Emergency cases are not frequent in urology specialty compared to other surgical fields, yet they pose a challenge as and when they are faced [1]. However, emergency cases constitute a sizeable proportion of urology cases at our tertiary care institution. Urological cross references from other departments of the institute further increases the emergency case load. The common presentation of emergency urology cases is retention of urine [2] but their lie geographic variations in the distribution of urological emergencies and hence the present study was undertaken to analyse the different urological presentations of emergency cases and their necessary interventions.
1) To estimate the proportion of urological emergencies out of all emergencies reported at the center.
2) To describe the different types of urological emergencies reported and their required management.
Materials and Methods
This hospital based observational descriptive study was done in the Department of Urology, SMS Hospital Jaipur. This hospital is the largest tertiary referral center in the state with wide catchment area. There were 35,35,639 Outpatient Department (OPD), 3,31,931 Inpatient Department (IPD), nearly 4,36,220 emergency IPD patients and 2,86,433 number of operations done at this centre in the year 2013.
Although being a tertiary referral teaching hospital, direct urological emergency admissions are also entertained on regular basis. The number of emergency admissions are out of proportion of available beds. So it is the true reflection of urological emergencies which are being faced by physicians on regular basis.
Total 2,345 urological emergencies that reported directly to emergency department and 5310 emergency referral within hospital for urological cross consultations were considered for the study. Patient data enlisting age, sex, referral status, clinical presentation, duration of hospital stay and management provided were collected from patient records on Arogya online registered referral system. This is an advanced hospital management system connected to mobile network of doctors and staff for faster communication and timely care of patients. It also facilitates maintenance of patient records for future references and data analysis [Table/Fig-1a & b].
Arogya online registered referral system connected to mobile network
Sample size: A sample of 2345 urological emergency cases is required at 95% confidence interval and 15% relative error to verify the minimum 7% proportion of different types of urological emergencies (ranges 7 to 73%) [3].
Sampling procedure: We scrutinized consecutive 39,994 emergency case records from August 2013 to September 2014 to obtain 2345 urology emergency cases. All 5310 urological cross referral cases reported during this period were also analysed for the study.
Results
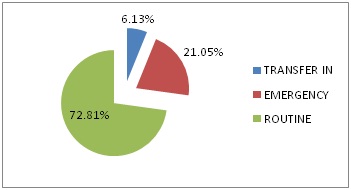
Urology cases constituted 5.84% (2345/39,994) of all surgical emergency admissions [Table/Fig-2]. Total 11,139 cases were admitted in the urology department during the study period, of which 8111 (72.8%) were routine outpatient department (OPD) admissions, 2345 (21.05%) were emergency admissions and 683 (6.13%) were transferred cases from other departments [Table/Fig-3]. Thus, emergency workload in urology department constituted 27.18% of total admissions.
Distribution of surgical cases admission in routine and emergency OPD
| Surgical department | Routine OPD admissions | %of total admissions | Emergency admissions | % of total emergency admission |
|---|
| Surgery | 18624 | 39.61% | 13673 | 34.1% |
| Neurosurgery | 3889 | 8.27 | 11128 | 27.82% |
| Orthopaedic | 8412 | 17.89 | 5866 | 14.6% |
| Cardiothoracic | 2669 | 5.67 | 4080 | 10.2% |
| Plastic surgery | 5309 | 11.29 | 2902 | 7.2% |
| Urology | 8111 | 17.25 | 2345 | 5.84% |
| Total | 47014 | | 39994 | |
Distribution of cases of Department of Urology
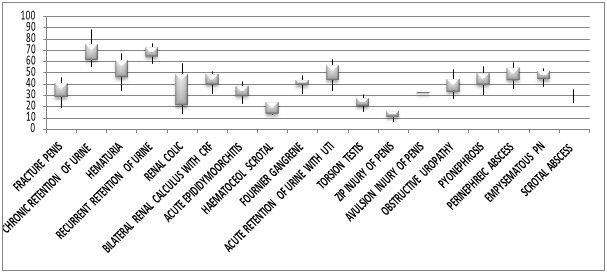
The age profile range of directly admitted emergency cases is as shown in [Table/Fig-4].
A “BOX & WHISKER” plot for Age profile of directly admitted emergency cases
The commonest presentation of emergency urology patients was renal colic (24.2%) followed by acute retention of urine (14.7%), obstructive uropathy (14.7%), haematuria (9.9%), Lower Urinary Tract Symptoms (LUTS) with Urinary Tract Infection (UTI) (9.8%) [Table/Fig-5].
Clinical Presentation of Emergency urology cases
| Presentations in emergency | No. of cases | % of total cases |
|---|
| Renal colic | 567 | 24.17 |
| Acute retention of urine | 330 | 14.71 |
| Obstructive uropathy | 344 | 14.66 |
| Haematuria | 231 | 9.85 |
| Lower urinary tract symptoms with UTI | 230 | 9.8 |
| Bilateral renal calculus with CRF | 128 | 5.45 |
| Pyonephrosis | 128 | 5.45 |
| Others | 387 | 16.50 |
Majority (22.59%, 1200/5310), of the references came from the Department of Medicine, followed by common poly-trauma unit (20.65 %), Nephrology (17.5%) and Surgery (13.7%). References from other departments including cardiology, neurosurgery, obstetrics & gynecology, rehabilitation centre were collectively 25.6% [Table/Fig-6], On an average there were 14 (14.54 +2.46) urological cross referrals per day from other departments. Haematuria was the leading presentation (17.75%) among the referred cases followed by traumatic catheterization (11.97%), LUTS with UTI (10.05%), Pelvis Fracture Urethral Distraction Defect (PFUDD) (9.15%) [Table/Fig-7].
Department wise Distribution of urological references for cross consultations
| Distribution of department | No. ofreferences(n-5310) | % of all references |
|---|
| Medicine | 1200 | 22.59 |
| Common polytrauma unit | 1097 | 20.65 |
| Nephrology | 933 | 17.57 |
| Surgery | 729 | 13.7 |
| Others departments | 1351 | 25.44% |
Profile of urological references for cross consultations
| Presentations of urological references | No. ofreferences(n-5310) | % of all references |
|---|
| Haematuria | 943 | 17.75 |
| Traumatic catheterisation | 636 | 11.97 |
| Lower urinary tract symptoms with UTI | 534 | 10.05 |
| Fracture pelvis with urethral injury | 486 | 9.15 |
| Retention of urine with difficult catheterisation | 445 | 8.38 |
| Obstructive uropathy | 356 | 6.7 |
| Paraphimosis | 331 | 6.23 |
| Pyonephrosis | 273 | 5.14 |
| Renal abscess | 256 | 4.82 |
| Neurogenic bladder | 245 | 4.61 |
| Renal trauma | 236 | 4.44 |
| Others | 569 | 10.71 |
Out of total 356 cases of obstructive uropathy, 224 cases presented as anuria and 132 cases as bilateral renal calculus with CRF. Out of total 224 anuric cases, 148 cases were of bilateral ureteric calculus and 76 cases were of solitary functioning unit of kidney with ureteric calculus.
No specific aetiology was found in 27.14% of haematuric cases but radiation cystitis (19.4%), bleeding disorder (13.89%), benign prostatic hyperplasia (10.07%) were probable causes among them. Almost half of renal trauma cases are of grade I and quarter of grade II. Out of 1097 patients referred from common polytrauma unit, 106 had bladder rupture, of them 71.7% were extra peritoneal and 28.3% were intra peritoneal. Eight of them had unilateral and two had bilateral ureteric injury also along with bladder trauma. Ninety cases had associated fracture of pelvis too.
There were 73 calls for intra operative consultation for bladder and ureteric injury, most of them occurred during abdominal hysterectomy done for postpartum haemorrhage (22), endometriosis (21), during caesarian section (19) and radical hysterectomy (11).
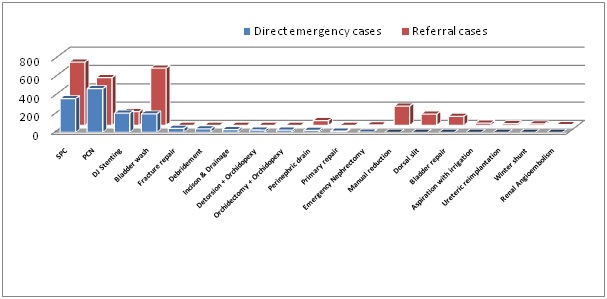
The common procedures (in decreasing order of frequency) required for emergency urological patients were Percutaneous Nephrostomy (PCN), Supra Pubic Catheterization (SPC), DJ stenting [Table/Fig-8] while the common procedures required for within hospital urological cross consultation were supra-pubic catheterization, bladder wash, per-cutaneous nephrostomy (decreasing order of frequency) [Table/Fig-8].
Urological interventions in emergency admitted (1448) and cross referral cases (2536)
*SPC-supra pubic catherisation & PCN -percutaneous nephrostomy
Discussion
The observation of 3,333 surgical emergency cases reported per month in our study is much higher than 400 surgical emergency admissions per month observed by Sharma RK et al., [2]. Similarly 3028 (2345 + 683) urological emergency cases observed in our study is much higher than Fall B et al., (1237 cases at Dakar university), Sharma RK et al., (78 cases) and Bobo Diallo A et al., (757) cases, Martin L et al., (1257 cases) and Moby MH et al., (291 cases) [2–6] [Table/Fig-9].
Comparative data of present study and previous similar studies
| Study | Durati-on | No. of patient | Mean age | Sex ratio | % of total admissi-on | Major Non-traumaticinjury | Majortraumatic injury | MajorIntervention |
|---|
| Martin L et al., [5] (2014) | One year | 1257 | 57±22 years | 73.3% male | - | Retention of urine | Scrotal injury | PUC/ SPC* |
| Moby MH et al., [6] (2012) | Three years | 291 | 42.5 years | - | - | - | Scrotal injury | Exploration and suturing wounds |
| Bobo Diallo A et al., [3] (2010) | Three years | 757 | 56 years | 16.60 | 22 % | Retention of urine | Urethral injury | PUC* |
| Fall B et al., [4] (2008) | 20 months | 1237 | 58.8 years | 20.32 | - | Retention of urine | - | SPC* |
| Mondet F et al., [7] (2002) | One year | 1715 | 53.18 years | 3.54 | 15.6% | Renal colic | Renal/ peno-scrotal trauma | PUC/SPC* |
| Parra Muntaner L et al., [8] (2001) | One year | 1504 | 53 years | 1.25 | - | Renal Colic | - | - |
| Sharma R.K et al., [2] (1987) | One month | 78 | - | - | 18.25 % | Retention of urine | - | - |
| Present study | One year | 3028 | - | - | 27.18 % | Renal Colic | Traumatic catheteriz-ation | SPC/PCN* |
*(PUC-per urethral catheterization, SPC-suprapubic catheterization, PCN-percutaneous nephrostomy)
Renal colic (24.2%), the most common emergency presentation of our study is comparable (44.54%) to Parra Muntaner L et al., and Mondet F et al., studies. [7,8] Renal colic was observed in 77.5% ureteric calculus in our study while Sharma et al., reported only 14.66% renal colic cases in their study [2].
The most common cause of acute retention of urine in our study was stricture urethra and of chronic urinary retention was benign prostatic obstruction followed by neurogenic bladder whereas Fall B et al., and Bobo Diallo A et al., reported prostatic tumors and urethral strictures as main causes in their study [3,4]. A comparable finding of 20.55% cases of urinary retention associated with spinal cord injury and 17.81% due to prostatomegaly/stricture was observed by Sharma et al., [2]. Haematuria cases contributed 9.9% of emergency admissions in our study compared to 9.6 % & 10.6% in the studies done by Sharma et al., and Bobo Diallo A et al., respectively [2,3].
Genitourinary trauma cases didn’t directly present to our urology department rather they were mostly referred cases. Traumatic catheterization (11.97%), fracture pelvis with urethral injury (9.15%), renal trauma (4.44%) were major cross reference emergencies whereas torsion testis (2.04%), fracture penis (1.19%), zipper (lacerated) and avulsion injury of penis were direct emergency urological presentations in our study. Similarly urogenital traumas were the most frequent traumatic cases in Fall B [4] and Bobo Diallo [3] studies. Circumcision accidents were also common in their area. Early referral to specialized departments and prompt management by the specific unit reduces the average length of stay of patients in hospital and total hospitalization charges, and also alleviates the agony, misery and despondency of patient’s family and relatives [2].
Due to large number of intra hospital referrals average time to reach the Department of Urology by patients was considerably more. With the use of Aarogya online referral system, this time was considerably reduced with added advantages of having patient details registered in the system, records maintained for future reference and an online track service utilized by other departments also. With the application of this technology for within hospital referrals, manpower use reduced considerably and thus it served as a step in fostering health service reforms.
Supra pubic catheterization was required in 1058 cases in our study whereas it was required in 59.8% cases in Fall B et al., study [4] and in 24.14% cases in Bobo Diallo A et al., study [3]. Per urethral catheterization (55.25%) was the most common intervention reported by Bobo Diallo A et al., [3]. Emergency percutaneous nephrostomy were performed in 997 cases, mostly for obstructive uropathy and pyonephrosis at our institute. Topographic location of our hospital brings it under the stone belt of India hence renal colic was the leading emergency urological presentation (24.2%) in our study.
Limitations
The present study had certain limitations. This study is a single centre study and seasonal variations in the presentation of urological emergencies had not been studied. We need to conduct similar studies across different parts of India for better understanding of geographic distribution of urological ailments and their changing patterns in terms of demographic and epidemiological variables.
Conclusion
Urological emergencies constitute around 6% of total surgical emergency admissions and around 27% of all urology admissions in this tertiary care institute. The most common non-traumatic presentation was renal colic whereas traumatic presentation was traumatic catheterization in our study. Most common surgical intervention needed in directly admitted emergency cases was percutaneous nephrostomy whereas it was suprapubic catherisation within hospital emergency referral cases. Present study highlights the data of within hospital cross referred patients also, which is the first contemplation of its kind to the best of our knowledge. This study also highlights data of intraoperative consultation for urological expertise which was not incorporated in previous studies.
*(PUC-per urethral catheterization, SPC-suprapubic catheterization, PCN-percutaneous nephrostomy)