases, reveals a cluster of round or serpiginous lesions in the hilum of testis, which appear hypointense TI-weighted and hyperintense on T2- weighted images.
The main differential diagnosis includes intra-testicular varicocele and cystic dysplasia of testis. Intra-testicular varicocele is a rare entity, which can give similar appearance on B-mode ultrasonography, however colour Doppler and pulsed Doppler evaluation shows colour flow with characteristic venous spectral waveform that augments during Valsalva maneuver [6]. Cystic dysplasia of testis is thought to be a congenital condition unlike tubular ectasia of rete testis which is an acquired condition. It is seen in children and has similar appearance to tubular ectasia of rete testis [7].
Other differential diagnosis includes epididymal cystadenoma, teratoma, non-Hodgkin’s lymphoma and seminiferous tubules dilatation secondary to testicular neoplasms [1].
Tubular ectasia of rete testis and spermatocele are benign entities With characteristics features on gray scale and colour Doppler examination. This condition should be recognized in older individuals and its awareness can prevent unnecessary investigations and surgical intervention.
[1]. Jorge R, Sonographic findings in non-neoplastic testicular lesionsRadiol Bras 2007 40(1):61-67. [Google Scholar]
[2]. Gooding GA, Leonhardt W, Stein R, Testicular cysts: US findingsRadiology 1987 163:537-38. [Google Scholar]
[3]. Older RA, Watson LR, Tubular ectasia of the rete testis: A benign condition with a sonographic appearance that may be misinterpreted as malignantJ Urol 1994 152:477 [Google Scholar]
[4]. Tartar MV, Trambert MA, Balsara ZN, Mattrey RF, Tubular ectasia of the testicle: Sonographic and MR imaging appearanceAJR Am J Roentgenol 1993 160:539-42. [Google Scholar]
[5]. Lee HH, Fong CJ, Lai CT, Giant Spermatocele with Multilocular Appearance: A Case Report and Literature ReviewJTUA 2005 16:81-84. [Google Scholar]
[6]. Weiss AJ, Kellman GM, Middleton WD, Kirkemo A, Intratesticular varicocele: sonographic findings in two patientsAJR 1992 158:1061 [Google Scholar]
[7]. Nistal M, Regadera J, Paniagua R, Cystic dysplasia of the testis: light and electron microscopic study of three casesArch Pathol Lab Med 1984 108:579 [Google Scholar]