Multiple patient-specific factors are associated with apical root resorption during orthodontic treatment, including morphological features such as root shapes [3], or oral habits [4], biological and genetic factors [5,6], endodontic treatment [7], sex [8], age [9], and anomalies in dentition such as malocclusions [10]. Moreover, treatment-specific variables include treatment with extractions [11], mechanical factors [12], treatment duration [11,13], amount and direction of the orthodontic force applied [14,15], and the amount and type of tooth movement [16,17]. For example, it appears that the intrusion of teeth causes approximately four times more root resorption than extrusion [18], however, it has also been demonstrated that extrusive movement is not without risk [18].
Low-friction mechanics are now commonly used, and previous clinical investigations have analysed their biomechanical properties [19–22]. However, differences may exist among different low-friction clinical protocols. The purpose of the current study was to evaluate the amount of root resorption using a specific low-friction treatment protocol, Integrated Straight-Wire (ISW). The amount of root resorption was investigated in a retrospective study involving patients treated by the same orthodontist. Furthermore, because of the limitation existing in the evaluation of the root resorption using panoramic radiographs [23], we combined the analysis with lateral cephalograms and application of a trigonometric correction.
Materials and Methods
Our retrospective study investigated the orthodontic records of 93 patients (53 females and 40 males), who were selected from the orthodontic department of the Dental School of the University of Brescia in 2013, with the following inclusion criteria: there was no history of trauma or bruxism, endodontic or prosthetic treatments, or previous root reshaping involving the maxillary and mandibular incisors, and were only successfully completed cases. Only non-extraction cases were included, with no criteria given relatively to the skeletal class. Their mean age was 14.2 years (SD=2.6), with a median value of 13 years.
An a priori sample size (n) calculation, with the apical root resorption as the main outcome, was performed fixing a power (β) of 90% (zβ = 1.28) and an α of 5% (zβ/2=1.96). The difference considered as clinically significant was 5% between the mean (μ) pre and post-treatment root length, with a standard deviation (σ) of 10%, estimated from a preliminary study (n=10). The calculation was carried using the following formula [24]:

Consequently, because of the retrospective nature of our study, we chose a representative sample size of 93, including 10 more patients because of possible variations in the standard deviation of the data of the final sample.
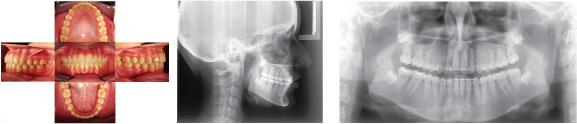
All patients were consecutively treated by the same orthodontist with the same low-friction ISW protocol using a fixed multi-brackets appliance with passive self-ligating (Damon©, Ormco Co., USA) pre-adjusted (0.022X0.028 slot) braces. The arch-wires used in the basic set-up were all Damon©Q form as follows: maxillary and mandibular 0.014 NiTi or 0.014 CuNiTi during stage I: 0.014 X 0.025 NiTi, 0.018 x 0.025 CuNiTi during stage II: 0.019 x 0.025 SS during stage III: and 0.019 X 0.025 SS, 0.019 X 0.025 TMA, 0.016 X 0.025 SS, 0.016 SS or 0.018 SS during stage IV: the protocol finished with 0.019 X 0.025 SS or 0.019 X 0.025 TMA. The mean treatment duration was 2.1 years, with patients showing mild crowding (between 0 and 4 mm) at the beginning of treatment [Table/Fig-1-3,4-6].
Pre-treatment intra oral pictures, latero-lateral cephalogram, and orthopantomography

Post-treatment intra oral pictures, latero-lateral cephalogram, and orthopantomography
Ethics
The procedures followed were in accordance with the ethical standards of the responsible institutional committee on human experimentation and with the Helsinki Declaration of 1975 that was revised in 2000.
Measurement techniques
In order to analyse the degree of root resorption, panoramic and lateral cephalometric radiographs were examined before and after orthodontic treatment. Each subject had his/her pre and post-treatment panoramic and cephalometric film taken by the same radiology technician using a standardized procedure. Each film was uploaded digitally as a .jpeg file and cephalometric analysis of pre and post-treatment lateral radiographs was performed using the Nemoceph NX© software. The change of inclination of maxillary and mandibular central incisors was then measured (with reference to the long axis of the tooth, from the incisal edge to the root apex).
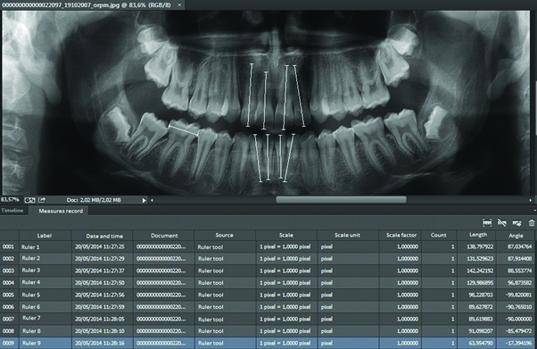
Pre and post-treatment panoramic radiographs were evaluated using Adobe Photoshop CS6® [Table/Fig-7]. Initial and final tooth lengths of maxillary and mandibular incisors (with reference to the long axis of the tooth, from the incisal edge to the root apex, through the midpoint of the CEJ) were measured in pixel using the tool “ruler”. For each film, the length of the mesio-distal diameter of the crown of the mandibular right first molar was measured in pixels, and then all the measurements were converted using this value as the specific unit for each patient. This procedure ensured the normalization of the data for the intra-patient comparison, assuming no changes in the coronal diameter, despite the changes in the root length. Two different clinicians performed each measurement.
Representative screenshot of the panoramic radiography measurements uploaded digitally
In order to ensure that the shortening of the length (ΔL) that showed in the frontal plane was not a result of the change of inclination of the teeth in the sagittal plane (Δδ) [Table/Fig-8], the values of the pre-treatment teeth lengths were adjusted using the following formula:
Sample representation of the angle between the pre and post-treatment inclination of the maxillary central incisors (Δδ), superimposed on the ANS-PNS of the cephalometric X-ray, and differential length in the frontal plane (ΔL)
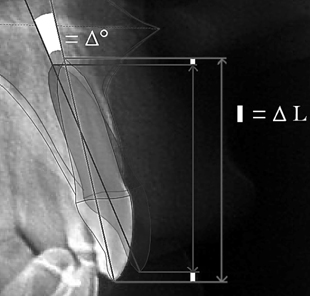

Once this trigonometric correction was adopted, it was possible to compare the values for pre- and post-treatment teeth lengths. The same amount of correction was adopted for both the central and lateral incisors, even though lateral incisors could have slightly different inclination changes compared to the centrals.
Statistical Analysis
All the data were uploaded in a Excel© (Microsoft, USA) worksheet and analysed using SPSS Statistics© v.22 software (SPSS, USA). We evaluated the normality of the data distribution by the asymmetry and kurtosis values and with the Kolmogorov-Smirnov and Shapiro-Wilk tests p < 0.05 taken as significant. Then, a two-tailed Student’s t-test was used for paired values to evaluate the differences between the pre- and post-treatment measurements p < 0.05 taken as significant. We estimated the inter-rater absolute agreement through intraclass correlation coefficient (ICC), using two-way ANOVA with mixed-effects average measures (ranging from 0 to 1, with 0 indicating no consistency and 1 indicating a perfect consistency among raters).
Results
Each pre and post-treatment average tooth length was calculated. Then, depending on the differential inclination, the respective trigonometric correction was applied to obtain a pre-treatment length that was comparable to the post-treatment length without an inclination bias [Table/Fig-9]. [Table/Fig-10,11] summarizes the outcomes of our measurements. The values of the pre- and post-treatment inter-rater absolute agreement in the measurement of the parameters are showed in [Table/Fig-12].
Average values and respective standard deviations and confidence intervals of the pre-treatment tooth lengths, post-treatment tooth lengths, angle between the pre and post-treatment inclination, trigonometric correction and adjusted pre-treatment tooth lengths after the trigonometric correction was applied. All of the length measurements use the mesiodistal diameter of the crown of the mandibular right first molar as the standard unit
| | | pre-treatment length | post-treatment length | differential inclination (Δδ) | trigonometric correction (ΔL) | pre-treatment length # |
|---|
| | | (units) | (units) | (°) | (units) | (units) |
|---|
| | | AV | SD | CI | AV | SD | CI | AV | SD | CI | AV | SD | CI | AV | SD | CI |
|---|
| maxillary | central | right | 2.18 | 0.21 | 2.14-2.22 | 2.18 | 0.21 | 2.14-2.23 | 1.43 | 6.68 | 0.07-2.79 | 0.01 | 0.03 | 0.00-0.02 | 2.19 | 0.21 | 2.15-2.23 |
| left | 2.15 | 0.20 | 2.11-2.19 | 2.16 | 0.21 | 2.12-2.21 | 1.43 | 6.68 | 0.07-2.79 | 0.01 | 0.03 | 0.00-0.02 | 2.16 | 0.20 | 2.12-2.20 |
| lateral | right | 1.99 | 0.22 | 1.95-2.03 | 2.02 | 0.22 | 1.97-2.06 | 1.43 | 6.68 | 0.07-2.79 | 0.01 | 0.03 | 0.00-0.02 | 2.00 | 0.22 | 1.94-2.04 |
| left | 2.00 | 0.21 | 1.94-2.04 | 2.03 | 0.22 | 1.99-2.08 | 1.43 | 6.68 | 0.07-2.79 | 0.01 | 0.03 | 0.00-0.02 | 2.01 | 0.21 | 1.96-2.05 |
| mandibular | central | right | 1.63 | 0.18 | 1.59-1.67 | 1.58 | 0.21 | 1.54-1.62 | 2.19 | 5.40 | 1.09-3.29 | 0.01 | 0.03 | 0.01-0.01 | 1.64 | 0.19 | 1.60-1.68 |
| left | 1.64 | 0.21 | 1.60-1.64 | 1.58 | 0.22 | 1.54-1.63 | 2.19 | 5.40 | 1.09-3.29 | 0.01 | 0.03 | 0.01-0.01 | 1.65 | 0.21 | 1.60-1.69 |
| lateral | right | 1.73 | 0.19 | 1.69-1.77 | 1.67 | 0.22 | 1.63-1.72 | 2.19 | 5.40 | 1.09-3.29 | 0.01 | 0.03 | 0.01-0.01 | 1.73 | 0.19 | 1.69-1.77 |
| left | 1.72 | 0.20 | 1.68-1.76 | 1.66 | 0.23 | 1.61-1.71 | 2.19 | 5.40 | 1.09-3.29 | 0.01 | 0.03 | 0.01-0.01 | 1.73 | 0.20 | 1.68-1.77 |
AV= average SD= standard deviation, CI= confidence interval, #= trigonometric correction applied, unit = mesiodistal diameter of the crown of the mandibular right first molar
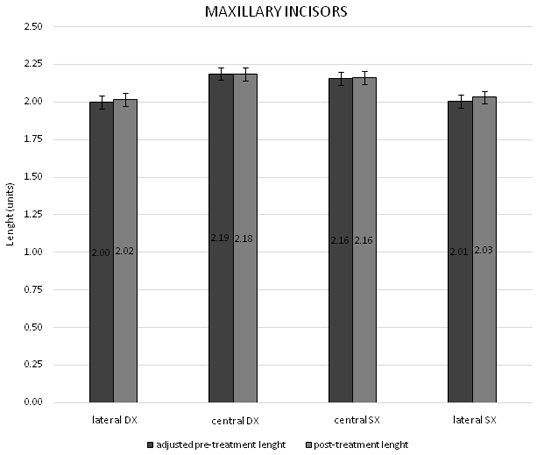
Mean pre and post-treatment length values of the maxillary incisors and their respective confidence intervals. The measurements use the mesiodistal diameter of the crown of the mandibular right first molar as unit.
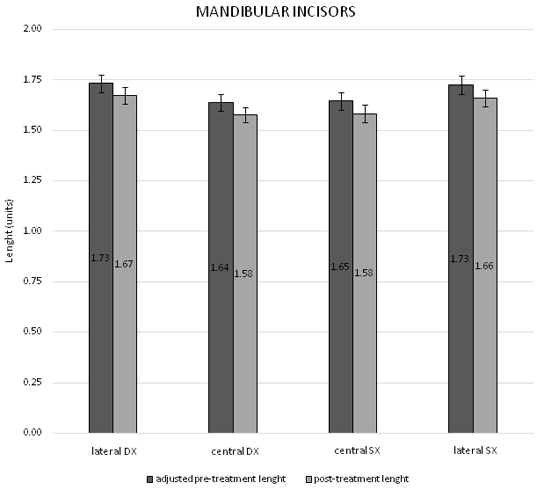
Mean pre-treatment and post-treatment length values of the mandibular incisors and the respective confidence intervals. The measurements use the mesiodistal diameter of the crown of the mandibular right first molar as unit
Intraclass correlation coefficient (ICC) values of the pre- and post-treatment measurements, representing the inter-rater absolute agreement
| | | | ICC |
|---|
| pre-treatment | maxillary | right | central | 0.981 |
| lateral | 0.975 |
| left | central | 0.985 |
| lateral | 0.950 |
| mandibular | right | central | 0.980 |
| lateral | 0.989 |
| left | central | 0.972 |
| lateral | 0.987 |
| post-treatment | maxillary | right | central | 0.992 |
| lateral | 0.995 |
| left | central | 0.991 |
| lateral | 0.985 |
| mandibular | right | central | 0.992 |
| lateral | 0.992 |
| left | central | 0.988 |
| lateral | 0.993 |
The data sets for the tooth measurements were normally distributed in both the Kolmogorov-Smirnov and Shapiro-Wilk tests (p > 0.05; [Table/Fig-13]).
Analysis of the normal distribution of the tooth length data
| | | | Kolmogorov-Smirnov | Shapiro-Wilk |
|---|
| | | | coeff. test | sign | coeff. test | sign |
|---|
| maxillary | central | right | pre-treatment | 0.08 | 0.20 | 0.99 | 0.38 |
| post-treatment | 0.05 | 0.20 | 0.99 | 0.40 |
| left | pre-treatment | 0.06 | 0.20 | 0.98 | 0.16 |
| post-treatment | 0.06 | 0.20 | 0.99 | 0.52 |
| lateral | right | pre-treatment | 0.06 | 0.20 | 0.98 | 0.31 |
| post-treatment | 0.05 | 0.20 | 0.99 | 0.96 |
| left | pre-treatment | 0.07 | 0.20 | 0.98 | 0.07 |
| post-treatment | 0.05 | 0.20 | 0.99 | 0.51 |
| mandibular | central | right | pre-treatment | 0.05 | 0.20 | 0.99 | 0.59 |
| post-treatment | 0.05 | 0.20 | 0.99 | 0.58 |
| left | pre-treatment | 0.06 | 0.20 | 0.99 | 0.96 |
| post-treatment | 0.06 | 0.20 | 0.99 | 0.46 |
| lateral | right | pre-treatment | 0.05 | 0.20 | 0.99 | 0.50 |
| post-treatment | 0.04 | 0.20 | 0.99 | 0.90 |
| left | pre-treatment | 0.06 | 0.20 | 0.99 | 0.50 |
| post-treatment | 0.04 | 0.20 | 0.99 | 0.92 |
Using Student’s t-tests, we found no statistically significant difference in the lengths of the maxillary incisors between the pre and post-orthodontic treatment values for the central, lateral or both sides p > 0.05. On the contrary, there was a statistically significant difference in the shortening of the mandibular incisors between the pre- and post-orthodontic treatment values for the centrals and laterals, and on both the left and right side p < 0.01 [Table/Fig-14].
Analysis of the differences between pre and post-treatment tooth lengths
| | | AV | SD | CI | sign |
|---|
| | | (%) | (%) | (%) |
|---|
| maxillary | central | right | 0.3 | 9.3 | (-1.6)-(2.2) | 0.90 |
| left | 0.6 | 9.3 | (-1.3)-(2.5) | 0.81 |
| lateral | right | 1.4 | 10.1 | (-0.7)-(3.5) | 0.36 |
| left | 1.8 | 10.9 | (-0.4)-(4.0) | 0.27 |
| mandibular | central | right | -3.1 | 12.7 | (-5.7)-(-0.5) | ** |
| left | -3.1 | 13.0 | (-5.7)-(-0.5) | ** |
| lateral | right | -3.1 | 10.9 | (-5.3)-(-0.9) | ** |
| left | -3.4 | 12.5 | (-5.9)-(-0.9) | ** |
AV= average; DS= standard deviation; CI= confidence interval; *= <0.05; **= <0.01; ***= <0.001
Discussion
This clinical retrospective investigation analysed root resorption after a low-friction orthodontic treatment. Tooth length measurements were performed on panoramic radiographs that are the standard radiographic exams required by orthodontists at the initiation and end of treatment, patients did not need to undergo further radiography.
As a result of difficulties in discriminating the crown from the root on panoramic X-rays, our measurements involved the whole tooth, assuming the absence of changes in the tooth crown and ascribing any possible shortening only to the root. As panoramic radiographs are not suitable for the qualitative evaluation of the root shape [23,25], and periapical radiographs were not available for all patients, we limited our evaluation of resorption on length measurements. X-rays were in digital format and direct measurements were not possible, therefore, we carried a pixel unit measurement on the digital format.
As panoramic radiographs are based on a para-frontal plane, different inclinations of the incisors between the pre and the post-treatment may result in length changes. In order to reduce the above-mentioned error, the difference between pre and post-treatment incisal inclination was measured on the respective lateral cephalogram, and each patient had his/her initial tooth length modified using a mathematical correction. This trigonometric correction can set the root length that the pre-treatment tooth would exhibit in the post-treatment panoramic radiograph to normalize the intra-tooth comparison. However, this method is based on a theoretical trigonometric formula, and further studies would be useful to evaluate its accuracy and biological cost-effectiveness. Additionally, as showed in our previous investigations [26], a comparison between 2D and 3D methods is worth of interest in the orthodontic treatment planning, especially when multiple evaluations are needed.
Studies that use panoramic radiographs to measure changes in root lengths between pre and post-treatment values that do not take modification of the incisal inclination into account should consider this potential bias.
Our group of patients was selected with a mild grade of crowding, because our aim was to evaluate the most representative sample concerning a non-extractive orthodontic protocol by means of a specific straight-wire, low-friction technique. In order to allow a qualitative comparison, if our results were transferred onto the scale of Malmgren (grade 0 to 4) [27], the maxillary incisors would be represented by grade 0 or 1 and the mandibular incisors by no more than grade 2, none of our patients had grade 3 resorption or more. Although Previous studies found an overall percentage of root resorption of 7.8% SD = 6.9% [28], milder degrees of root resorption could be the result of many variables, including lower amounts of root movement [11,29,30]. For this reason, our findings could be less evident than the results reported by the literature.
As reported by other authors [19], a slight increase in root lengths was shown in the maxillary lateral incisors (1.4-1.8%), although this was not statistically significant in our study p > 0.05. This could be attributed to the completion of root development in younger patients, which would be in accordance with the median age of our sample (13 years) and with the root completion sequence.
Limitations
Even though we followed a standardized protocol during the X-ray exams, a different level of distortion may exist between pre and post-treatment radiographs. This bias was reduced by measuring the mesiodistal diameter of the crown of the mandibular right first molar and using it as a baseline unit for all the other measurements on the same X-ray, in order to normalize the intra-patient comparison. However, a certain degree of distortion may still be present.
To distinguish between the left and right central incisors on the cephalometric radiograph is difficult, we therefore selected the most inclined tooth in the maxillary and mandibular arch and then applied the obtained correction to both the central and lateral incisors. Even though our estimate was specific for the central incisors, it was useful for the laterals but less effective. Therefore, the lateral incisors values reported in our results may be less realistic than the values related to the central incisors.
Further researches including different amount of crowding and comparisons with other X-ray examinations, e.g. high accuracy CBCT linear measurements [31], shall assess the reliability of the methods used in this preliminary study.
Conclusion
In patients with mild crowding and consequent low amount of root movement, a straight wire low-friction orthodontic treatment can lead to a post-treatment decrease of mandibular central and lateral incisor root lengths on both the right and left side approximately of 3%. However, our analysis on panoramic radiographs found no evidence that resorption involved the maxillary incisors. The use of a trigonometric correction may reduce the limitation of the 2D radiographs, but further studies are needed to assess its accuracy.
AV= average SD= standard deviation, CI= confidence interval, #= trigonometric correction applied, unit = mesiodistal diameter of the crown of the mandibular right first molar
AV= average; DS= standard deviation; CI= confidence interval; *= <0.05; **= <0.01; ***= <0.001