Progress has been rapid in describing the dermatoglyphs. It was often claimed to be associated with several diseases like congenital heart disease, schizophrenia, cancer, diabetes and other genetic disorders [9–13].
Therefore, we guess that there may be an association between dermatoglyphic patterns and coronary artery disease patients of Ningxia, China. Hence, the present study was attempted to investigate the dermatoglyphic patterns of a normal control cohort and the patient cohort (CAD) among Han people from Ningxia, China in order to select a non-invasive anatomical marker of CAD risk and thus facilitate early detection and treatment.
Materials and Methods
Our subjects were 258 male Ningxia residents, China (age 30-73 years) during 2009 to 2012. The participants were recruited from the same Han ethnic group. Normal controls (n=129, mean age±S.D. =47.5±6.6 years) were resident natives and all exhibited healthy physical and mental states. The patient group (n=129, mean age ±S.D.=50.5±6.7 years) were CAD patients diagnosed by the method of coronary arteriography called the golden standard method in the general hospital affiliated to Ningxia Medical University. The patients had been ruled out from inherited mutations, congenital defects and other diseases. The parents and grandparents of all subjects were from the same Han ethnic group. All agreements were approved by the Ningxia Medical University Committee for the Protection of Human Subjects, and each of participants gave informed written consent before the experiment.
Standard ink methods for fingerprints and palm prints as described in Cummins and Midlo were used [14]. The fingerprints and palm prints were taken on a white glossy paper by rolling the special finger technique using red ink pad [Table/Fig-1]. Then the digital photographs for the prints were taken and analysed with Adobe Photoshop software. All the participants were told to clean their hands properly to remove dirt and stains before the test, and they were asked to be relaxed and to co-operate to achieve the movement of the fingers during the experiment. We excluded subjects with injuries to the fingers.
Fingerprints and palm prints, the ridge counts, and ATD angle of a subject taken during study
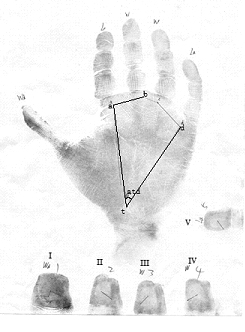
The dermatoglyphic traits considered in the present study includes finger ball pattern types, ridge counts (finger ridge counts—FRC;total finger ridge counts—TFRC), and ATD angles. No distinction was made between the varieties of whorl (W) patterns; also tented arch was just recorded as an arch (A). Loop was recorded as either ulnar loops (LU) or radial loop (LR). All the patterns were as defined by Penrose [15]. The ridge counts were done by reference to Zhang Hai-guo [16]. A straight line was drawn to join A and B triradii and the number of intersecting ridges counted, which gave A-B ridge counts (A-BRC). The A,T triradii and T,D triradii were also connected with line, and the two line formed an angle was called ATD angle as shown in [Table/Fig-1]. The various digits were designated as follow: Thumb-I; Index finger-II; Middle finger-III; Ring finger-IV; Little finger-V. L and R stood for left and right respectively.
Statistical Analysis
Chi-square test, t-test were used for the statistical analysis in this study. Data was analysed by SPSS software (v:13). The difference was considered to be significant if the p-value was less than 0.05.
Results
Frequency distribution of finger print patterns is shown in [Table/Fig-2]. The results revealed that a higher frequency of whorls in cases was seen in all digits on both hands as compared to controls. [Table/Fig-3] summarized the data of [Table/Fig-2] and showed the actual observations and frequency of each pattern type per individual. It also presents the results of Chi-square test between two groups. The cardinal feature was that the order of prevalence of whorl, loop and arch in cases was whorl>loop>arch whereas in controls was loop>whorl>arch. The differences of whorls and ulnar loops noted between the two groups were significant (p<0.01, p<0.01 respectively). Although little difference in radial loops and arch occurred but they were not significant (p>0.05, p>0.05 respectively).
Frequency distribution of finger print patterns in coronary artery disease and controls (%)
| Hand | Finger | Control | CAD |
|---|
| A | LU | LR | W | A | LU | LR | W |
|---|
| L | I | 4.65 | 43.41 | 1.55 | 50.29 | 0.00 | 33.34 | 0.77 | 65.89 |
| II | 2.33 | 41.08 | 8.53 | 48.06 | 6.20 | 30.23 | 7.75 | 55.81 |
| III | 2.33 | 58.14 | 1.55 | 37.98 | 3.10 | 49.61 | 2.33 | 44.96 |
| IV | 2.33 | 37.98 | 1.55 | 58.14 | 1.55 | 30.23 | 0.77 | 67.44 |
| V | 3.88 | 74.42 | 0.00 | 21.71 | 2.33 | 70.54 | 0.00 | 27.13 |
| R | I | 3.88 | 40.31 | 0.77 | 55.04 | 3.88 | 29.45 | 0.00 | 66.67 |
| II | 3.88 | 38.76 | 9.30 | 48.06 | 3.10 | 28.68 | 10.85 | 57.36 |
| III | 1.55 | 49.61 | 2.33 | 46.51 | 2.33 | 49.61 | 1.55 | 46.51 |
| IV | 1.55 | 37.21 | 0.77 | 60.47 | 0.77 | 30.23 | 0.00 | 68.99 |
| V | 2.33 | 68.99 | 0.77 | 27.91 | 0.77 | 61.24 | 0.00 | 37.98 |
Digital pattern observations (N) and the χ2 test results of the frequency of finger print patterns (%) in coronary artery disease and controls
| Hand | Digit patterns |
|---|
| A | | LU | | LR | | W | |
|---|
| N | % | N | % | N | % | N | % |
|---|
| Control | 37 | 2.87 | 632 | 48.99 | 35 | 2.71 | 586 | 45.43 |
| CAD | 31 | 2.40 | 533 | 41.32 | 31 | 2.40 | 695 | 53.88 |
| χ2 value | 0.75 | 15.33 | 0.25 | 18.42 |
| p-value | >0.05 | <0.01 | >0.05 | <0.01 |
[Table/Fig-4] shows the mean finger ridge counts and the total finger ridge counts on both hands of CAD and controls. The results revealed that finger ridge counts (FRC) and total finger ridge counts (TFRC) in cases were higher than those of in normal. However, all the p-values of the t-test results in [Table/Fig-4] were greater than 0.05. So we did not find significant difference between two groups in our study. [Table/Fig-5] shows the mean ATD angles between two groups. In our study, the ATD angle was found to be significantly wider in CAD than in normal controls on both palms (p<0.05). The table also shows the mean A-BRC on both palms. The results revealed that A-BRC on the right palm in cases was significantly higher than that of in controls (p<0.05), but it was not found on the left palm (p>0.05).
Mean and standard error of each finger ridge counts, total finger ridge counts, t- test results on both hands in coronary artery disease and controls
| FRC | Number | Control | CAD | t-value | p-value |
|---|
| I | L | 129 | 16.63±6.02 | 16.64±4.92 | 0.89 | 0.38 |
| R | 129 | 16.64±6.10 | 16.66±5.14 | 0.98 | 0.15 |
| II | L | 129 | 12.39±4.82 | 12.40±5.02 | 1.61 | 0.11 |
| R | 129 | 12.38±5.23 | 12.43±5.12 | 1.08 | 0.15 |
| III | L | 129 | 12.41±4.15 | 12.42±5.15 | 1.44 | 0.13 |
| R | 129 | 12.43±4.54 | 12.46±4.23 | 1.82 | 0.08 |
| IV | L | 129 | 17.22±4.52 | 17.72±5.43 | 1.11 | 0.27 |
| R | 129 | 17.72±5.48 | 17.74±6.12 | 1.38 | 0.17 |
| V | L | 129 | 11.61±3.89 | 11.62±4.54 | 1.71 | 0.09 |
| R | 129 | 11.62±4.12 | 11.65±4.10 | 1.82 | 0.07 |
| TFRC | 1290 | 141.05±4.88 | 141.74±4.97 | 1.45 | 0.15 |
Mean and standard error of ATD angles, A-B ridge counts,
| index | Number | Control | CAD | t-value | p-value |
|---|
| ATD angles | L | 129 | 43.25±4.14 | 47.89±5.21 | 2.34 | 0.02* |
| R | 129 | 43.31±4.95 | 47.99±5.74 | 2.11 | 0.04* |
| A-BRC | L | 129 | 33.98±3.82 | 35.80±4.45 | 1.71 | 0.09 |
| R | 129 | 33.89±3.65 | 35.89±3.80 | 2.38 | 0.01* |
t- test results on both palms in coronary artery disease and controls
* p-value < 0.05
Discussion
Dermatoglyphs begins to develop during the sixth to seventh week of the first trimester, and the development is finished in the fourth month of fetal life. After the beginning of the second trimester, much of the heart is already formed. Nevertheless, the anlage of the ridge lines and the volar fat pads are present earlier. It might be possible that the factors arising in the critical period of pregnancy may affect the development of the heart and the ridges of fingers and plams. Dermatoglyphic similarities have been correlated with several illnesses and in fact the evaluation of fingerprints in patients with heart disease [17] has been reported. For the present cross-sectional study finger print patterns, finger ridge counts (FRC), total finger ring counts (TFRC), ATD angle, A-B ridge counts (ABRC) of both hands and palms have been studied.
Early studies have shown that a high frequency of whorls was more frequently associated with artery disease such as aortic stenosis, aortic co-arctation, and tetralogy of Fallot [17,18]. A Sanchez Cascos had reported that whorls occurred in 15-30 percent of finger-prints in the controls, but much more frequent in aortic stenosis (41%), aortic co-arctation (37%), and Fallot’s tetralogy (33%) [18]. Similar result was observed in the present study. The whorls were 45.43 percent of fingerprints patterns in controls and 53.88 percent in CAD cases. There was a significant statistical difference between controls and CAD patients in whorl pattern (p<0.01). Previous studies add to our finding suggesting that a high frequency of whorls may be correlated with CAD.
Ulnar loops were clearly dominant (60-70%) in the congenital heart groups as well as in the controls, and radial loops were rare in earlier study [18]. In the present study, we also found the similar phenomenon, but there was a significant higher ulnar loops in controls than in CAD patients (p<0.01). However, in the dermatoglyphic analysis of the digital patterns between Down’s syndrome and normal controls, it indicated that there was a statistically significant difference in loop pattern between cases and normals, which was 96% loop pattern in cases as against 63.6% in normals [19]. We speculated that the reason of causing these diverse results may be the inherent difference between different diseases and the discrepancy of subjects in different researchs. The specific reason remained to be further researched.
We also found that the FRC and TFRC in cases were higher than those of in normal [Table/Fig-4]. However, compared with the previous studies in congenital heart disease revealed that total ridge count were more frequent in aortic stenosis, aortic co-arctation, and tetralogy of Fallot [9,20]. There was no significant difference between two groups in our study. We are unable to explain why this should be so.
Many studies have already showed that the ATD angle was significantly wider in congenital heart disease than in normal controls [9,20], Milton Alter had reported that all subtypes of CHD had a wider ATD angle than controls [9]. It was most marked in the Fallot’s tetralogy group where the mean ATD angles were 51°, compared with 41° in the controls in A Sanchez Cascos’s study [21]. In our study, the values of ATD angles observed for CAD were 47.89 in left hand and 47.99 in right hand, which were clearly abnormal as these were far above the normal value 43.25 and 43.31. Therefore, the present study appeared to support the results of most previous studies that CAD, including other types of heart disease, may be associated with abnormal ATD angles. Hence, it suggests that the ATD angles are a good non-invasive anatomic indicator for the assessment of individuals, who are likely to show some symptoms of CAD later in life.
The average A-BRC in normal individuals has been put at 34 while values higher than this were said to be abnormal [22]. In our study, the A-BRC observed in CAD group was increased towards the range of the abnormal groups as it was higher in both hands than 34. We did find stronger relationship between A-BRC and CAD on the right Palm, but not for the left palm. We do not have any good explanation for this fact. This indicates that A-BRC may have a relationship with CAD.
In summary, abnormal dermatoglyphics, especially the ATD angles, may yet provide a clue to the identification of CAD due to a genetic cause or to a teratogen operating during early gestation when both the heart and the skin ridges are forming.
Limitations of The Study
In our study, there were still some limitations. We only got the fingerprints and palm prints of male individuals in Ningxia han, China, the related materials of female should be needed. And the size of samples should be larger in the future to get more useful information.
Conclusion
The presence of abnormally high A-B ridge count, ATD angles and the frequency of whorls are a characteristic dermatoglyphic pattern of CAD which could be very useful in its early diagnosis. These data are therefore recommended as a tool which could be used for early diagnosis of CAD.
Although limited conclusions could be drawn based on this preliminary study, dermatoglyphics may have a future role in identifying men either with or at increased risk for CAD. Analysis of dermatoglyphics in patients suspected of having CAD should be encouraged.
t- test results on both palms in coronary artery disease and controls
* p-value < 0.05