Small bowel volvulus is a rare and life threatening surgical emergency. Nearly 75% of volvulus occurs in colon and 25% occurs in small bowel. Small bowel volvulus is abnormal twisting of bowel loops around the axis of its own mesentry leading to twisting and occlusion of mesenteric vessels causing intestinal obstruction, venous engorgement, gangrene and perforation. Small bowel volvulus is more common in neonates and young adults and very rare in adults. We are reporting a first case of small bowel volvulus and gangrene caused by herniation of ovarian cyst through mesenteric defect and twisting of small bowel around the axis of ovarian cyst leading to closed loop obstruction, small bowel volvulus and gangrene. Outcome of the disease is mainly based on the early diagnosis and intervention. Mortality is about 5.8 - 8% in nongangrenous SBV which increases drastically to 20 – 100% in gangrenous bowel.
Gangrene bowel, Internal hernia, Meckels diverticulum, Mesenteric defect, Ovarian cyst
Case Report
A 45-year-old female patient presented to our emergency department with complaints of central abdominal pain, vomiting for 3 days, fever and constipation for one day and amenorrhea for 4 months. No history of previous surgery and trauma. On examination patient showed tachycardia, increased sweating and anxious look. Abdomen was distended with severe tenderness, guarding and absent bowel sounds.
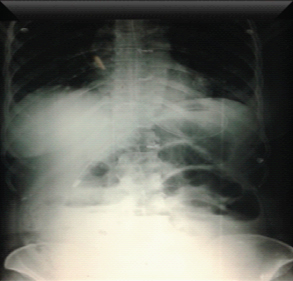
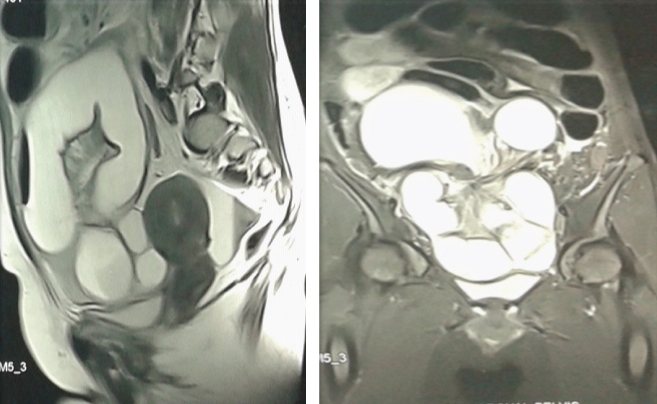
X ray abdomen on erect posture showed dilated small bowel [Table/Fig-1] and MRI showed large cystic lesion in the pelvis and right iliac fossa with grossly distended intestinal loops suggestive of small bowel obstruction secondary to cecal volvulus [Table/Fig-2a,b].
X ray showed dilated small bowel
MRI showed whirl sign with distended intestinal loops with cystic lesion? caecal volvulus
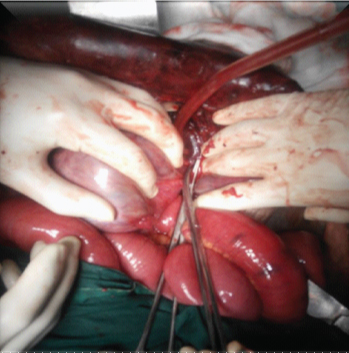
Immediate laparotomy was performed. Intraoperatively, dilated gangrenous distal ileum with meckel diverticulum [Table/Fig-3] was found twisted around the root of right ovarian cyst of size about 10 x 9 cm with adhesions between them [Table/Fig-4]. After adhesiolysis, there was a mesenteric defect noted in the volvulated bowel in the volvulus bowel of about 20 x10 cm through which ovarian cyst herniated [Table/Fig-5].
Gangrenous meckel’s diverticulum

Adhesion between ovary and bowel
Volvulated loop with mesenteric defect

The patient also had left small ovarian cyst with fibroid uterus for which total abdominal hysterectomy and bilateral salphingooopherectomy followed by Resection of gangrenous bowel [Table/Fig-6] and anastomosis was done.

Postoperatively patient was diagnosed to be hyperthyroid and she was treated with anti thyroid drugs and patient recovered without any complications.
Discussion
Small bowel volvulus represents less the 5% of all intestinal obstruction. Small bowel volvulus represents 25% of small intestinal obstructions [1]. Small bowel volvulus is a rare and life threatening surgical emergency [2]. Nearly 75 % of volvulus occur in colon and 25% occurs in small bowel [3]. Small bowel volvulus is abnormal twisting of bowel loops around the axis of its own mesentry leading to twisting and occlusion of mesenteric vessels causing intestinal obstruction, venous engorgement, gangrene and perforation [1,2]. Small bowel volvulus is more common in neonates and young adults and very rare in adults [4]. Epidemiologically it is common in Africa, middle-east Asia and India with incidence of about 24-60 cases per one lac population with repect to 1.7-5.7 cases/1 lac in North America and western Europe [1]. It is common in Muslims during the month of Ramzan alleged due to prolonged fasting followed by high fibre diet. It has seasonal incidence in rural Nepal during the month filled with festivals and feasts [5,6].
Small bowel volvulus is divided into primary and secondary based on its aetiology [2]. Small bowel volvulus is said to be primary (48%) primary if no predisposing anatomical cause found. Secondary small bowel volvulus may either be due to congenital anomalies or acquired [2]. Primary small bowel volvulus is mainly due to long small bowel, broad fat free mesentry with narrow base [5], increased gut motility [5]. The widely accepted mechanism is sudden transfer of bulky food into jejunum which makes the heavier bowel loops to fall over to the left lower quadrant which has less resistance. Peristalsis causes the empty loops of proximal jejunum and ileum to rotate clockwise in right lower quadrant causing torsion of mesentery [6]. Heavy musculature is also seen as important cause for primary small bowel volvulus as it is commonly seen in young adults [6,7].
Secondary small bowel volvulus is common in 6th to 8th decade and very rare before 40 years [7]. Various pathologies have been documented in the literature as the reasons for secondary small bowel volvulus which occurs following an anatomical cause which may be due to congenital anomalies such as malrotaion of midgut [8], chylolymphatic mesenteric cyst [2], intestinal duplication [8], ovarian cyst [9], meconium pseudocyst [10], congenital mesenteric defect [10], meckels diverticulum, ileal atresia, meconium ileus [4], jejunal diverticulum [11], persistant omphalocele cyst [2] and acquired causes such as adhesions, bands [11], mesenteric cyst [2], ascariasis [2,4], tumours [2], leiomyoma [4], internal hernia such as paraduodenal hernia [4], in pregnancy during third trimester [1,4], ovarian cyst as in our case [9,12], enteroenterostomy [4], simultaneous pancreas and kidney transplantation [4], laparoscopic appendicectomy due to pneumoperitoneum, bowel handling, patient positioning, anaesthesia drugs causing intestinal bloating and fast decompression [4].
Gynaecological pathology presenting with abdominal signs is about 1.5% in outpatients and 5% in emergency department [9]. Intestinal obstruction complicating ovarian cyst is rare and usually seen in neonates (3%) with about 19 cases has been so far reported [9,12] and 2 reported cases in adults [9,12]. Intestinal complications mainly occurs when the size of the ovarian cyst is more than 10cm which requires emergent surgery [9]. Two mechanisms have been proposed as the cause for intestinal complications, first, adhesions causing torsion and second due to pressure effects of huge cyst [9,12]. Intestinal obstruction following internal hernia is 0.2-0.9% of which paraduodenal hernia is the commest (50%). Internal hernia through congential mesenteric defect is commonly seen in children and rare seen in adults which occurs mostly secondary to trauma and surgery. Zia Ur Rahman et al., and Avjith Roy et al., reported cases of internal herniation of bowel loops through mesenteric defect [13,14].
Ali duran et al., reported a case of giant ovarian cyst compressing small intestine leading to gangrene [9]. Ahmet Akin Sivaslioglu et al., presented a rare case of torsion ovarian cyst with ileal gangrene due to pushing and twisting of mesenteric vessels [12].
We are reporting the first case of small bowel volvulus and gangrene caused by herniation of ovarian cyst through mesenteric defect and twisting of small bowel around the axis of ovarian cyst leading to closed loop obstruction, small bowel volvulus, gangrene with incidental meckel diverticulum and hyperthyroidism (increased gut motility).
Clinically patient presents with periumbilical pain which doesn’t subside with analgesics and associated nausea (83%), vomiting (100%) and abdominal distension (55%) and peritonism (14-26%). Fever, tachycardia and peritonism present in 90% of gangrene bowel cases which needs immediate surgical intervention. Haematologically total count will be more than 18000 cells/cubic mm, increased amylase, lactate levels (55%) and metabolic acidosis (25%). There is no haematological investigation to differentiate gangrene and non gangrene bowel [5].
On Imaging studies, Doppler ultrasound shows the classical sign ‘whirlpool sign’ first described by Parcos et al., due to inversion of superior mesenteric vein and artery with 89-100% sensitivity [2]. The pathognomic whirl pool sign represents twisted pedicle, dilated intestinal loops around central axis formed of mesentry and superior mesenteric artery and vein twisted around them causing mechanical obstruction with secondary venous engorgement of the intestine [15]. Absence of the sign doesn’t rule out small bowel volvulus [8].
Computer tomography is the investigation of choice and its sensitivity depends on the length and orientation of the loop in relation to the imaging plane. On CT, ‘C’, ‘U’ shaped loops of bowel [3,5,6], radially arranged distented bowel loops around the mesenteric vessels, two adjacent collapsed small bowel segments and small bowel feces sign which is gas or solid material within the dilated bowel loop [3]. Bowel wall thickening, mesenteric oedema, pneumatosis, gas in portal vein and ascites are sign of ischemia [3,5]. Upper gastrointestinal barium series is the investigation of choice in malrotation of gut [8] which shows corkscrew and spiral path [5]. Angiography shows barber pole sign [5]. CT and MRI shows whirl sign, peacock sign [5]. Outcome of the disease is mainly based on the early diagnosis and intervention. Mortality is about 5.8-8% in nongangrenous small bowel volvulus which increases drastically to 20-100% in gangrenous bowel. Early diagnosis and intervention by laparotomy is the utmost important in small bowel volvulus to avoid gangrene leading to postoperative short bowel syndrome [4,5].
Conclusion
Small bowel volvulus occurs due to various pathologies as mentioned above and its outcome mainly depends on the early diagnosis and intervention as mortality increases significantly in the setting of gangrene. Doppler ultrasound show pathognomic whirlpool sign and CT is the investigation of choice. Here in we report a rare case of small bowel volvulus secondary to herniation of ovarian cyst through a mesenteric defect.
[1]. Mahdavi A, Yunesi N, Small bowel volvulus in a primigravida woman: Case reportJournal of Family and Reproductive Health 2007 1(1):51-54. [Google Scholar]
[2]. Vijayaraghavan SB, Ravikumar VR, Srimathy G, Whirlpool Sign in Small-Bowel Volvulus Due to a Mesenteric CystJ Ultrasound Med 2004 23:1375-77. [Google Scholar]
[3]. Heiken JP, Smithuis R, Closed Loop Obstruction in Small Bowel Obstructionhttp://www.radiologyassistant.nl/en/p4542eeacd78cf/closedloop- obstructioninsm Allbowelobstructionhtml;last seen on 19/8/2015 [Google Scholar]
[4]. Aydin U, Yazici P, Toz H, Hoscoskun C, Coker A, Management of small bowel volvulus in a patient with simultaneous pancreas-kidney transplantation a case reportJournal of Medical Case Reports 2007 1:106doi:10.1186/1752-1947-1-106 [Google Scholar]
[5]. Iwuagwu O, Deans GT, Small bowel volvulus: a reviewJ R Coll Surg Edinb 1999 44:1505 [Google Scholar]
[6]. Ali N, Mubarak M, Ali Y, Primary volvulus of the small intestineAnn Nigerian Med 2013 7:86-89. [Google Scholar]
[7]. Vaez-zadeh K, Duirz W, Nowrooz-zadeh M, Volvulus of the Small Intestine in Adults: A Study of Predisposing FactorsAnnals of Surgery 1969 169(2) [Google Scholar]
[8]. Berrocal T, Lamsa M, Gutierrez J, Torres I, Preiesto C, Hogo ML, Congenital anomalies of the small intestine, colon and rectumScientific Exhibit Radiographics 1999 19:1219-36. [Google Scholar]
[9]. Duran A, Duran FY, Cengiz F, Duran O, Intestinal Necrosis due to Giant Ovarian Cyst: A Case ReportHindawi Publishing Corporation Case Reports in Surgery 2013 2013:831087 [Google Scholar]
[10]. Valladares E, Rodríguez D, Vela A, Cabré S, Lailla JM, Meconium pseudocyst secondary to ileum volvulus perforation without peritoneal calcification: a case reportJournal of Medical Case Reports 2010 4:292 [Google Scholar]
[11]. Hong MY, Chi CH, Small-Intestinal VolvulusN Engl J Med 2011 365(4):358 [Google Scholar]
[12]. Sivaslioglu AA, Aksut H, Iri R, Small bowel necrosis secondary to three times torsion of an ovarian dermoid cyst in a 55-year-old woman: a case reportJ Cases Obstet Gynecol 2014 1(1):5-7. [Google Scholar]
[13]. Roy A, Acharya AN, Nath N, Congenital mesenteric defect — A rare cause of internal herniation in adultsHellenic Journal of Surgery 2014 86:391-93. [Google Scholar]
[14]. Rehman ZU, Khan S, Large Congenital Mesenteric Defect Presenting in an AdultSaudi J Gastroenterol 2010 16(3):223-25. [Google Scholar]
[15]. Katis PG, Dias SM, Volvulus: A rare twist on small-bowel obstructionJAMC 2004 171(7) [Google Scholar]