Phenytoin Induced Osteopathy -Too Common to be Neglected
Milind Machhindra Patil1, Jayaprakash Sahoo2, Sadishkumar Kamalanathan3, Vivekanandan Pillai4
1 Senior Resident, Department of Endocrinology & Metabolism, JIPMER, Pondicherry, India.
2 Assistant Professor, Department of Endocrinology & Metabolism, JIPMER, Pondicherry, India.
3 Associate Professor, Department of Endocrinology & Metabolism, JIPMER, Pondicherry, India.
4 Additional Professor and Head, Department of Endocrinology & Metabolism, JIPMERPondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Milind Machhindra Patil, 2nd Floor, 1st Building, Opposite Senthatamizh Tirumana Nilayam, Amritha Nagar, Thattanchavadi, Pondicherry-605006, India. E-mail : milindpmed@gmail.com
Anticonvulsants have the broad spectrum of side effects on the bone that are collectively known as osteopathy. Anticonvulsant induced osteopathy can have detrimental consequences. We present an unusual case that uniquely highlights both adverse effects of phenytoin on bone metabolism and side effects of its overtreatment.
A 29-year-old lady came for evaluation of metabolic bone disease. Since last one year, she had severe bilateral hip pain resulting in restriction of movements. She was taking phenytoin 300 mg daily for last ten years for a seizure disorder. During evaluation at another center, she was diagnosed to have vitamin D deficiency, osteomalacia and secondary hyperparathyroidism. She received recombinant parathormone, high doses of vitamin D along with phenytoin. She presented at our centre with persistent pain and hypervitaminosis D. We stopped recombinant PTH, vitamin D and changed phenytoin to levetiracetam. Her condition improved over next six months with normalization of vitamin D. Thus, patients on phenytoin should be actively screened for side effects and the appropriate preventive and correctional measures should be undertaken. While managing these side effects overtreatment should be avoided.
Anticonvulsants, Osteomalacia, Osteoporosis, Vitamin D
Case Report
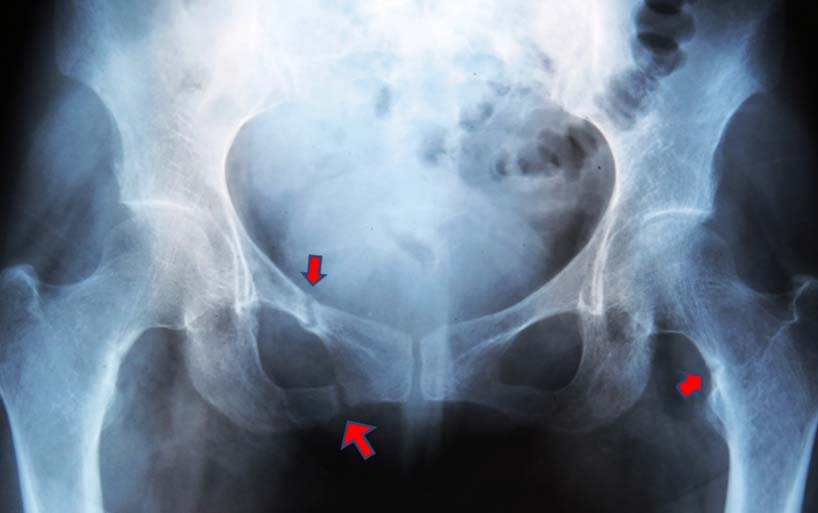
A 29-year-old female was referred for evaluation of metabolic bone disease. She was a known case of seizure disorder for which she was taking phenytoin 100mg three times a day for last ten years. Since last one year, she had bilateral hip pain that started insidiously and gradually progressed to such an extent that she had difficulty while walking. She denied any history of trauma, fractures, or steroid use. She was a non-smoker and non-alcoholic. First she consulted at another center where she found to have vitamin D deficiency, secondary hyperparathyroidism [Table/Fig-1]. The x-ray of the hip joint showed features suggestive of osteomalacia with pseudo-fractures [Table/Fig-2a]. Dual energy X-ray absorptiometry (DEXA) scan showed osteoporosis with total hip Z-score: -2.7 and Spine Z-score: -3.4. She was treated with vitamin D (6 lacs IU) every weekly for three months. Also, she received elemental calcium 1000 mg orally and recombinant PTH 20 microgram/day subcutaneously daily for the three months. She continued phenytoin. Due to the persistence of symptoms she consulted at our centre. She had hypervitaminosis D, mild hypercalcaemia and hypercalciuria at presentation [Table/Fig-1]. However, she was not having other symptoms of hypervitaminosis D like polyuria, polydipsia, nausea, vomiting, anorexia, constipation, headache, and the altered neurological status.
Showing the investigations done at various centre
| Investigations (normal range) | At outside centre | At our centre* | Follow up at our centre ** |
|---|
| Calcium (2.2-2.6 ukat/L) | 2.35 mmol/L | 2.85 mmol/L | 2.40 mmol/L |
| Phosphorus (0.81-1.4mmol/L) | 0.97 mmol/L | 0.80 mmol/L | 0.81 mmol/L |
| Alkaline phosphatase (0.67-2.51 ukat/L) | 2.75 ukat/L | 1.44 ukat/L | 1.50 mmol/L |
| 25-hydroxy Vitamin D (75-250 nmol/L) | 41.93 nmol/L | 936 nmol/L | 131.2 nmol/L |
| PTH (8-51ng/L) | 104.6 ng/L | 15.30 ng/L | 20 ng/L |
| Urinary Ca/Cr ratio (<0.20) | - | 0.233 | 0.13 |
*3 months later than evaluation done at outside centre
**6 months later than first evaluation done at our centre
X-ray showing pseudofracture as marked by arrow
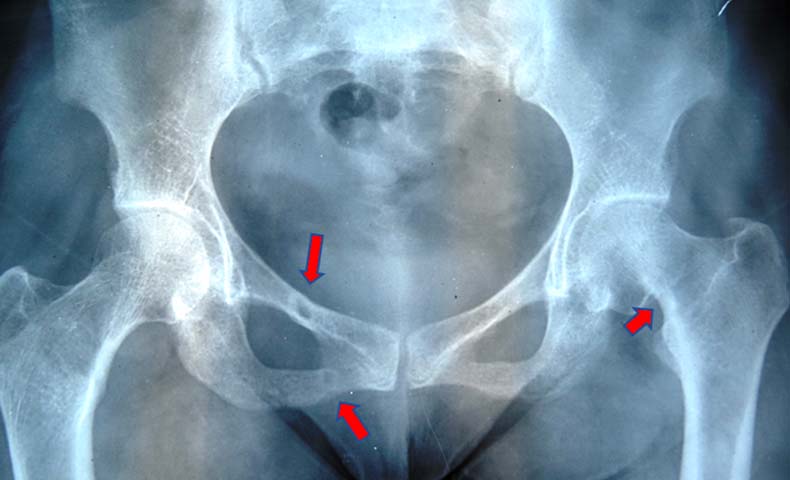
X-ray showing healed pseudofracture as marked by arrow
On examination, her height and weight were 148cm and 43kg respectively with BMI of 19.63kg/m2. Her general and systemic examinations were normal except for the pain on compression of the hip joint.
We replaced phenytoin with levetiracetam that is not having side effects on bone. Additionally, Vitamin D/calcium supplementation and recombinant PTH were stopped. Over a period of next three months, the pain subsided with healing of pseudo-fracture [Table/Fig-2b]. Her vitamin D normalized over period of six months.
Discussion
Patients with epilepsy receive anticonvulsants for the prolonged duration making them vulnerable to deleterious consequences of osteopathy. Osteopathy includes either of osteoporosis, osteomalacia, mixed forms or bone loss without evidence of vitamin D deficiency. On the average, 50% of patients receiving anticonvulsants (range 4-70% in different studies) have osteopathy. It affects patients of both genders and all age groups. Besides, anticonvulsants have been identified as an independent risk factor for low bone density and osteoporosis [1]. All these factors contribute to increased risk of fractures in these patients.
The primary proposed mechanisms for anticonvulsant induced osteopathy are development of vitamin D deficiency, hypocalcaemia and secondary hyperparathyroidism. Other mechanisms include a direct effect on bone cells, sex steroids and vitamin K [2].
Enzyme inducing drugs causes increased expression of cytochrome P24 that inactivates 25 hydroxy vitamin D into inactive calcitriol acid. Resulting vitamin D deficiency leads to hypocalcaemia, hypophosphatemia, secondary hyperparathyroidism all of which contribute to increased bone loss. Phenytoin, also, directly decreases calcium absorption leading to hypocalcaemia. It also causes vitamin K deficiency. Vitamin K deficiency can potentially cause bone loss by preventing the post-translational modification of the vitamin K-dependent matrix proteins. Phenytoin and carbamazepine inhibit osteoblast while valproic acid activates osteoclast leading to bone loss [3,4]. Enzyme inducing anticonvulsants like phenytoin and carbamazepine decrease levels of free androgens by increasing the clearance of androgen as well as increasing sex hormone binding globulin levels [2].
Thus, both enzyme-inducing antiepileptics like phenytoin, carbamazepine and phenobarbital as well as enzyme inhibiting anticonvulsant like valproic acid can cause osteopathy. The data regarding newer anticonvulsants is limited but short duration study with levetiracetam has found no effect on bone metabolism [5].
Since most of the early symptoms are non-specific, many cases are left undiagnosed till they present with severe phenotype as seen in our case. A presence of bone pains, fractures after minimal trauma, muscle weakness, or worsening of seizures control should be considered seriously as a clinical marker of severe osteopathy. If any of these red flag signs are present patient should be evaluated in detail and treated aggressively.
Most of the recommendations for management are empirical in the absence of long-term trials evaluating different therapeutic options. In general, all patients should undergo baseline evaluation of serum calcium, albumin, phosphate, alkaline phosphatase, PTH and 25-OH vitamin D levels. DEXA scan should be performed at baseline in high-risk patient and after five years in minimal risk patients. Patients should be advised to adopt good bone health practices that include regular weight-bearing exercise, adequate sunlight exposure, adequate intake of calcium/vitamin D and avoidance of smoking and alcohol use [2]. Bisphosphonates may be considered for adults with significant osteopenia or osteoporosis although there are no established data for its use in anticonvulsants induced bone loss specifically.
Patients on long-term anticonvulsants should be given at least two to three times more vitamin D for their age group as a preventive measure. For management of vitamin D deficiency, a higher dose equivalent to 6000–10,000 IU/d of vitamin D followed by maintenance therapy of 3000–6000 IU/d should be given [6]. Our patient received vitamin D in large excess of suggested dose which resulted in hypervitaminosis D. Hypervitaminosis D is defined as 25 OH Vitamin D levels more than 250 nmol/l. It presents with symptoms of hypercalcaemia like anorexia, constipation, nausea, vomiting, polyuria. Other symptoms include bone pain, drowsiness, continuous headaches, irregular heartbeat, loss of appetite, muscle and joint pain. Our patient had only mild hypercalcaemia and calciuria despite elevated vitamin D levels [7]. We speculate that withholding vitamin D and Calcium might have prevented the further complications.
Thus, we present a unique case where the patient suffered morbidity due to both lacks of appropriate preventive measures and lack of proper management.
Use of anticonvulsants for the prolonged duration is a known risk factor for increased bone loss and fracture since long time [8]. This risk increases with dose and duration of treatment. Many physicians are unaware of this risk as shown in the survey by Valmadrid et al., [9]. Besides, the guidelines addressing this issue are lacking. The prevalence of the epileptic disorder in Indian population is estimated to be 5.5 per 1000 population [10]. Thus, a large number of the patients are at increased risk of osteopathy. In addition, the management of fractures is very expensive as compared to simple preventive measures especially in Indian setup. Our case report highlights need to raise awareness among physician toward this common but often neglected side effect.
Conclusion
Thus we report a common side effect of phenytoin i.e. osteopathy that was neglected. Our case also highlights the important issue of its prevention and management.
*3 months later than evaluation done at outside centre
**6 months later than first evaluation done at our centre
[1]. Bartl R, Antiepileptic drug-induced osteopathy. Subtypes, pathogenesis, prevention, early diagnosis and treatmentDtsch Med Wochenschr 2007 132(27):1475-79. [Google Scholar]
[2]. Valsamis HA, Arora SK, Labban B, McFarlane SI, Antiepileptic drugs and bone metabolismNutr Metab 2006 3:36 [Google Scholar]
[3]. Sheth RD, Wesolowski CA, Jacob JC, Penney S, Hobbs GR, Riggs JE, Effect of carbamazepine and valproate on bone mineral densityJ Pediatr 1995 127(2):256-62. [Google Scholar]
[4]. Feldkamp J, Becker A, Witte OW, Scharff D, Scherbaum WA, Long-term anticonvulsant therapy leads to low bone mineral density–evidence for direct drug effects of phenytoin and carbamazepine on human osteoblast-like cellsExp Clin Endocrinol Diabetes Off J Ger Soc Endocrinol Ger Diabetes Assoc 2000 108(1):37-43. [Google Scholar]
[5]. Koo DL, Joo EY, Kim D, Hong SB, Effects of levetiracetam as a monotherapy on bone mineral density and biochemical markers of bone metabolism in patients with epilepsyEpilepsy Res 2013 104(1-2):134-39. [Google Scholar]
[6]. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guidelineJ Clin Endocrinol Metab 2011 96(7):1911-30. [Google Scholar]
[7]. Alshahrani F, Aljohani N, Vitamin D: Deficiency, Sufficiency and ToxicityNutrients 2013 5(9):3605-16. [Google Scholar]
[8]. Kruse R, Osteopathies in antiepileptic long-term therapy (preliminary report)Monatsschrift Für Kinderheilkd 1968 116(6):378-81. [Google Scholar]
[9]. Valmadrid C, Voorhees C, Litt B, Schneyer CR, Practice patterns of neurologists regarding bone and mineral effects of antiepileptic drug therapyArch Neurol 2001 58(9):1369-74. [Google Scholar]
[10]. Sridharan R, Murthy BN, Prevalence and pattern of epilepsy in IndiaEpilepsia 1999 40(5):631-36. [Google Scholar]