Worldwide, breast cancer accounts for 22.9% of all cancers in women. Breast cancer is the second most common cancer among women in India [1]. The number of diagnosed breast cancer cases is increasing due to increased awareness regarding the disease and implementation of early detection methods.
The major modalities of treatment are chemotherapy, surgery, hormone therapy and radiotherapy [2]. Administration of anticancer drugs before surgery is called neoadjuvant chemotherapy [3]. The tumour may be initially so large, that surgery is impossible or difficult to perform. Neoadjuvant chemotherapy is helpful in such patients with large inoperable breast cancer, to downstage the disease and to make it operable [4]. Thus the procedure becomes easier, less traumatic and more likely to succeed.
There are many regimens available for treatment of breast cancer. The most time tested and popular regimen for neoadjuvant chemotherapy is FAC (5-flurouracil, Adriamycin, Cyclophosphamide). The AT (Adriamycin, Paclitaxel) regimen has been introduced only a few years ago. Data regarding toxicity profile and efficacy of AT regimen is sparse.
To study and compare the toxicity profile between 5-Flourouracil, Adriamycin, Cyclophosphamide (FAC) regimen and Adriamycin, Paclitaxel (AT) regimen in patients with locally advanced breast carcinoma in neoadjuvant setting.
Materials and Methods
A prospective observational study with 50 patients in each treatment arm. Study duration was 12 months from November 2012 to October 2013.
Sample size was calculated as hundred (50 in each treatment group) by expert statistician using the given formula.
p is proportion of the patients with development of toxicities, q is 100-p, d is p1-p2
At 5% significance level,
Inclusion criteria - Female patients of any age group with cytology proven locally advanced breast carcinoma (stage IIB, IIIA, IIIB or lllC AJCC Staging) were considered for the study.
Exclusion criteria- Patients with history of neoplasm other than breast carcinoma, Pre-existing motor or sensory neuropathy, ventricular arrhythmias, congestive cardiac failure, pregnancy, severe infections, severe hepatic or renal insufficiency, distant metastasis and patients on other modes of treatment were excluded from the study.
Patients attending outpatient wing of Radiotherapy Department during the study time period, fulfilling inclusion criteria were enrolled into the study. Written informed consent was obtained from each patient. Detailed elucidation of history and clinical examination were done prior to initiation of treatment. General examination was done to detect anaemia, jaundice, lymphadenopathy, edema and infections. Systemic examination included examination of all the organ systems. Local examination of breast and axilla were done thoroughly. Breast lumps were measured and recorded. Reports of all the relevant baseline investigations were obtained. All collected data were entered in the structured proforma. The treating physician (third author) allocated the patients to receive either FAC or AT regimen based on a random number chart. Data collection was done by the first author and data analysis was done by the second author with the help of expert statistician. Patients in both groups were educated about the probable adverse effects.
Treatment Plan
FAC Regimen
5-Flurouracil 500mg/m2 as intravenous infusion in normal saline.
Adriamycin 50mg/m2 as intravenous infusion in normal saline.
Cyclophosphamide 500mg/m2 as intravenous infusion in normal saline
AT Regimen
Adriamycin 50mg/m2 as intravenous infusion in normal saline.
Paclitaxel 175mg/m2 as intravenous infusion in normal saline.
All drugs are given on day-1 and repeated every 21 days for six cycles.
Premedication
On the previous day 8 p.m.,
Inj. Diphenhydramine 25 mg intravenous
Inj. Ranitidine 50 mg intravenous
Inj. Dexamethasone 8mg intravenous
On the day of chemotherapy repeat 1, 2, 3 and
Inj. Ondansetron 8mg intravenously at 6 a.m., and half an hour before chemotherapy.
Toxicity assessment
Personal interview and clinical examination were done for all patients to detect the development of toxicity manifestations during the course of chemotherapy, after each chemotherapy cycle and after completion of treatment. Laboratory investigation results were also noted. All the data collected were entered in a proforma. The toxicities were graded according to the WHO toxicity grading criteria. In this criterion the toxicities are graded from zero to four. Grade zero denotes that patient is asymptomatic and laboratory results are within normal range. Higher grade indicates greater toxicity. The highest toxicity developed during any cycle was taken as toxicity grade of that patient.
Response assessment
Tumour size measurements were taken after each chemotherapy cycle and at completion of treatment. These values were compared to baseline measurements. Clinical response was defined as at least 50% reduction in the sum of products of bidimensional perpendicular measurements of tumours on two observations, three weeks apart [5].
Ethical considerations
Ethical clearance was obtained from The Human Ethics Committee of the institution. Written informed consent was obtained from all patients included in the study. Study was conducted according to the guidelines given by ICH-GCP.
Statistical Analysis
Data analysis was done with the help of Excel 2007 and SPSS 16 statistical software. The toxicity grades were entered in the Excel 2007 worksheet for each variable. The highest toxicity during any cycle was considered as the toxicity grade for that patient. Chi-square test was used to assess the difference between the two groups as the toxicity grading is a categorical variable. Difference in clinical response also was assessed by Chi-square test. There were no dropouts.
Results
A. Demographic profile
I. Age distribution
The age range of patients included in the study was between 32 years - 66 years. The patients in each regimen were grouped into four intervals (30-39, 40-49, 50-59, 60-69). The maximum number of patients belonged to the age group 50-59. There was no statistically significant difference between the two treatment groups regarding age wise distribution (p-value = 0.968). The mean age of patients in FAC group was 51.9 with a standard deviation of 8.2. In AT group mean age was 51.6 with a standard deviation of 8.0 [Table/Fig-1,2].
Mean Age and standard deviation
| Age | FACn = 50 | ATn = 50 |
|---|
| Mean | 51.9 | 51.6 |
| SD | 8.2 | 8.0 |
Age distribution of patients
| Age group | FAC | AT | Total |
|---|
| N | % | N | % | N | % |
|---|
| 30-39 | 4 | 8% | 3 | 6% | 7 | 7% |
| 40-49 | 14 | 28% | 15 | 30% | 29 | 29% |
| 50-59 | 24 | 48% | 23 | 46% | 47 | 47% |
| 60-69 | 8 | 16% | 9 | 18% | 17 | 17% |
II. Menopausal status
In the present study, 86% subjects were premenopausal. In FAC group 42 women accounting for 84% and in AT group 44 women accounting for 88% had not attained menopause. Analysis shows that there is no statistically significant difference between the two treatment groups regarding menopausal status (p-value = 0.564).
B. Toxicity Profile
1. Overall comparison of toxicities [Table/Fig-3]
Overall comparison of toxicities
| Toxicity | FAC | AT | p-value |
|---|
| Anaemia | 34 (68%) | 12 (24%) | < 0.001 |
| Leucopenia | 36 (72%) | 49 (98%) | 0.008 |
| Thrombocytopenia | 6 (12%) | 1 (2%) | 0.131 |
| Nausea | 49 (98%) | 50 (100%) | 0.144 |
| Vomiting | 45 (90%) | 49 (98%) | 0.156 |
| Diarrhoea | 4 (8%) | 1 (2%) | 0.169 |
| Stomatitis | 30 (60%) | 3 (6%) | <0.001 |
| Peripheral neuropathy | 3 (6%) | 49 (98%) | <0.001 |
| Hyperpigmentation | 41 (82%) | 4 (8%) | <0.001 |
| Alopecia | 50 (100%) | 50 (100%) | |
| Injection site reactions | 29 (58%) | 32 (64%) | 0.722 |
| Allergy | 2 (4%) | 2 (4%) | 1.00 |
| Infections | 5 (10%) | 5 (10%) | 1.00 |
| Myalgia | 2 (4%) | 46 (92%) | <0.001 |
| Arthralgia | 4 (8%) | 41 (82%) | <0.001 |
| Photosensitivity | 30 (60%) | 0 | <0.001patients |
When overall toxicities are taken into consideration anaemia, thrombocytopenia, stomatitis, hyperpigmentation, photosensitivity and diarrheoa were more common with patients receiving FAC regimen, whereas leucopenia, peripheral neuropathy, myalgia, arthralgia, vomiting and injection site reactions were more common with AT regimen.
II. Haematological toxicity:
a) Anaemia [Table/Fig-4]
Comparison of anaemia between FAC and AT regimens
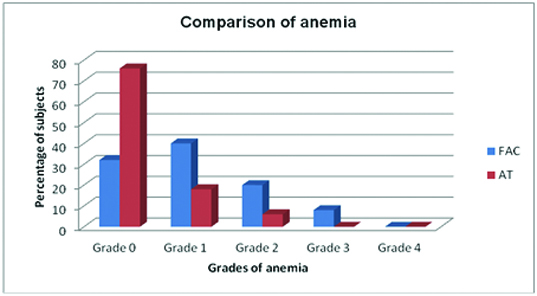
In the current study, 46 patients developed anaemia. Among them, 34 patients were in FAC group and 12 were in AT group. Grade I anaemia was seen in 20 (40%) patients receiving FAC regimen and 9 (18 %) patients receiving AT regimen. Grade II anaemia was seen in 10 (20%) patients of FAC group and 3 (6%) patients of AT group. Grade III anaemia was seen only in patients receiving FAC regimen. None of the patients in both groups progressed to grade IV anaemia. So, anaemia was more frequent in patients receiving FAC regimen and this difference was statistically significant (p-value < 0.001).
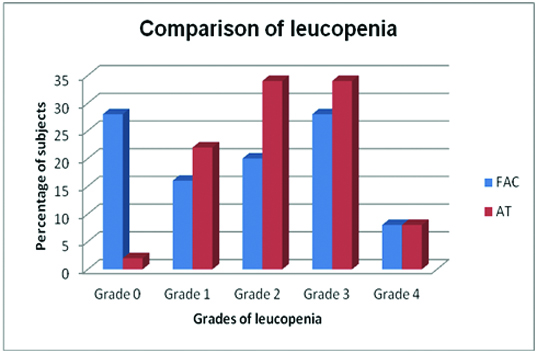
Leucopenia developed in 85 patients taken up for the current study. Among patients receiving FAC regimen 36 (72%) developed leucopenia, whereas 49 (98%) patients in AT regimen developed this toxicity. The incidence of leucopenia was high in patients receiving AT regimen and this difference was statistically significant. (p-value = 0.008) [Table/Fig-5].
Comparison of leucopenia between FAC and AT regimens
c) Thrombocytopenia [Table/Fig-6]
Comparison of thrombocytopenia
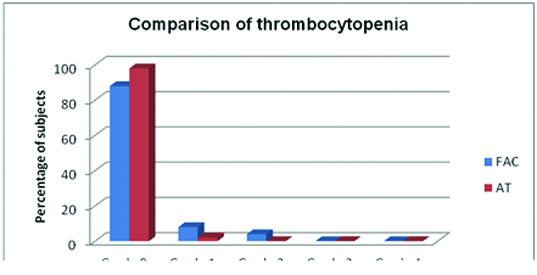
Seven patients included in the current study developed thrombocytopenia. Grade I thrombocytopenia developed in five patients, while grade II developed in two patients. In FAC group six (12%) patients had thrombocytopenia, whereas only one patient in AT group developed this toxicity. The difference was not statistically significant (p-value = 0.131).
III. Gastrointestinal toxicity
Vomiting [Table/Fig-7].
Comparison of vomiting between FAC and AT regimens
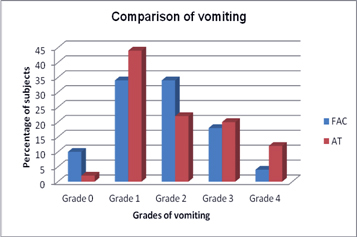
Vomiting was more frequent with AT regimen. Among patients receiving AT regimen, 49 (98%) developed vomiting. In FAC group 45 (90%) patients developed this toxicity.
Grade IV vomiting was seen in 4% patients of FAC group and 12% patients of AT group. The difference between FAC and AT regimens regarding vomiting was not statistically significant (p-value = 0.156)
c) Diarrhoea [Table/Fig-8]
Comparison of diarrhoea between FAC and AT regimens
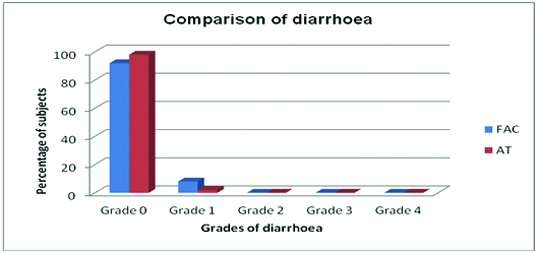
Five patients taken up for the study developed grade I diarrhoea. In FAC group four (8%) patients and in AT group one (2%) patient developed this toxicity. No patients went in for grade II, III or IV diarrhoea. Occurrence of diarrhoea was more common among patients receiving FAC regimen. This difference is not statistically significant (p-value = 0.169).
d) Stomatitis [Table/Fig-9]
Comparison of stomatitis between FAC and AT regimens
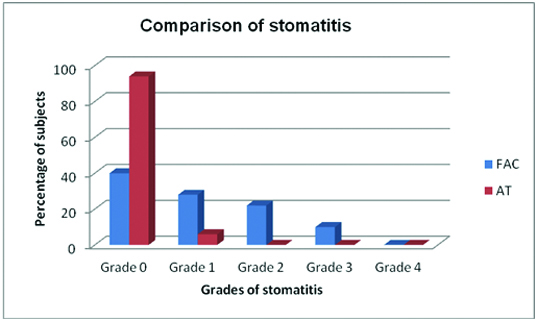
Stomatitis was found to be more common in patients receiving FAC regimen than AT regimen. In FAC group 30 (60%) patients developed stomatitis. Among them 14 (28%) had grade I, 11 (22%) had grade II and five (10%) had grade III toxicity. In contrast only three (6%) patients in AT regimen developed grade I stomatitis. No patient in AT group progressed to grade II, III or IV stomatitis. The difference in the incidence of stomatitis between FAC and AT regimens was found to be statistically significant (p-value <0.001).
IV. Peripheral neuropathy [Table/Fig-10]
Comparison of peripheral neuropathy
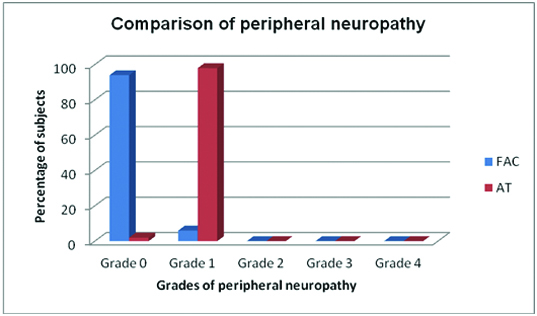
Peripheral sensory loss was an evident neurotoxicity, which occurred in 52 patients included in this study. The incidence of peripheral neuropathy was higher in patients on AT regimen. Out of the 50 patients, 49 (98%) developed grade I peripheral neuropathy in AT group. In FAC group only three (6%) developed this toxicity. Grade II, III or IV toxicity was not seen in any patient in both groups. The difference between the two regimens regarding peripheral neuropathy was statistically significant (p-value <0.001). A p value of <0.05 was considered to show a significant difference between two groups regarding any parameter.
V. Dermatological toxicity
a) Hyperpigmentation [Table/Fig-11]
Comparison of hyperpigmentation
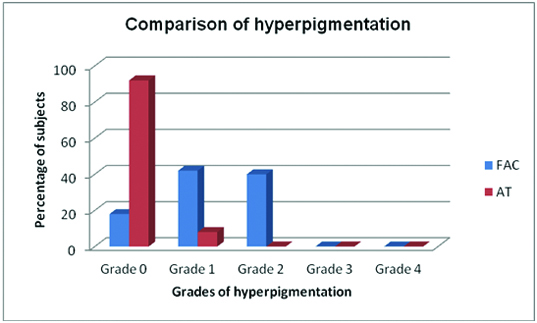
Hyperpigmented patches on skin were more common in patients receiving FAC regimen. Out of the 50 patients 41 (82%) developed hyperpigmentation of skin in FAC group. In contrast only 4 (8%) developed this toxicity in AT group. All cases of hyperpigmentation were in grade I category. The difference in occurrence of hyperpigmentation between FAC and AT regimens was statistically significant (p-value <0.001)
b) Alopecia
Alopecia means loss of hair from the head or body. Grade I alopecia means mild hair loss and grade II means total hair loss. All patients taken up for the current study developed grade II alopecia in both FAC and AT groups.
c) Injection site reactions
In FAC group 29 (58%) patients had injection site reactions. Among them 25 (50%) had grade I and four (8%) had grade II toxicity. In AT group 32 (64%) patients developed injection site reactions. None of the patients in any group progressed to grade III or IV toxicity. There is no statistically significant difference between the two groups regarding this toxicity.
VI. Allergy
Four patients taken up for the study developed allergy to drugs. Two patients from both FAC and AT groups had this adverse reaction. Only grade I allergic reactions were observed.
VII. Infections
Infections developed in 10 patients taken up for the study. All were grade I respiratory tract infections. There were no serious or life threatening cases.
VIII. Toxicities not included in WHO criteria
a) Myalgia [Table/Fig-12]
Comparison of myalgia between FAC and AT regimens
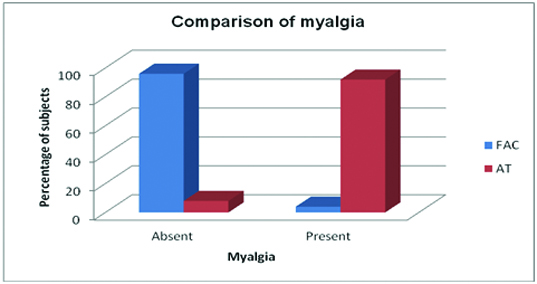
Among 100 patients taken up for the study, 52 developed myalgia. It was a major toxicity in patients receiving AT regimen. Myalgia was complained by 46 (92%) patients in AT group. But, in FAC group only two (4%) developed myalgia. There was a statistically significant difference between the two treatment groups regarding myalgia (p-value <0.001).
b) Arthralgia [Table/Fig-13]
Comparison of arthralgia between FAC and AT regimens
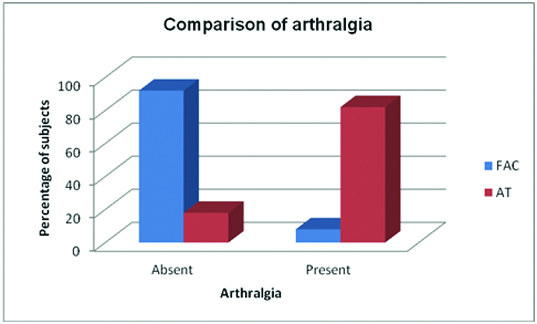
Forty patients taken up for the study developed arthralgia. It was more common among patients receiving AT regimen. In AT group 41 (82%) patients had arthralgia. In contrast only 4 (8%) patients from FAC group had this toxicity. The difference between FAC and AT regimens regarding arthralgia was statistically significant (p-value <0.001)
c) Photosensitivity [Table/Fig-14]
Comparison of photosensitivity
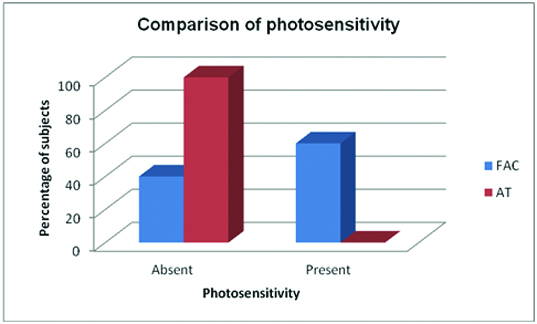
Photosensitivity was seen exclusively in patients receiving FAC regimen. Among them 30 (60%) patients had this toxicity. None in AT group developed photosensitivity.
Comparison of clinical response
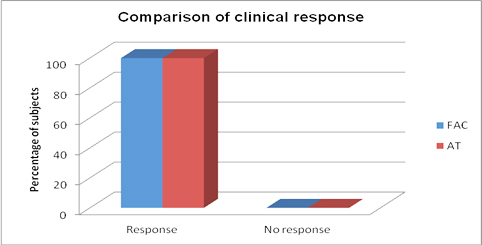
In the current study clinical response is defined as at least 50% reduction in the sum of products of bidimensional perpendicular measurements of all tumours on two observations, 3 weeks apart. Both FAC and AT regimens were 100% effective according to this parameter.
Discussion
The aim of the present study was to compare the toxicity profiles of two popular regimens used for neoadjuvant chemotherapy in patients with locally advanced breast cancer. These are 5-Fluorouracil, Adriamycin, Cyclophosphamide (FAC) regimen and Adriamycin, Paclitaxel (AT) regimen. Patients on both FAC and AT regimens developed toxicities, but the pattern of toxicities were different. Based on the observations from current study, any one regimen cannot be considered better than the other with regard to toxicities.
Age plays a significant role in the etiology, clinical response and prognosis of breast cancer. The demographic profile of patients in both regimens was comparable in the current study. The age range of patients included in the study was between 32 and 66 years. The majority of patients were more than 50-years-old. The mean age of the patients were 51.9 in FAC group and 51.6 in AT group. In the prospective observational study conducted by Dhanya et al., the age range of patients was between 20 and 65 [1]. Majority of patients belonged to the age group 36-50 years and the mean age was 44 years. In the study done by Stephen E Jones et al., with FAC regimen age range was 23 to 67 years and mean age was 47 [6].
There was a significantly higher occurrence of anaemia in FAC group (68%) than AT group (24%). In the study conducted by Dhanya et al., 63% patients on FAC regimen developed anaemia [1]. Incidence of leucopenia was higher with AT regimen than FAC (98% vs 72%). Similar results were obtained from the study by Jacek Jassem et al., among patients with metastatic breast cancer [5]. In the above mentioned study, 99% patients receiving AT regimen and 93% patients receiving FAC regimen developed leucopenia. Thrombocytopenia was more common in FAC group (12%). But the difference between FAC and AT regimens regarding thrombocytopenia was not statistically significant.
Incidence of nausea and vomiting was comparable between FAC and AT regimens. Vomiting was seen in 90% patients in FAC regimen and 98% patients in AT regimen. There was no statistically significant difference. In the study conducted by Jacek Jassem et al., nausea or vomiting developed in 76% patients in FAC regimen and 60% patients in AT regimen [5].
Diarrhoea developed in four (8%) patients in FAC group and 1 (2%) patients in AT group. This difference was not statistically significant. In the study conducted by Jacek Jassem et al., 9% patients in FAC group and 29% patients in AT group had diarrhoea. This difference was also statistically insignificant [5].
In the current study, there was a statistically significant difference in the incidence of stomatitis between the two regimens. In FAC group 30 (60%) patients developed stomatitis. In contrast only three (6%) patients in AT group had this toxicity. In the study conducted by Dhanya et al., 90% patients on FAC regimen had stomatitis [1].
Peripheral neuropathy was significantly higher in patients receiving AT regimen when compared to FAC. In AT group, 49 (98%) patients developed peripheral neuropathy. In FAC group only three (6%) developed this toxicity. In the study conducted by Jacek Jassem et al., peripheral neuropathy developed in 62% patients of AT group and 3% patients of FAC group [5].
Hyperpigmentation was significantly high in patients receiving FAC regimen than AT regimen. Out of the 50 patients 41 (82%) developed hyperpigmentation of skin in FAC group. In contrast only four (8%) developed this toxicity in AT regimen. In the study conducted by Dhanya et al., 98% patients in FAC group had hyperpigmentation of skin [1].
Alopecia developed in all patients (100%) of FAC and AT group. Similar results were obtained in the study conducted by Dhanya et al., [1]. Also, in the study by J Gehl et al., among patients receiving AT regimen, 100% alopecia was observed [7].
In the current study, there was no statistically significant difference between FAC and AT groups regarding injection site reactions. In FAC group 29 (58%) and in AT group 32 (64%) patients had local reactions at injection site. In the study done by Dhanya et al., 98% patients on FAC regimen developed this adverse reaction [1].
Incidence of infections was same (10%) in patients receiving both FAC and AT regimens. In the study by Stephen E Jones et al., 6% patients receiving FAC regimen developed infections [6]. In a study conducted by JY Pierga et al., among patients on FAC regimen, 14% developed infections [8].
There was a statistically significant difference between the two treatment groups regarding myalgia and arthralgia. Myalgia was complained by 46 (92%) patients on AT regimen and two (4%) patients on FAC regimen. Arthralgia was present in 41 (82%) patients of AT group and four (8%) patients of FAC group. Similar results were obtained in the study by Jacek Jassem et al., In that study, myalgia or arthralgia developed in 73% patients on AT regimen and 17% patients on FAC regimen [5].
Photosensitivity was seen exclusively in patients receiving FAC regimen. Among them 30 (60%) patients had this toxicity. Similar results were obtained in the study by Dhanya et al. In that study 68% patients on FAC regimen had photosensitivity [1].
In the current study clinical response was defined as at least 50% reduction in the sum of the products of bidimensional perpendicular measurements of all tumours on two observations, three weeks apart. Both FAC and AT regimens were 100% effective according to this parameter. In the study by Jacek Jassem et al., 68% patients on AT regimen and 55% patients on FAC regimen had a clinical response [5]. That study was conducted in patients with metastatic breast cancer. In the study by J Gehl et al with AT regimen overall response rate was 83% [7].
When overall toxicities are taken into consideration anaemia, thrombocytopenia, stomatitis, hyperpigmentation, photosensitivity and diarrhoea were more common with patients receiving FAC regimen. Statistically significant difference was present regarding anaemia, stomatitis, hyperpigmentation and photosensitivity. Clinicians can avoid FAC regimen in patients predisposed to these toxicities. For example, if a patient has anaemia and is diagnosed with LABC, it is better to avoid FAC regimen. AT regimen with less chance for developing anaemia is the better option for such a patient.
Leucopenia, peripheral neuropathy, myalgia, arthralgia, vomiting and injection site reactions were more common in AT regimen. But statistical significance was detected only with leucopenia, peripheral neuropathy, myalgia and arthralgia. Clinicians can avoid AT regimen in patients predisposed to these toxicities. If a patient with arthritis develops LABC and is treated with AT regimen, there can be worsening of arthralgia. FAC regimen with less chance for arthralgia is the better option for such patients.
Study Limitations
This study was a prospective observational study. For better assessment of toxicity profile and efficacy, a randomized controlled trial is preferable. The study period was short. So, delayed toxicities like carcinogenesis could not be monitored. The sample size was small. Larger numbers of patients are needed for proper assessment of toxicity profile, efficacy and ADL score.
Conclusion
FAC and AT regimens have different pattern of toxicities and any one regimen cannot be considered better compared to the other regarding toxicities. Both regimens are equally efficacious according to predefined clinical response criteria. Patient’s predisposition to toxicities may govern the selection of regimen for treatment.