Treatment of Virgin OHVIRA Syndrome with Haematometrocolpos by Complete Incision of Vaginal Septum without Hymenotomy
Niyazi Tug1, Mehmet Akif Sargin2, Ayhan Çelik3, Turgut Alp4, Ilter Yenidede5
1 Associate Professor, Department of Obstetrics and Gynecology, Fatih Sultan Mehmet Research and Training Hospital, Istanbul, Turkey.
2 Specialist, Department of Obstetrics and Gynecology, Fatih Sultan Mehmet Research and Training Hospital, Istanbul, Turkey.
3 Specialist, Department of Obstetrics and Gynecology, Fatih Sultan Mehmet Research and Training Hospital, Istanbul, Turkey.
4 Specialist, Department of Urology, Fatih Sultan Mehmet Research and Training Hospital, Istanbul, Turkey.
5 Specialist, Department of Obstetrics and Gynecology, Fatih Sultan Mehmet Research and Training Hospital, Istanbul, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mehmet Akif Sargın, Balıkesir Cad. Soganlık Yeni Mahalle Uprise Elite Sitesi C 2 Blok D:1 Kartal, Istanbul Turkey.
E-mail: drmehmetakifsargin@yahoo.com
Mullerian malformations result from defective fusion of the Mullerian ducts during development of the female reproductive system and have an incidence of 2-3%. The American Fertility Society classification of Mullerian anomalies is the most commonly utilized standardized classification. The least common form of these malformations is Herlyn-Werner-Wunderlich syndrome characterized by obstructed hemivagina and ipsilateral renal anomaly (OHVIRA). This syndrome has been described with case reports since 1922. Early diagnosis and surgery that include drainage of fluid and resection of the vaginal septum is necessary for OHVIRA to prevent late complications (i.e. pyocolpos, chronic cryptomenorrhea). Here in we report a case of Herlyn-Werner-Wunderlich syndrome that hymen has been preserved during the operation of non-fenestrated transverse vaginal septum resection with hysteroscopy.
Herlyn-Werner-Wunderlich syndrome, Hysteroscopy, Transverse vaginal septum
Case Report
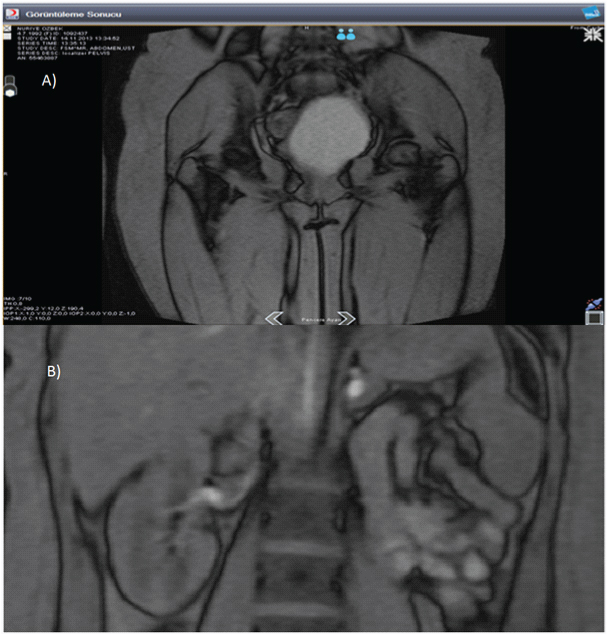
A 21-year-old virgin patient presented with spasmodic and mild periodic abdomino pelvic pain and distention for one year. She had regular cycles with a menarche age of 12. Physical examination revealed abdominal distention and normal external genitalia with annular and intact hymen. Ultrasonography, magnetic resonance imaging and renal scintigraphy revealed uterus didelphys, left haematometrocolpos, obstructed hemivagina and renal agenesis [Table/Fig-1]. The patient asked for protection of hymen for socio-cultural faith. Patient and her family was clearly informed about the whole procedure and possibility of hymenal damage during the operation. Detailed written informed consent was obtained. Vaginoscopy, hysteroscopy and cystoscopy were planned.
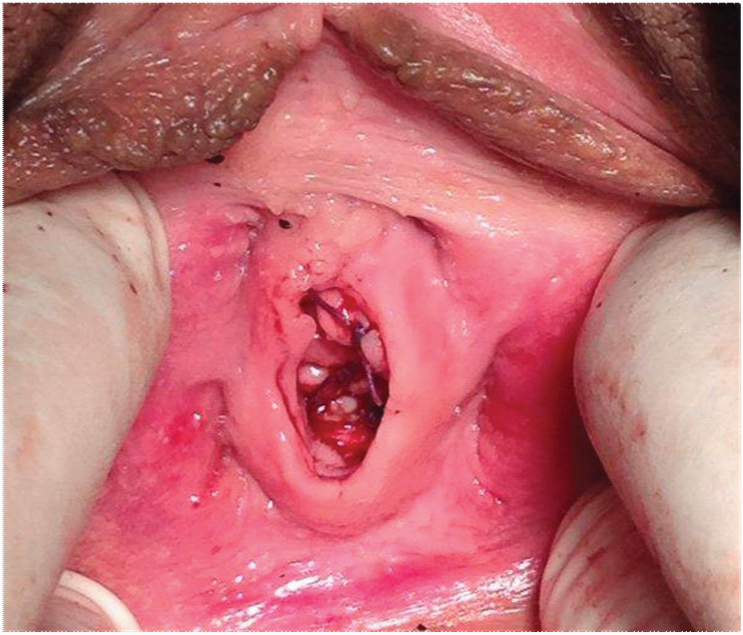
A single right ureteral orifice and otherwise normal bladder was observed on cystoscopy. Vaginoscopy revealed a bulging complete transverse vaginal septum extending from cervical ostiums to hymenal ring. Normal endometrial tissue and right tubal ostium of the right uterine horn was observed. Distal part of the septum was simply cut and suturedal lowing huge amount of menstrual blood to be drained. After irrigation, the left vagina and uterine horn was entered by hysteroscope. The tuba uterina of the left horn was dilated throughout its length. Cavity of the right uterine horn was normal and right cervix was effaced. Vaginal septum was completely incised by CO2 laser extending to the cervical ostiums while hymen was not injured [Table/Fig-2]. The patient had regular and painless menses and no distension was observed in her uterine horns and vagina twelve months postoperatively.
Preoperative Magnetic Resonance Imaging: a) Hematometrocolpos; b) Single right kidney
Introitus after the operation
Discussion
The true incidence of congenital uterine anomalies is difficult to determine. Mullerian malformations have an estimated incidence of 1,1-3,5% [1]. Basic classification of Mullerian duct defects consists of agenesis and hypoplasia, defects of lateral fusion, and defects of vertical fusion which have obstructed or non-obstructed patterns. OHVIRA has an incidence of 0.16–10% of these Mullerian duct anomalies [2,3].
Vertical fusion defects such as transverse vaginal septum can develop anywhere in the vagina. The septae commonly localized at the junction of the upper and middle third of vagina. Complete obstruction is a rare variant regarding to commonly septal fenestration [2,4]. Herein presented case, vaginal septum was non-fenestrated, starting form left cervical ostium, extending throughout whole vaginal length and ending at the level of hymen.
OHVIRA syndrome does not affect the external genitalia and does not produce symptoms in prepubescent children. Symptoms usually begin a few months after normal menarche which are dysmenorrhea, cyclic progressive abdominopelcvic pain and palpable pelvic mass due to blood collection in the obstructed hemivagina [2,4]. Haematometrocolpos can rarely be a cause of acute abdomen [5]. As the disease remains untreated, reversed menstruation and its secondary effects, such as endometriosis, pelvic adhesions, infertility and pelvic inflammatory disease may also develop [4]. Ultrasonography and Magnetic Resonance Imaging are main useful methods regarding to early diagnosos, to prevent chronic complications and planning surgery [3,6]. Magneting Resonance Imaging is superior to ultrasonography [7]. In the present case, the patient was 21-year-old at the time of diagnosis and had no history of infection or endometriosis.
The urinary and genital systems are derived from same ridge of mesoderm. Abnormal differentiation of the mesonephric and paramesonephric ducts can be accompanied by kidney and urinary tract anomalies [8]. The most common associated anomaly is renal agenesis. Renal ectopy, cystic renal dysplasia and duplicated collecting systems have all been described with genital tract anomalies [9,10]. Association between hemivagina and renal agenesis was seen in forty-one of forty-two patients in the study of Haddad et al., [11].
Many Mullerian duct anomalies do not require treatment. However, surgery is necessary for OHVIRA as soon as diagnosed in order to prevent long term complications (i.e. pyocolpos, chronic cryptomenorrhea). The surgical management of these cases involves drainage of fluid and resection of the vaginal septum with great care to avoid compromise to the bladder, rectum and the cervixes. The two cervixes may be at different levels and the tissue between them should be left in place so as not to compromise their blood supply.
In a study conducted by Williams et al., 46 cases who underwent transverse vaginal septum resection operations were analysed. 33% were managed via an abdominoperineal approach, 59% were managed via a vaginal approach, 6% had laparoscopic resection and one patient did not have surgery [12]. Majority of surgeons prefer to excise the vaginal septum in total then the normal vaginal mucosal edges from each vagina are sutured together over the defect while some others marsupialize the cut edges of the septum. Alternatively, primary drainage of the obstructed vagina by creating a window on the septum with a secondary surgery at a later time has also been performed [4].
The great concern must be the prevention of the common complications of the surgery of the transverse vaginal septum which include dyspareunia, Reobstruction and vaginal stenosis. One could argue that in these cases the extent of surgery might play a key role. For example, complete excision of the septal tissue may lead to circumferential scar formation and vaginal stenosis or a limited resection to create a window to drain the collected blood is more likely to be complicated by reobstruction. Herein the presented case, the primary concern was to preserve the future fertility potential and the integrity of the hymen of the patient so a minimally invasive approach was preferred; no hymenotomy was performed and the septum was not excised, instead was simply incised from the level of hymen throughout its length to the level of cervix endoscopically.
Conclusion
The diagnosis of OHVIRA should be suspected in menstruating women with cyclic pelvic pain, mass and unilateral renal agenesis. Surgery should be performed before complications arise. Integrity of the hymen can be preserved if it is of concern and simple vaginal incision may be a safe and effective approach in the treatment of the transverse vaginal septum cases.
[1]. Strassmann EO, Fertility and unification of double uterusFertil Steril 1965 17(2):165-76. [Google Scholar]
[2]. Vercellini P, Daguati R, Somigliana E, Asymmetric lateral distribution of obstructed hemivagina and renal agenesis in women with uterus didelphys: institutional case series and a systematic literature reviewFertil Steril 2007 87(4):719-24. [Google Scholar]
[3]. Cox D, Ching BH, Herlyn-Werner-Wunderlich syndrome: a rare presentation with pyocolposJ Radiol Case Rep 2012 6(3):9-15. [Google Scholar]
[4]. Jindal G, Kachhawa S, Meena GL, Dhakar G, Uterus didelphys with unilateral obstructed hemivagina with hematometrocolpos and hematosalpinx with ipsilateral renal agenesisJ Hum Reprod Sci 2009 2(2):87-89. [Google Scholar]
[5]. Aydin R, Ozdemir AZ, Ozturk B, Bilgici MC, Tosun M, A rare cause of acute abdominal pain: Herlyn-Werner-Wunderlich syndromePediatric emergency care 2014 30(1):40-42. [Google Scholar]
[6]. Mehra S, Chamaria K, Garga U, Kataria A, Ahuja A, Imaging Diagnosis of Herlyn-Werner-Wunderlich Syndrome-An Extremely Rare Urogenital AnomalyJ Clin Diagn Res 2015 9(5):6-8. [Google Scholar]
[7]. Troiano RN, McCarthy SM, Mullerian duct anomalies: imaging and clinical issuesRadiology 2004 233(1):19-34. [Google Scholar]
[8]. Walters Mark D, Karram Mickey M, Chapter 3, Embryology and congenital anomalies of the urinary tract, rectum, and female genitale systemUrogynecology and Reconstructive Pelvic Surgery 2015 4th edPhiladelphiaElsevier & Saunders:36-38. [Google Scholar]
[9]. Speroff L, Glass RH, Kase NG, Development of the mulleriansystem.: MitcellC, editorIn: Clinicalgynecologic endocrinology and infertility 1998 6th edBaltimore MdLippincott, Williams & Wilkins:124 [Google Scholar]
[10]. Fedele L, Bianchi S, Agnoli B, Tozzi L, Vignali M, Urinary tract anomalies associated with unicornuate uterusJ Urol 1996 155(3):847-48. [Google Scholar]
[11]. Haddad B, Barranger E, Paniel BJ, Blind hemivagina: long-term follow-up and reproductive performance in 42 casesHum Reprod 1999 14(8):1962-64. [Google Scholar]
[12]. Williams C, Nakhal R, Hall-Craggs M, Transverse vaginal septae: management and long-term outcomesBJOGPublished online: 19 2014;DOI: 10.1111/1471-0528.12899 [Google Scholar]