Gangrenous Cystitis in A Woman Following Vaginal Delivery: An Uncommon Occurrence - A Case Report
Rakhi Rai1, Pooja Sikka2, Neelam Aggarwal3, Sriharsha Ajjur Shankaregowda4
1 Research Officer, Department of Obstetrics and Gynaecology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
2 Assistant Professor, Department of Obstetrics and Gynaecology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
3 Associate Professor, Department of Obstetrics and Gynaecology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
4 Senior Resident, Department of Urology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rakhi Rai, House no 5817A, Sector 38 West, Chandigarh-160036, India.
E-mail: drrakhi81@yahoo.co.in
Gangrenous cystitis is now a rare condition with the advent of antibiotics and better obstetric services. It has a multifactorial causation manifesting as urosepsis or peritonitis. We report a case of 24-year-old lady who presented at day 12 postpartum with abdominal distension and vomitings. History of prolonged labour was present. Peritoneal tap was suggestive of pyoperitoneum. Hence she was taken up for emergency laparotomy and incidentally found to have bladder necrosis. Partial cystectomy was done and patient was discharged in a satisfactory condition after 2 weeks.
Antibiotic, Necrosis, Pyoperitoneum
Case Report
A 24-year-old para two presented to the Department of Obstetrics and Gynaecology, at day 12 postpartum with abdominal distension and vomitings. Her antenatal period was uneventful. She went into spontaneous labour at 38 weeks of gestation. She had a history of prolonged labour, more than 20 hours. There were no signs of obstructed labour and no history of any instrumentation. Baby was born with good apgar and both mother and baby were discharged next day. On day three, she developed pain lower abdomen but didn’t seek any medical help. On day nine postpartum, when she had multiple vomitings, she was referred to our hospital.
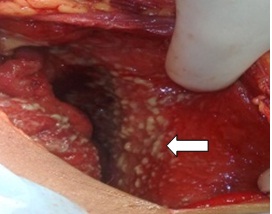
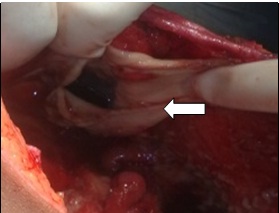
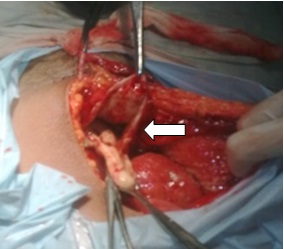
On examination, she was conscious, afebrile and haemodynamically stable. She had abdominal distension and absent bowel sounds. No abnormality was detected on per speculum or pervaginal examination. Perurethral catheter was inserted and slightly haemorrhagic urine was drained. Her haemoglobin was 10.8 gm/dl; total leucocyte count was 22500cumm with predominant neutrophils, platelet count of 5.25 lac & prothrombin index of 48%. Her renal function tests were deranged i.e. blood urea 137mg% & serum creatinine 2.2mg% and urine complete examination showed 15-20 pus cells. The blood and urine culture were sterile. Ultrasonography showed free fluid with internal echoes and septations in bilateral paracolic gutters and sub hepatic and left subdiaphragmatic area. Purulent fluid was aspirated on abdominal paracentesis. Intravenous antibiotics (piperacillin-tazobactum 2.25grams thrice a day & metronidazole 500mg thrice a day) were started. She received 3 doses of piperacillin-tazobactum and 2 doses of metronidazole prior to laparotomy. Four units of fresh frozen plasma were transfused. She was taken up for laparotomy in view of pyoperitoneum. Intraoperatively, 4 litres of serous fluid with pus flakes were drained [Table/Fig-1]. Intraoperative assistance of urologist was sought. Dome of bladder was necrotic and sloughed out including the posterior wall [Table/Fig-2,3]. Necrotic part of bladder was excised. Bladder was closed in 2 layers with vicryl 2-0 over suprapubic catheter & perurethral catheter. Pus cultures obtained showed bacterial growth of no significance. Histopathological examination showed acute inflammation of urinary bladder and inflammatory granulation tissue in the peritoneal biopsy. Postoperatively she recovered well. Her urine output was monitored both in suprapubic & perurethral catheter and was adequate. Her urine culture was done twice & was sterile. She was discharged in a satisfactory condition after 2 weeks.
Flakes covering peritoneal cavity
Defect at dome of bladder
Discussion
Due to antibiotic use in any intervention, gangrenous cystitis is now a very rare condition. It may vary from necrosis of mucosa to necrosis of entire bladder wall. The aetiology is usually multifactorial and identification of single particular cause is difficult [1]. Usually occurs in elderly, mainly affecting patients with co-morbidities like diabetes, spinal cord injuries, pelvic malignancies or stones [2]. Indexed patient was a young female without any co-morbidity. Causative agents include direct or indirect causes. Direct factors lead to direct damage to bladder wall like chemicals, radiation or widespread infection. Indirect factors interfere with blood supply leading to bladder ischemia & hence gangrene. Indirect causes include over distension of bladder secondary to chronic urinary retention, pressure of malpositioned pregnant uterus, prolonged labour, pelvic malignancies or blockage of arterial or venous channels by infection, emboli or thrombophlebitis [2,3]. Prolonged labour was the cause in the index case. It is now rare in obstetric cases due to better obstetric techniques and extensive antibiotic use. Stalin Viswanathan et al., [3] reported a case of emphysematous cystitis in a postpartum patient following a vaccum delivery and probable cause suspected was prolonged labour leading to neuropraxia of pelvic nerves, hypotonia of bladder, over distension and subsequent emphysematous cystitis. It doesn’t present with any specific symptoms [1]. Clinically it manifests as urosepsis or peritonitis. Presenting features include lower abdominal pain, Fever, dysuria, haematuria or pyuria. Pus or exfoliated debris in urine may block catheter leading to urinary retention [2,4]. Our patient presented with abdominal pain, distension and vomitings. A rare case of colovesical fistula due to gangrenous cystitis associated with vascular impairment and infection superimposed on urinary retention had been reported by A Raza et al., [5]. CT scan helps in making correct diagnosis [6]. Early aggressive treatment should be done. Multidisciplinary team approach involving a gynaecologist, urologist, surgeon and anaesthetist should be adopted. Conservative treatment in the form of appropriate antibiotic and adequate bladder drainage may be used in early stages [2]. Mostly requires surgical treatment in the form of debridement of necrotic nonviable bladder tissue, varying from partial to complete cystectomy depending upon the extent of degenerative process [1,2,6]. Emergency surgery is usually being undertaken without any predefined diagnosis [4]. Total cystectomy with ureteroneocystostomy was performed in a case reported by Bonera et al., [1]. In our case partial cystectomy excising necrotic tissue and repair was done. The high mortality rate is mainly due to delay in diagnosis because of nonspecific symptomatology, mixed infections with resistant strains and co-morbidities [2]. String and Hopkins reported 207 cases in their review, out of which 120 patients died, 80 recovered and in the rest outcome was indefinite [7]. Hence immediate and intensive treatment is a key to favourable outcome.
Conclusion
Laparotomy for puerperal sepsis has an added advantage of detecting uncommon occurrences like gangrenous cystitis which otherwise might go undetected. Intraoperative surgical repair of bladder with the help of urologist is associated with a favourable outcome.
[1]. Bonera A, Antoci G, Bianchi P, Alberti P, Gangrenous cystitisCase report Minerva Urol Nefrol 1996 48(4):193-97. [Google Scholar]
[2]. Hinev A, Anakievski D, Krasnaliev I, Gangrenous cystitis: report of a case and review of the literatureUrol Int 2010 85(4):479-81.doi: 10.1159/000321010 [Google Scholar]
[3]. Viswanathan S, Enterococcus faecium related emphysematous cystitis and bladder ruptureAustralas Med J 2012 5(11):581-84. [Google Scholar]
[4]. Charra B, Hachimi A, Sodki M, Gueddari H, Benslama A, Motaouakkil S, Urinary peritonitis caused by gangrenous cystitisSigna Vitae 2008 3(2):32-33. [Google Scholar]
[5]. Raza A, Balsitis M, Hosie K B, Gangrenous cystitis: a rare cause of colovesical fistulaPostgrad Med J 1999 75:34-35. [Google Scholar]
[6]. Sataa S, Habiba M, Emna M, Urinary peritonitis caused by gangrenous cystitisLa tunisie Medicale 2013 91(12):736-37. [Google Scholar]
[7]. String WC, Hopkins GA, Gangrene of the bladderJ Urol 1933 31:517-25. [Google Scholar]