Benign and malignant biliary obstructions are difficult to differentiate with imaging alone. Benign obstruction is most commonly caused by choledocholithiasis. Other causes are post cholecystectomy stricture, inflammatory, stricture formation secondary to pancreatitis and idiopathic cause. Other causes of benign obstruction are choledochal cyst, primary sclerosing cholangitis, and Mirrizi syndrome [1,2]. Malignant obstruction is most commonly caused by cholangiocarcinoma. Other causes are carcinoma gall bladder, carcinoma head of pancreas, lymph nodes and metastasis [2–4]. MRCP is a well-established modality in detection of dilated biliary tree and its causes are calculus, masses. However in few cases, it is difficult to differentiate whether the obstruction is caused by inflammatory cause or a stricture is malignant in nature. Hence, we carried out a study to detect features of obstruction to differentiate benign from malignant cause using MRCP and correlated with surgical, ERCP and histological diagnosis.
To evaluate the role of MRCP in differentiating benign from malignant causes of biliary obstruction using surgical, ERCP or histopathological diagnosis as gold standard.
Materials and Methods
This prospective study was done from May 2013 to May 2014. Total 75 patients with clinical and laboratory finding suggestive of biliary obstruction were included in our study. Patients with metallic implant insertion, cardiac pacemakers, metallic foreign body in-situ, patients having history of claustrophobia and patients who required sedation or ventilation were excluded from the study. Imaging was done on Philips Achivia 3.0 Tesla MRI machine using body coil. Examination was performed after the patient had fasted for minimum of 4 hours to promote gall bladder filling. Oral negative contrast agent (Pineapple juice 100 ml) was given to patient 15 min before examination to improve image quality and contrast.
MRCP sequences used were axial T1W SENSE, axial and coronal T2W SENSE, Fat suppressed T2W SPAIR, thick slab MRCP, heavily T2W high resolution 3D. MRI scan parameters are given in [Table/Fig-1]. The observations made on MRCP/MRI were biliary channels, their asymmetrical/ symmetrical dilatation, pancreatic duct, calculus, stricture’s site, margins (regular/irregular), tapering (abrupt/gradual), length of stricture (long/short), Gall Bladder, lymph nodes, metastasis.
| T1 TFE | T2w axial | T2W coronal | FAT SAT SPAIR | SSh_MRCPrad | sMRCP 3D |
|---|
| TR | 10 | 1331 | 1864 | 1277 | 9449 | 2580 |
| TE | 2.3 | 80 | 80 | 70 | 740 | 740 |
| Time of Scan | 1.15 | 1.15 min | 1.15 min | 1.15min | 1.25min | 4.06min |
| Slice Width | 7 | 7 mm | 4mm | 7mm | 40mm | 300mm |
| No of Sections | 25 | 25 | 25 | 25 | 9 | 3 |
| Field of View (mm) | 375 | 375 | 375 | 375 | 300 | 300 |
| Matrix size | 252×512 | 268x512 | 268x166 | 268×512 | 320x512 | 256×512 |
| Flip angle | 15° | | | | 37° | |
Statistical Analysis
Data analysis was done using rates, ratios and percentages of different diagnosis. Diagnostic effectivity was calculated for MRCP which included sensitivity, specificity and accuracy by comparing with surgical, histopathological or ERCP findings. Statistical analysis was done by using chi-square test and p-value was calculated.
Results
Total 75 patients with clinical suspicion of biliary obstruction were imaged by MRI/MRCP. Out of these, 54 (72%) cases were benign and 21 (28%) were malignant in nature. Malignant lesions were more common in older patients as compared with benign lesions. Mean age of patients with benign obstruction was 47.6±17.03 years and of malignant obstruction was 55±16.3years. There was slight male preponderance in biliary obstructive diseases in our study. Most common symptom affecting the patients was pain abdomen and yellowish discoloration of skin and sclera. Vomiting and fever were more commonly seen in patients with benign obstruction whereas loss of appetite and weight loss were more common in malignant obstruction. Various biliary obstructive diseases in the present study are given in [Table/Fig-2].
Various Biliary Obstructive Diseases on the basis of final diagnosis on surgical, ERCP or histopathological outcome
| S No. | Diagnosis | Cases | Percentage |
|---|
| 1 | Choledochal cyst | 11 | 14.7% |
| 2 | Choledocholithiasis | 18 | 24% |
| 3 | Pancreatitis | 4 | 5.3% |
| 4 | Inflammatory stricture | 5 | 6.7% |
| 5 | Postcholecystectomy stricture | 15 | 20% |
| 6 | Primary sclerosing cholangitis | 1 | 1.3% |
| 7 | Cholangiocarcinoma | 13 | 17.3% |
| 8 | Carcinoma Gallbladder | 2 | 2.7% |
| 9 | Periampullary mass | 4 | 5.3% |
| 10 | Carcinoma head of pancreas | 2 | 2.7% |
| Total | 75 | 100% |
The most common cause of benign obstruction in present study was choledocholithiasis [Table/Fig-3] 18 (24%), followed by post-cholecystectomy strictures 15 (20%). Other benign causes were choledochal cyst 11 (14.7%), inflammatory strictures 5 (6.7%), pancreatitis 4(5.3%) and primary sclerosing cholangitis 1(1.3%). Causes of benign strictures in our study are given in [Table/Fig-4].
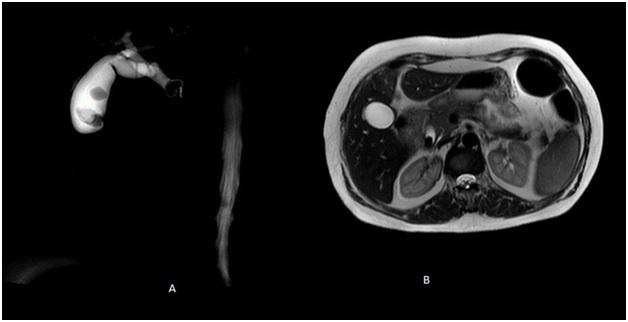
Choledocholithiasis with Cholelithiasis (a) MRCP image shows multiple well defined filling defects (arrow), suggestive of multiple calculi, in the lumen of CBD and gall bladder (b) T2W axial image shows filling defect suggestive of calculus in distal CBD
Aetiology of benign strictures in our study
| Aetiology of benign strictures | No. | Percentage |
|---|
| Iatrogenic (postcholecystectomy) | 15 | 62.5% |
| Inflammatory stricture | 5 | 20.8% |
| Pancreatitis | 4 | 16.7% |
| Total | 24 | 100% |
Among 21 cases of malignant obstruction, cholangiocarcinoma [Table/Fig-5] was the most common cause with 13 (62%) cases. Other causes of malignant obstruction were periampullary carcinoma 4 (19%), carcinoma gall bladder and carcinoma head of pancreas each 2 (9.5%) [Table/Fig-6].
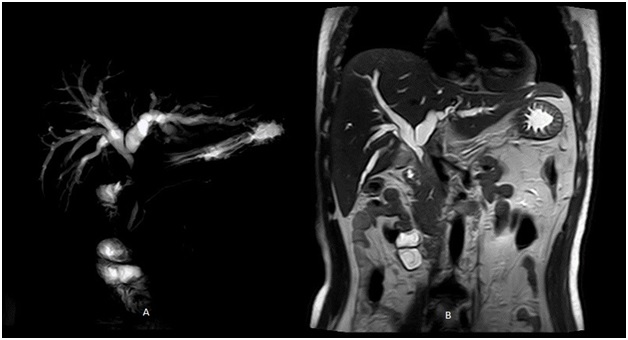
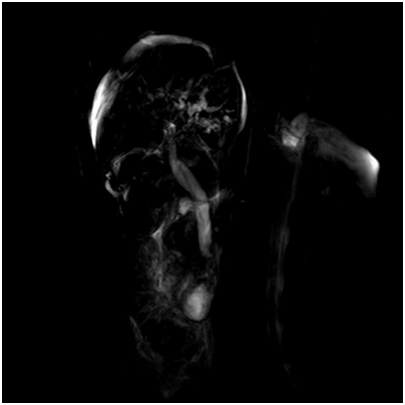
Cholangiocarcinoma (a) MRCP shows dilated IHBR in both lobes of liver with narrowing at hilum proximal and mid CBD is not visulaised. Distal CBD is normal in caliber. (b) Long segment and irregular thickening of CBD is seen on T2W coronal image suggesting malignant pathology
Aetiology of malignant strictures in our study
| Aetiology of Malignant Strictures | No. | Percentage |
|---|
| Cholangiocarcinoma | 13 | 62% |
| Periampullary carcinoma | 4 | 19% |
| Pancreatic carcinoma | 2 | 9.5% |
| Gall bladder carcinoma | 2 | 9.5% |
| Total | 21 | 100% |
These diseases were categorized into 5 groups based on the cause of obstruction as seen on final diagnosis [Table/Fig-7]. The most common pathology in present study was benign stricture consisting 24 (32%) cases. Causes of benign strictures included postcholecystectomy stricture [Table/Fig-8], (m/c) 15 (62.5%) inflammatory stricture 5 (20.8%) and stricture secondary to pancreatitis [Table/Fig-9]. 4 (16.7%) Malignant stricture group consisted 21 (28%) cases which included cholangiocarcinoma (m/c) 13 (62%), periampullary carcinoma 4 (19%), carcinoma gall bladder 2 (9.5%) and pancreatic head carcinoma 2 (9.5%). Other disease groups were choledocholithiasis 18 (24%), choledochal cyst 11 (14.7%) and primary sclerosing cholangitis 1 (1.3%).
Classification of patients on the basis of cause of biliary obstruction
| Sr. | Diagnosis | No. | Percentage |
|---|
| 1. | Choledocholithiasis | 18 | 24% |
| 2. | Benign stricture | 24 | 32% |
| 3. | Malignant stricture | 21 | 28% |
| 4. | Choledochal cyst | 11 | 14.7% |
| 5. | Primary sclerosing cholangitis | 1 | 1.3% |
| Total | 75 | 100% |
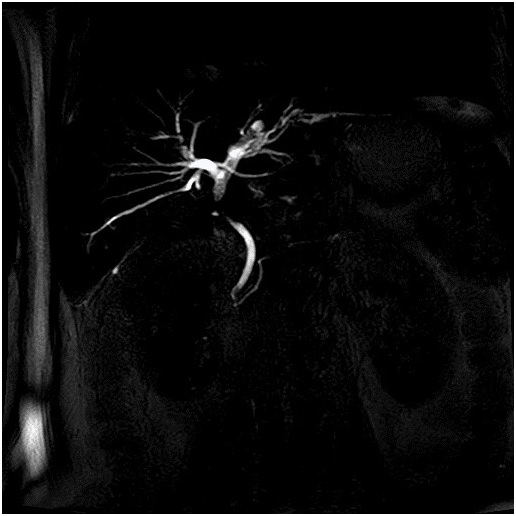
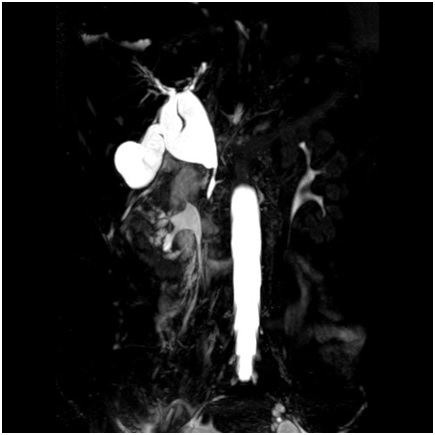
Post Cholecystectomy Stricture: MRCP image show dilated IHBR with abrupt, short segment narrowing at hilum, mid and distal CBD normal in caliber
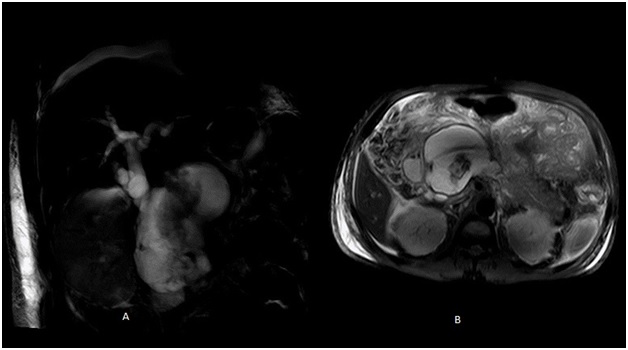
CBD Stricture with Pancreatitis (a) dilated IHBR and CBD seen on MRCP image with fluid collection near distal end of CBD. Distal CBD narrows abruptly. (b) T2W axial image shows pseudocyst near head of pancreas and pancreatitis involving body and tail region
Final diagnosis in present study was based on surgical, histopathological or ERCP correlation. MRCP findings were then correlated with final diagnosis and diagnostic effectivity of MRCP was calculated for individual group of diseases and for overall biliary obstructive diseases. MRCP correctly diagnosed all 18 cases of choledocholithiasis and one case of primary sclerosing cholangitis [Table/Fig-10]. All 11 cases of choledochal cyst were correctly diagnosed by MRCP. 1 case of cholangiocarcinoma was falsely diagnosed as choledochal cyst on MRCP. Type of choledochal cyst was correctly diagnosed in all the cases by MRCP. According to Todani’s classification [5], there were 9 cases of fusiform extrahepatic choledochal cyst (Type I), 2 cases of combined intrahepatic and extrahepatic choledochal cyst (Type IVa) [Table/Fig-11]. Thus sensitivity of MRCP for detection of choledochal cyst was 100%, specificity 98.4%, and diagnostic accuracy 98.7%.
Primary Sclerosing Cholangitis: MRCP image shows multiple strictures, irregularities of bile ducts and bile duct wall thickening
Choledochal cyst: MRCP image shows dilated both intra and extrahepatic biliary ducts suggestive of choledochal cyst type IV a
In present study, 22 cases of benign stricture were correctly diagnosed on MRCP. Two cases of periampullary carcinoma were wrongly diagnosed as benign strictures on MRCP. Two cases of benign strictures were wrongly diagnosed as malignant strictures on MRCP. Thus sensitivity of MRCP for detection of benign strictures was 91.7%, specificity 96.1% and diagnostic accuracy 94.7%. In our study, 18 cases of malignant stricture were correctly diagnosed on MRCP. Two cases of benign strictures were wrongly diagnosed as malignant stricture on MRCP. Two cases of periampullary carcinoma were wrongly diagnosed as benign stricture on MRCP and one case of cholangiocarcinoma was wrongly diagnosed as choledochal cyst on MRCP. Thus sensitivity of MRCP for detection of malignant strictures was 85.7%, specificity 96.3% and diagnostic accuracy 93.3% [Table/Fig-12].
Diagnostic effectivity of MRCP in various pathologies in comparison with surgical, ERCP and histopathological outcome
| Disease Group | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | p-value |
|---|
| Choledocholithiasis | 100 | 100 | 100 | 100 | 100 | <0.0001 |
| Choledochal cyst | 100 | 98.4 | 91.7 | 100 | 98.7 | <0.0001 |
| Primary sclerosing cholangitis | 100 | 100 | 100 | 100 | 100 | <0.0001 |
| Benign stricture | 91.7 | 96.1 | 91.7 | 96.1 | 94.7 | <0.0001 |
| Malignant stricture | 85.7 | 96.3 | 90 | 94.5 | 93.3 | <0.0001 |
In present study, regular, symmetric and short segment narrowing was more commonly found in benign strictures. Irregular, asymmetric and long segment narrowing was more commonly found in malignant stricture. Presence of mass was highly specific for malignant strictures but absence of mass did not rule out possibility of malignancy. Abrupt or gradual tapering did not show any specific distribution and was not helpful in differentiating benign from malignant stricture [Table/Fig-13].
Sensitivity, Specificity, PPV, NPV, diagnostic accuracy and P-value of various stricture characters in differentiating malignant from benign strictures
| Stricture character | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Diagnostic accuracy (%) | p-value |
|---|
| Margin | 95.2% | 87.5% | 86.9% | 95.4% | 91.1% | 0.0001 |
| Asymmetrical dilation of IHBR | 71.4% | 87.5% | 83.3% | 77.8% | 80% | 0.0002 |
| Tapering of stricture | 19% | 91.6% | 66.7% | 56.4% | 57.8% | 0.5384 |
| Length of stricture | 57.1% | 91.7% | 85.7% | 71% | 75.5% | 0.0013 |
| Mass | 62% | 96% | 92.8% | 74% | 80% | 0.0001 |
Overall diagnostic accuracy of MRCP in differentiating benign from malignant biliary obstructive diseases in correlation with surgical, ERCP and histopathological outcome was 93.3%, sensitivity 85.7% and specificity 96.3% [Table/Fig-14].
Overall diagnostic effectivity of MRCP in differentiating benign from malignant biliary obstructive diseases in correlation with surgical, ERCP and histopathological outcome- Using Chi-square test, χ2 = 47.893 with 1 degrees of freedom; p <0.0001, Sensitivity=85.7%, Specificity=96.3%, Diagnostic accuracy=93.3%
| MRCP finding | Final diagnosis |
|---|
| True positive(Malignant) | True negative(Benign) | Total |
|---|
| Test positive(Malignant) | 18 | 2 | 20 |
| Test negative(Benign) | 3 | 52 | 55 |
| Total | 21 | 54 | 75 |
Discussion
Differentiation of benign from malignant biliary obstruction has been one of the challenges for the radiologist by imaging alone. The reported accuracy in differentiation of benign from malignant cause of obstruction has varied from 30-80 % [6–9]. We carried out a prospective study using MRCP to differentiate benign and malignant biliary obstruction. In present study, mean age of patients with malignant biliary obstruction was higher than benign obstruction. Similar results were seen in study conducted by Saluja et al., [10]. Biliary obstructive diseases were found to be more common in men than in women in our study with a ratio equal to 13:12. Benign diseases were equally distributed in both sexes. Malignant diseases were more common in males similar to Saluja et al., and Park et al., [10,11].
The most common symptoms we found in patients with biliary obstruction were right upper quadrant pain and yellowish discoloration of skin and sclera. Loss of appetite and weight loss were more common symptoms found in patients with malignant pathologies similar to Saluja et al., [10].
Among 75 cases, Choledocholithiasis was the most common pathology seen in our study seen in 18 (24%) patients. These pathologies were categorized into five groups according to the cause of obstruction as observed on surgery or ERCP. Benign stricture was the most common cause of obstruction consisting 24 (32%) cases. The most common cause of benign stricture in our study was postcholecystectomy stricture 15 (62.5%) cases. There were 21 cases of malignant stricture in our study with cholangiocarcinoma being the most common cause with 13 (62%) cases.
All 18 cases of choledocholithiasis were correctly diagnosed on MRCP giving 100% sensitivity, 100% specificity and 100% diagnostic accuracy which was similar to that in study done by Varghese et al., [12]. {Sensitivity 91%, Specificity 98% and accuracy 97%}.
There were 11 cases of choledochal cyst in our study which were correctly diagnosed on MRCP with one case of cholangiocarcinoma falsely diagnosed as choledochal cyst, giving 100% sensitivity, 98.4% specificity and 98.7% diagnostic accuracy. According to Todani’s classification [5], there were 9 cases of fusiform extrahepatic choledochal cyst (Type I), 2 cases of combined intrahepatic and extrahepatic choledochal cyst (Type IVa) in our study. Similarly Type I choledochal cyst was the most common cyst in study done by Lipsett et al., [13].
We had one case of primary sclerosing cholangitis in our study, which showed multiple strictures, irregularities of bile ducts and bile duct wall thickening on MRCP. Similar findings were described by Katabathina et al., in cases of primary sclerosing cholangitis on mrcp [2]. In present study, there were 24 cases of benign biliary stricture. MRCP had sensitivity 91.7%, specificity 96.1%, and accuracy 94.7% for diagnosis of benign strictures. Hintze et al., in 1997 found sensitivity 87% and specificity 87% of MRCP for the diagnosis of benign stricture [14]. Lee et al., in their study found that sensitivity of MRCP in diagnosis of benign lesions was 81%, specificity 92% and accuracy 87% [15].
Among 21 malignant strictures, MRCP detected 18 cases correctly with sensitivity 85.7%, specificity 96.3% and accuracy 93.3%. Similar results were seen in studies done by Reinhold et al., and Lopera et al., [16,17].
Irregular margins of the stricture were more commonly found in malignant strictures. Asymmetrical dilatation of biliary radicals was more commonly associated with malignant strictures. Smooth margin of strictures and symmetrical dilatation of biliary radicals were more commonly seen in benign strictures. Saluja et al., suggested in their study that malignant strictures were irregular with an asymmetric dilatation because of the nature of involvement of the bile duct by the malignant tumour [10].
In previous studies, abrupt narrowing was more commonly observed in benign pathologies due to ultrashort strictures of the CBD [2]. Park et al., stated that abundant fibrosis and desmoplastic reaction without definite mass formation in some bile duct carcinomas may lead to a stricture that involves a long ductal segment and appears gradually tapered and without mass effect rather than abruptly narrowed [11]. However, in present study, abrupt or gradual tapering of strictured segment did not showed any correlation with benign or malignant strictures. This may be due to the fact that the extrahepatic bile duct distal to the obstruction may have been collapsed at the time of MRCP, which may have caused overestimation of gradual tapering of the stricture on MRCP images in our study.
We found that long segment narrowing was more commonly found in malignant stricture and short segment strictures were more commonly benign in nature. Malignant strictures are usually long as they have an infiltrative growth pattern, which spreads intramurally beneath the epithelial lining [10]. Yu et al., also reported that malignant strictures were significantly thicker and longer than the benign strictures and upstream CBD dilatation was larger in the infiltrative cholangiocarcinoma cases than in the benign cases [18]. In their study, Park et al., concluded that MR Cholangiopancreatography is comparable to ERCP in differentiating extrahepatic bile duct cholangiocarcinoma from a benign stricture and showed that a lengthy narrowed segment with irregular margins and asymmetric narrowing is suggestive of malignancy [11]. Kim et al., showed that a narrowed segment with the following MR imaging features is more likely to be malignant: hyperenhancement relative to the liver during the portal venous phase, length of over 12 mm, wall thickness greater than 3 mm, indistinct outer margin, luminal irregularity, and asymmetry [19]. Katabathina et al., in their study found that benign strictures showed a short-segment smooth stricture of the CHD or CBD with associated intrahepatic biliary dilatation on MR Cholangiopancreatography [2]. 62% malignant strictures showed mass lesion with bile duct stricture on MRCP in our study whereas only one case of benign stricture showed mass lesion (4%) which was proved to be benign on histopathology showing inflammatory changes. Thus presence of mass was highly specific for malignant strictures but absence of mass did not rule out possibility of malignancy. These findings were similar to study by Saluja et al., where 66.6% of cases of malignant biliary strictures showed mass lesion [10].
Overall in our study, out of 75 patients, 54 cases were benign whereas 21 cases had malignant obstruction. Among 75 patients, 70 were correctly diagnosed and properly evaluated by MRCP. The sensitivity, specificity and diagnostic accuracy of MRCP for differentiation of benign from malignant causes of biliary obstruction was 85.7%, 96.3%, and 93.3% respectively. In previous studies, sensitivity of MRCP for detection of cause of benign and malignant obstruction ranged from 92-100%. Saluja et al., found sensitivity, specificity and diagnostic accuracy of MRCP for biliary obstructive diseases in their study to be 87.5%, 85.3% and 82.7% respectively similar to our study [10]. Park et al., found that the sensitivity, specificity, and accuracy of MRCP for differentiation of malignant from benign causes of biliary stricture were 81%, 70%, and 76% respectively [9].
Limitations
Surgical/histopathological/ERCP correlation could not be performed in all cases as some cases of both benign and malignant pathologies were treated conservatively.
Recommendation
From this study, it is recommended that its benign or malignant nature of biliary obstruction can be assured by MRCP by observation of stricture margin, dilatation, and length and accordingly proceed to next step in management. MRCP is an efficient diagnostic procedure for detection of presence, level, cause of obstruction and routinely advocated before any intervention is planned.
Conclusion
MRCP is an accurate, noninvasive means of evaluating biliary obstructive diseases. MRCP is the investigation of choice for suspected choledocholithiasis, choledochal cyst and primary sclerosing cholangitis. A benign stricture can be differentiated from a malignant one if it shows regular, symmetric and short segment narrowing. Irregular, asymmetric and long segment narrowing was more commonly found in malignant stricture.
Abbreviations
MRCP: Magnetic resonance cholangiopancreatography,
ERCP: Endoscopic retrograde cholangiopancreatography,
MRI: Magnetic resonance imaging,
T1W: T1 weighted,
SENSE: Sensitivity encoding,
T2W: T2 weighted,
SPAIR: Spectral attenuated inversion recovery,
3D: 3 Dimensional,
m/c: most common.