Introduction
Obstructive uropathy is very common cause of pain abdomen. Recognition of the cause of the pain and level of obstruction is the goal. Ultrasound is the primary modality used for detection and characterization of obstructive uropathy along with conventional radiographs. Obstructive uropathy in early stages can be difficult to diagnose using standard B-mode USG or arterial sensitive index.
Aim
The purpose of this study is to evaluate the diagnostic accuracy of renal venous doppler ultrasound in diagnosing acute obstructive uropathy either alone or in addition to arterial doppler study of inter lobar arteries. As there is limited literature available till date on Indian population regarding renal venous doppler in obstructive uropathy, this study can be useful.
Materials and Methods
Fifty patients presenting with features suggestive of obstructive uropathy were studied and compared with non-obstructed kidney of the same patient. Fifty normal individuals were studied and taken as controls.
Results
The mean venous impedance index on the obstructed side (0.26 ± 0.07) was less than the mean venous impedance index on the unobstructed side (0.41 ± 0.08) and was statistically highly significant. There was no statistically significant difference in mean arterial Resistivity Index (RI).
Conclusion
Thus renal venous doppler study is a reliable tool in diagnosing cases of acute obstructive uropathy. Though its use as single parameter to identify obstruction still needs further studies, it can be used in conjugation with b mode ultrasound and arterial Doppler to identify obstruction.
Introduction
Obstructive uropathy is one of the common cause of pain abdomen seen in emergency department. Obstructive uropathy in early stages can be difficult to diagnose using standard B-mode USG or arterial sensitive index. During obstruction of urinary tract, the pressure in the collecting system increases causing reduction in renal parenchymal compliance which affects the intraparenchymal venous blood flow to a greater degree than arterial flow [1].
Objectives
Objective is to evaluate the diagnostic reliability of renal venous doppler study in addition to Arterial Doppler study of inter lobar arteries in diagnosing obstructive uropathy.
Scanned Views Obtained
Coronal: Kidneys, Ureters when dilated.
Sagittal: Ureters, Urinary bladder.
Axial: Kidneys, Bladder.
Materials and Methods
In the 3 year study from October 2010 to October 2013, 100 cases were selected for this study. The cases were recruited from casualty, medical, surgical departments.
Patients (both males and females) with history of renal colic (<4 weeks) with positive evidence of obstruction noted on Ultrasound/Intravenous urography & CT scan were included in the study. However, patients with congenital conditions affecting the kidney, acute/chronic infections and focal lesions affecting the kidney (both benign and malignant tumours) were excluded from the study. Also patients with systemic diseases causing renal parenchymal changes like diabetes, hypertension and connective tissue disorders were also excluded from the study.
All eligible patients were properly counseled. There were three machines used in this study. Toshiba Xario – Prime, GE logiq P-5 and Philips – HD 15.
Initially the patients were evaluated with gray scale transabdominal imaging to evaluate the potential features of obstructive uropathy. Complete survey of the urinary tract was performed. Observations include size, shape, echo texture of the kidneys, pelvicalyceal system and presence of calculi in both coronal and axial images. Then examination for any dilatation of ureter and presence of the calculi in the ureter was done. Urinary Bladder examined for any vesico ureteric junction and distal ureteric calculi. The presence of calculus is diagnosed by the presence of strong echogenic focus with a distal acoustic shadowing and twinkling artifact on colour doppler. This was confirmed either by radiograph KUB/CT scan. The findings of USG are thus correlated with radiograph KUB/CT scan. All the individuals were subjected to arterial doppler of interlobar arteries and renal venous doppler study of Interlobar veins.
The following parameters were obtained in both inter lobar arteries and veins in obstructed and non-obstructed kidneys.
1. PSV 2. EDV 3. RI 4. II (Impedance Index)
The venous impedance index was calculated from PSV, EDV by the formula [1]

Statistical Analysis
Results are expressed as mean+SD and proportions as percentages. Diagnostic validity tests were performed to assess the diagnostic value of sonographic and clinical diagnosis. Statistical analysis was performed with a commercially available statistical software program (SPSS 22.0).
Results
A total of 100 individuals were evaluated by performing renal venous doppler study, of which 50 patients presented with clinical history of obstructive uropathy and 50 were controls (normal persons) with no history of obstructive uropathy. There were no significant differences between right and left kidneys in the arterial and venous impedance indices of the control group. In acute cases, the mean arterial RI on the obstructed side (0.62 ± 0.07) was greater than the index on the unobstructed side (0.59 ± 0.05). However this was not statistically significant (p = .42). The mean venous impedance index on the obstructed side was (0.26 ± 0.06). This was less than the mean venous impedance index on the unobstructed side of cases (0.41 ± 0.08) and was highly statistically significant since (p = 0.0001). In all cases of obstruction presenting late, there was mild to moderate dilatation of the collecting system, cases with severe dilatation were not included in the study.
Age and sex distributions of cases and controls are shown in [Table/Fig-1,2] respectively. Clinical features and site of obstruction identified is tabulated in [Table/Fig-3,4] respectively. Arterial and venous indices are shown in [Table/Fig-5,6] respectively.
Age distribution in study group
| Age(Years) | Number ofCases (n=50) | Percentage | Number ofcontrols (n=50 | Percentage |
|---|
| 10-20 | 2 | 4% | - | - |
| 20-30 | 11 | 22% | 15 | 30% |
| 31-40 | 24 | 48% | 16 | 32% |
| 41-50 | 08 | 16% | 13 | 26% |
| 51-60 | 05 | 10% | 06 | 12% |
Sex distribution in study group
| Sex | Number of Cases (n=50) | Percentage | Number of controls (n=50) | Percentage |
|---|
| Male | 39 | 78% | 30 | 60% |
| Female | 11 | 22% | 20 | 40% |
| Clinical features | Number of Cases (n=50) | Percentage |
|---|
| Loin pain | 50 | 100% |
| Hematuria | 17 | 34% |
| Vomitings | 19 | 38% |
| Clinical features | Number of Cases (n=50) | Percentage |
|---|
| PUJ | 5 | 10% |
| URETER | 19 | 38% |
| VUJ | 26 | 52% |
| S.NO | OBSTRUCTIVE | NON OBSTRUCTIVE | CONTROL (Right) | CONTROL (Left) |
|---|
| MEAN | 0.62 ± 0.07 | 0.59 ± 0.05 | 0.56 ± 0.04 | 0.57± 0.04 |
| PSV, (cm/s) | 36 ± 11 | 33 ± 12 | 32 ± 10 | 31 ± 9 |
| S.NO | OBSTRUCTIVE | NON OBSTRUCTIVE | CONTROL(Right) | CONTROL(Left) |
|---|
| MEAN | 0.26 ± 0.06 | 0.41 ± 0.08 | 0.41 ± 0.08 | 0.42 ± 0.07 |
| PSV, (cm/s) | 24 ± 11 | 21 ± 12 | 15 ± 8 | 17 ± 7 |
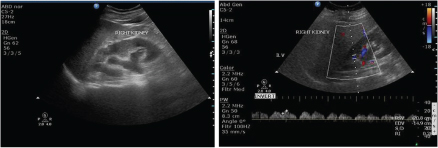
Transabdominal scan showing right hydronephrosis due to 8 mm calculus in the right pelvi ureteric junction. Renal venous doppler study shows decreased impedance in [Table/Fig-7].
Renal venous doppler study shows decreased impedance
Discussion
Sonography is the initial tool for detecting various renal pathologies, however gray scale sonography has low sensitivity for detecting acute ureteric obstruction [2].
Conventional gray scale sonography has high sensitivity (≥90%) but low specificity (65%–84%) for urinary system dilatation in the diagnosis of renal obstruction [3] and may miss the diagnosis because pyelocaliectasis can occur late in obstructive conditions [4].
Conventional grayscale USG identifies only anatomical changes like pelviureteric dilatation in ureteral obstruction and it cannot distinguish this from other causes of collecting system dilatation like residual dilatation from previously existing relieved obstruction, extrarenal pelvis and pyelonephritis on gray-scale USG alone [5]. Moreover, in an acute setting, obstruction may persist for several hours prior to collecting system dilatation [4].
Arterial RI measurements by duplex doppler sonography can be used for the diagnosis of obstruction as they detect subtle intrarenal blood flow changes [6]. It is useful to assess renal blood flow by doppler sonography together with real-time sonographic information of the collecting system [7].
Much of the research using doppler sonography of the renal arterial system to diagnose obstructions has relied on measurements of vascular impedance, such as the resistive index. The rationale has been that after 3 hours of unilateral obstruction, renal blood flow declines [8], which suggests an overall increase in renal resistance that should be measurable using the resistive index. A resistive index of 0.7 has been designated to be the upper limit of the normal range [9], with higher values suggesting obstruction [2]. The problem has been that the elevation in the resistive index above the normal range is not great, and the overlap between normal and abnormal is considerable [10–12]. The internal control afforded by the unobstructed kidney has been used to overcome the limitations of poor sensitivity and specificity and to improve accuracy. Meletic et al., found that “a difference in resistive index between the two sides of greater than or equal to 0.06 had a sensitivity of 94% and a specificity of 99%” [13]. The difficulty in reproducibly measuring a physiologic variable to an accuracy of 0.06 is considerable. Because of difficulties associated with using the arterial resistive index as a measure of acute obstruction, studies are focused on the venous side of the vascular tree.
There is reversal of flow at the end of diastole which is propagated into the renal vessels. It is known that there is a high inflow of blood into the kidney and thus a temporary reduction in outflow must be accommodated by enlargement of the veins which is known as compliance [5]. If the veins are rendered non compliant because of an increase in interstitial pressure, this end diastolic flow reduction is reduced. As a corollary, if compliance is increased, venous pulsatility also increases.
On the venous side, the normal resistance is negligible, and the pulsatility directly relates to compliance. There is a reduction in resistance in the unobstructed kidney, but in a study done by Grant A Bateman and Ramesh Cuganesan, the arterial resistive index was not sensitive to this change [1]. Due to the lack of sensitivity of the arterial resistive index, the venous impedance index of the interlobar veins was performed.
In our series we observed that there is not much of difference between the arterial resistive index of obstructive and non obstructive cases. The mean arterial resistive index on the obstructive side is 0.62 and the mean arterial resistive index on the non obstructive kidneys is 0.58 and controls are 0.57. This shows that the arterial resistive index is not a very reliable index in evaluation of cases of acute obstructive uropathy.
In comparison the venous impedance index values on the obstructed side (mean 0.26) were lower than on the unobstructed side (mean 0.41) and in the control subjects.
The present study is compared to Grant A Bateman et al., and Suna Özhan Oktar et al., in [Table/Fig-8a&b] (arterial indices & venous indices) [1,14]. Difference in venous impedance indexes was noted in all these three studies. Though difference in arterial impedance value was noted in our study, it was not statistically significant. These findings were similar to that of Grant A Bateman et al., whereas in Suna Özhan Oktar et al., difference in arterial impedance was also statistically significant [1,14].
| Study group / Arterial Impedance | Test group—obstructed kidney | Test group—unobstructed kidney | Control group—right kidney | Control group—left kidney |
|---|
| Grant A Bateman et al., [1] | 0.67 ± 0.08 | 0.62 ± 0.05 | 0.64 ± 0.10 | 0.64 ± 0.10 |
| Suna Özhan Oktar et al., [14] | 0.62 ± 0.06 | 0.57 ± 0.06 | 0.61 ± 0.09 | 0.62 ± 0.08 |
| Present study | 0.62 ± 0.06 | 0.58 ± 0.06 | 0.56 ± 0.04 | 0.57 ± 0.04 |
| Study group / Arterial Impedance | Test group—obstructed kidney | Test group—unobstructed kidney | Control group—right kidney | Control group—left kidney |
|---|
| Grant A Bateman et al., [1] | 0.38 ± 0.25 | 0.80 ± 0.25 | 0.45 ± 0.18 | 0.45 ± 0.19 |
| Suna Özhan Oktar et al., [14] | 0.25 ± 0.07 | 0.53 ± 0.25 | 0.42 ± 0.18 | 0.44 ± 0.21 |
| Present study | 0.26 ± 0.06 | 0.41 ± 0.08 | 0.41 ± 0.08 | 0.42 ± 0.07 |
Limitations
This study evaluated only acute obstructive uropathy but not chronic uropathy. Age and sex matching was not done with reference to arterial and venous doppler indices.
Conclusion
The present study shows that majority of the cases with obstruction showed a decrease in the venous impedance index. The difference in arterial resistive index between the obstructive and non-obstructive kidneys is not significant. This study showed that venous impedance index is a much better parameter than arterial resistive index in evaluating obstructive uropathy.
This parameter when used in conjunction with arterial RI values can predict hemodynamic changes associated with renal obstruction. However, large multicentric trials are needed to validate the same.
[1]. Bateman GA, Cuganesan R, Renal vein Doppler sonography of obstructive uropathyAJR 2002 178:921-25. [Google Scholar]
[2]. Mostbeck GH, Zontsich T, Turetschek K, Ultrasound of the kidney: obstruction and medical diseasesEur Radiol 2001 11:1878-89. [Google Scholar]
[3]. Ellenbogen PH, Scheible FW, Talner LB, Leopold GR, Sensitivity of gray-scale ultrasound in detecting urinary tract obstructionAJR Am J Roentgenol 1978 130:731-33. [Google Scholar]
[4]. Platt JF, Rubin JM, Ellis JH, Acute renal obstruction: Evaluation with intrarenal duplex Doppler and conventional USRadiology 1993 186:685-88. [Google Scholar]
[5]. Mahir Kaya (2012). The Evaluation of Renal Hemodynamics with Doppler Ultrasonography, Hemodynamics - New Diagnostic and Therapeutic Approaches, Dr. A Seda Artis (Ed.) [Google Scholar]
[6]. Saboo SS, Soni SH, Saboo SH, Chinapuvvula NR, Kaza S, Doppler sonography in acute renal obstructionIndian J Radiol Imaging 2007 17:188-92. [Google Scholar]
[7]. Platt J, Marn C, Baliga P, Ellis JH, Rubin JM, Merion RM, Renal Dysfunction in Hepatic Disease: Early Identification with Renal Duplex Doppler US in Patients Who Undergo Liver TransplantationRadiology 1992 183:801-06. [Google Scholar]
[8]. Moody TE, Vaughan ED, Gillenwater JY, Relationship between renal blood flow and ureteral pressure during 18 hours of total unilateral ureteral occlusionInvestig Urol 1975 13:246-51. [Google Scholar]
[9]. Chen J, Pu Y, Liu S, Chin TY, Renal Hemodynamics in Patients with Obstructive Uropathy Evaluated by Duplex Doppler SonographyJ Urol 1993 150:18-21. [Google Scholar]
[10]. Rodgers PM, Bates JA, Irving HC, Intrarenal Doppler ultrasound studies in normal and acutely obstructed kidneysBr J Radiol 1992 65:207-12. [Google Scholar]
[11]. Karadeniz T, Topsakal M, Eksioglu A, Ariman A, Basak D, Renal hemodynamics in patients with obstructive uropathy evaluated by color Doppler sonographyEur Urol 1996 29:298-301. [Google Scholar]
[12]. Salgado OJ, Martin MG, Urdaneta B, Garcia R, Rodriguez-Iturbe B, Serial pulsatility index measurements in renal grafts before, during, and after episodes of urinary obstructionJ Ultrasound Med 1999 18:827-30. [Google Scholar]
[13]. Meletic D, Fuckar Z, Sustic A, Mozetic V, Smokvina A, Stancic M, Resistance and pulsatility indices in acute renal obstructionJ Clin Sonography 1998 26:79-84. [Google Scholar]
[14]. Oktar SÖ, Yücel C, Özdemir H, Karaosmanoglu D, Doppler sonography of renal obstruction: value of venous impedance index measurementsJ Ultrasound Med 2004 23:929-36. [Google Scholar]