Frenulum Sparing Circumcision: Step-By-Step Approach of a Novel Technique
Sunil Purshotham Shenoy1, Prashanth Kallaje Marla2, Pritham Sharma3, Narayana Bhat4, Amrith Raj Rao5
1 Head, Department of Urology, A J Institute of Medical Sciences & Research Centre, Mangaluru, Karnataka, India.
2 Professor, Department of Urology, A J Institute of Medical Sciences & Research Centre, Mangaluru, Karnataka, India.
3 Assistant Professor, Department of Urology, A J Institute of Medical Sciences & Research Centre, Mangaluru, Karnataka, India.
4 Professor, Department of Paediatric Surgery, A J Institute of Medical Sciences & Research Centre, Mangaluru, Karnataka, India.
5 Consultant Urological Surgeon, Wexham Park Hospital, Wexham, Royal County of Berkshire, SL2 4HL, UK.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sunil P. Shenoy, Head, Department of Urology, A.J. Institute of Medical Sciences & Research Centre, Mangaluru-575003, Karnataka, India.
E-mail: drsunilpshenoy@gmail.com
Objective
Circumcision, by most conventional methodologies, involves division of the frenulum and excision of the entire foreskin covering the glans. This seemingly simple procedure is occasionally associated with dreadful and devastating complications. We describe a new frenulum-sparing technique that circumvents some of the potential complications of conventional techniques and could also potentially help preserve preputial role in sexual function.
Materials and Methods
An initial dorsal slit, three fourths of the way up to the corona is extended laterally and obliquely on either side, to meet the preputial edge, 3-4 mm from the frenulum. A broad sleeve of sub-coronal mucosa is thus preserved. The frenulum is left untouched, leaving a wide skin bridge connecting the mucosal sleeve with the shaft skin. The raw area is closed with interrupted, synthetic absorbable sutures. Over a three year period, 42 patients were circumcised using this technique.
Results
No significant complications like frenular bleed, painful postoperative erections, chordee, meatal stenosis, or urethra-cutaneous fistula were observed in any patient. The cosmetic results were pleasing.
Conclusion
The frenulum-sparing technique of circumcision is a promising modification to the various existing techniques. The method described is technically easier to perform than conventional frenulum-dividing procedures and has an acceptable cosmesis. Further randomised controlled studies on larger cohorts are necessary to establish the true benefits of this technique over established procedures.
Complications, Frenular artery, Prepuce, Phimosis
Introduction
Circumcision is the most commonly performed surgical procedure worldwide [1–3]. While neonatal circumcision is often carried out for religious and social indications, its protective effect on prevention of invasive penile cancer is well documented [4]. Adult circumcisions are usually carried out for medical indications, commonest being phimosis. Complications of circumcision reported in the literature vary widely from <1% to as high as 55% [5–7]. The complications listed include bleeding, infection, excess or inadequate skin removal, skin adhesions, meatitis, meatal stenosis, lymphoedema, altered glans sensitivity and urethro-cutaneous fistula amongst others [7,8]. Different techniques of carrying out circumcision and modifications thereof have been described to reduce the risk of complications. Most techniques involve removing the entire foreskin over the glans, including the division of the frenulum. Controversy still reigns as to the ideal extent of preputial preservation during circumcision. Even when medically indicated, the procedure is usually carried out on the lines of religious circumcision wherein the entire preputial skin is removed. Herein, we describe step-by-step, a novel technique of circumcision that retains more prepuce while sparing the frenulum and we believe this technique avoids some of these complications.
Materials and Methods
During the period January 2011 to December 2013 we performed 42 circumcisions using this modified technique in the age group 4 to 64 years [Table/Fig-1]. Follow-up was done till December, 2014 (1-4 years). All patients (and guardians of minors) selected gave informed consent for frenular preservation during the procedure. The procedure followed was in accordance with the standards prescribed by the Institutional Ethics committee.
Demographic data and indications for circumcision
| Age group (Years) | Number of patients (42) | Indication for circumcision |
|---|
| 4-10 | 5 | Phimosis (5) |
| 10-20 | 6 | Phimosis (6) |
| 20-30 | 10 | Phimosis (8),Painful erections (2) |
| 30-40 | 9 | Phimosis (8)Cosmesis (1) |
| 40-50 | 5 | Phimosis (3)Balanitis (2) |
| 50-60 | 4 | Phimosis (3)Posthitis (1) |
| 60-70 | 3 | Phimosis (2)Adjunct to TURP (1) |
Phimosis or cosmesis was the indication for circumcision in majority of cases [Table/Fig-1]. One patient underwent the procedure to facilitate introduction of the 26 French resectoscope during transurethral prostatic resection (TURP). Exclusion criteria during the selection process included religious circumcision, long redundant prepuce, frenular breve, scarred frenulum, suspected underlying cancer of the penis, and severe posthitis or Balanitis Xerotica Obliterans (BXO) involving the entire foreskin.
The technique involves the initial creation of a dorsal slit that extends three-fourths of the distance from meatus to the corona. Then, lateral incisions from the proximal end of the dorsal slit are made obliquely, parallel to the corona maintaining their original distance from the margin. The two incisions terminate at the preputial edge, 3-4 millimeters away from the frenulum on either side. The skin and mucosal margins are approximated with 40 synthetic absorbable sutures after control of minor bleeding points with bipolar cautery. The frenular artery is not encountered during the procedure. The prepuce should easily be drawn over the coronal margin and remain in position, leaving the meatus well exposed [Table/Fig-2a-g,3a-c].
Step-wise depiction of the frenulum-sparing technique; h) Pathway of lymphatic flow to the shaft skin from the circum-coronal mucosal sleeve.
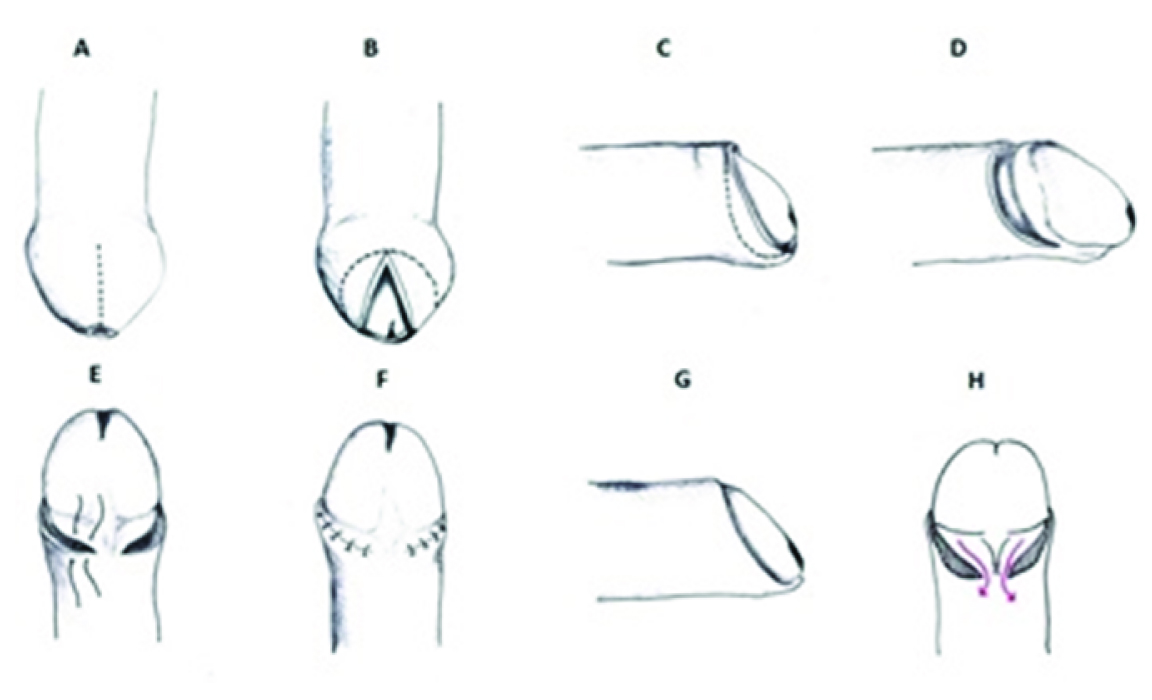
Appearance: a) preoperative; b) Intact frenular bridge; c) immediate postoperative; d) 1 month postoperative.

Results
No significant complications like frenular bleed, painful postoperative erections, chordee, meatal stenosis, circumcoronal lymphoedema of residual preputial skin or urethra-cutaneous fistula were observed in any patient. The cosmetic results were pleasing [Table/Fig-3d].
Discussion
In our technique, we remove the phimotic foreskin but avoid disturbing the frenulum and its adjoining web. Sparing the frenulum as in our technique circumvents some of the complications associated with circumcision. Frenular artery bleed that usually requires a re-operation is eliminated [7,8]. Absence of a suture line on a transected frenulum avoids painful postoperative erections. One of the recognized complications is removal of excess skin, especially on the ventral aspect. This often leads to painful chordee and in worst cases, the scrotal skin is drawn upwards during an erection, leading to uncomfortable and unpleasant sexual intercourse. In our technique, as the ventral aspect of the skin is untouched, such an eventuality is avoided. Another rare complication reported in the literature is the occurrence of urethro-cutaneous fistula [7–11]. Although most cases are due to plastic devices used in the neonates, this has also been reported in adults undergoing circumcision. The mechanism of injury is varied and has been postulated as due to excess diathermy or by the inadvertent use of excess suture material to secure bleeding from the frenular vessels [8]. Our technique eliminates any risk to the underlying urethra. Meatal stenosis is a recognized complication of circumcision, especially involving neonates. However, meatal stenosis is also reported in adults and Persad et al., have suggested a role of the division of the frenular artery in its pathogenesis [12]. Our technique preserves the frenular artery and we have not seen any case of meatal stenosis in our series.
Partial preputial preservation as described herein requires a broad sleeve of circum-coronal mucosa to be retained, to allow the skin to ride over the coronal margin. There are reports describing circumferential lymphoedema of this sleeve in operations involving penile degloving, possibly as a consequence of severing of its lymphatic continuity with the skin of the shaft [13]. We have indeed observed a similar situation after conventional frenulum-dividing circumcision as well, leading to a persistent woody ring around the corona that mars cosmesis. Williams and Kapila in their paper quote “Although penile lymphoedema following circumcision has been reported, there is a paucity of information regarding the aetiology and management of such a problem and accounts in the literature are anecdotal” [7]. Using our novel technique, we have not come across a case of lymphoedema in spite of leaving behind a broad sub-coronal mucosal sleeve and we theorize this to the fact that there is uninterrupted lymphatic flow through the bridge of the frenular skin back into the skin of the shaft and thence to the superficial inguinal group of lymph nodes [Table/Fig-2h].
Several publications have highlighted important functional aspects of the frenulum and prepuce [14,15]. Frenulum is richly innervated by fine-touch neuro-receptors, such as Meissner’s corpuscles. The frenulum has also been implicated in arousal and erectile properties with studies suggesting erectile dysfunction is patients wherein it has been altered by circumcision [16]. Indeed, the study by Sorrells et al., suggested that circumcision removed five most sensitive parts of the human penis including the frenulum near the ridged band and at the muco-cutaneous junction [15]. The preservation of the frenular web is also associated with prolonged ejaculation latency time [17]. In patients with spinal cord injury, vibratory stimulation applied to the frenulum of the penis produced ejaculates sufficient for intrauterine insemination [18]. By sparing this important structure in our technique, these unique qualities that the frenulum possesses are protected.
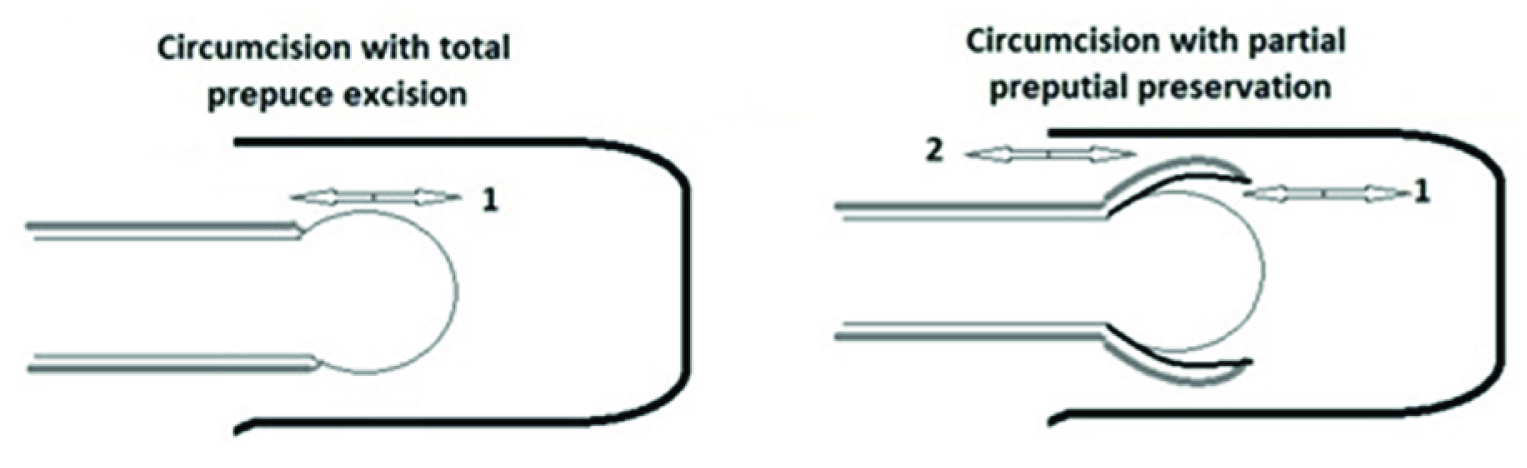
Our technique, involves preservation of significant amount of prepuce in addition to sparing the frenulum. While re-emphasizing the role of the prepuce in sexual arousal due to its neuro-sensitivity as in the case of the frenulum, preservation of glanular surface moisture and hence its sensitivity may be an additional factor. We postulate that presence of two interfaces for coital friction instead of one, when the glans has a partially retained skin cover as in our technique, could provide for enhanced sensational feed-back during coitus [Table/Fig-4].
Mechanical factors at play during coitus: a) Single frictional interface (1) during coitus with the entire prepuce excised; b) Two frictional interfaces (1 and 2) with partial preputial preservation.
Conclusion
We describe a step-by-step approach to our technique of frenulum-sparing circumcision. The technique is easy to perform and reduces likely hood of certain complications that could result in not only post-surgical morbidity but also functional and cosmetic dissatisfaction for the patient. We accept that 42 cases are insufficient to assess the complication rate, and larger randomised controlled trials with longer follow-up periods would truly confirm the advantages of our technique over established procedures. The postulated theoretical beneficial effects of the technique on sexual function however need to be further studied.
[1]. Okeke LI, Asinobi AA, Ikuerowo OS, Epidemiology of complications of male circumcision in Ibadan, NigeriaBMC Urol 2006 6:21 [Google Scholar]
[2]. Weiss HA, Larke N, Halperin D, Schenker I, Complications of circumcision in male neonates, infants and children: a systematic reviewBMC Urol 2010 10(2) [Google Scholar]
[3]. Crawford DA, Circumcision: a consideration of some of the controversyJournal of child health care 2002 6:259-70. [Google Scholar]
[4]. Schoen EJ, Oehrli M, Colby CJ, Machin G, The Highly Protective Effect of Newborn Circumcision Against Invasive Penile CancerPediatrics 2000 105:E36 [Google Scholar]
[5]. Speert H, Circumcision of the newborn; an appraisal of its present statusObstetrics and gynecology 1953 2:164-72. [Google Scholar]
[6]. Patel H, The problem of routine circumcisionCan Med Assoc J 1966 95:576-81. [Google Scholar]
[7]. Williams N, Kapila L, Complications of circumcisionThe Br J Surg 1993 80:1231-36. [Google Scholar]
[8]. Kaplan GW, Complications of circumcisionThe Urol Clin N Am 1983 10:543-49. [Google Scholar]
[9]. Sancaktutar AA, Pembegul N, Bozkurt Y, Kolcu B, Tepeler A, Multiple circumferential urethrocutaneous fistulae as a rare complication of circumcision and review of literatureUrol 2011 77:728-29. [Google Scholar]
[10]. El-Bahnasawy MS, El-Sherbiny MT, Paediatric penile traumaBJU Int 2002 90:92-96. [Google Scholar]
[11]. Yazici M, Etensel B, Gursoy H, A very late onset urethral fistula coexisting with skin bridge after neonatal circumcision: a case reportJ Ped Surg 2003 38:642-43. [Google Scholar]
[12]. Persad R, Sharma S, McTavish J, Imber C, Mouriquand PD, Clinical presentation and pathophysiology of meatal stenosis following circumcisionBr J Urol 1995 75:91-93. [Google Scholar]
[13]. Austoni E, Altieri VM, Tenaglia R, Trans-scrotal penile degloving, a new procedure for corporoplastiesUrologia 2012 79:200-10. [Google Scholar]
[14]. Taylor JR, Lockwood AP, Taylor AJ, The prepuce: specialized mucosa of the penis and its loss to circumcisionBr J Urol 1996 77:291-95. [Google Scholar]
[15]. Sorrells ML, Snyder JL, Reiss MD, Eden C, Milos MF, Wilcox N, Fine-touch pressure thresholds in the adult penisBJU Int 2007 99:864-69. [Google Scholar]
[16]. Song B, Cai ZM, Possible function of the frenulum of prepuce in penile erectionAndrologia 2012 44:23-25. [Google Scholar]
[17]. Hosseini SR, Mohseni MG, Salavati A, Yosefi R, Role of frenular web preservation on ejaculation latency timeActa Med Iran 2012 50:676-78. [Google Scholar]
[18]. Pryor JL, LeRoy SC, Nagel TC, Hensleigh HC, Vibratory stimulation for treatment of anejaculation in quadriplegic menArchives of Phys Med Rehab 1995 76:59-64. [Google Scholar]