Bacteria, especially gram negative bacteria, are showing increased resistance to the current antibiotics and drug development programmes seem insufficient to provide therapeutic cover in the near future. Repeated courses of antimicrobial therapy are common in acutely ill, febrile patients, who frequently have endotracheal tubes, urinary catheters and central venous catheters [1]. In combination with host factors, indwelling devices are routes for transmission and colonization of resistant infections [2]. Lengthy or unjustified use of antibiotics helps microbes to undergo mutations which help them to resist antibiotics and become new dominant strains [3].
The incidence of infection due to extended-spectrum β-lactamase (ESBL) producing organisms has increased sharply especially in Escherichia coli and Klebsiella pneumoniae and also by Pseudomonas aeruginosa and Acinetobacter baumannii. The growing prevalence of ESBL producing organisms is responsible for increased use of carbapenems. But extensive and sometimes unnecessary use of carbapenems has facilitated the emergence of carbapenem resistant bacteria by production of carbapenem hydrolysing enzyme, metallo-β-lactamase (MBL). MBL producing Pseudomonas and Acinetobacter isolates are common cause of nosocomial infections but other MBL producing gram negative bacteria like E. coli and Klebsiella spp. are also emerging as a worldwide public health concern, especially in USA, Greece and Israel [4]. Data from India is currently insufficient.
This study was carried out to elucidate risk factors for infection with ESBL and MBL producing E. coli and Klebsiella spp.
Materials and Methods
A prospective observational descriptive study was carried out in the Department of Microbiology, Lady Hardinge Medical College, New Delhi and associated hospitals from November 2010 to March 2012.
Three hundred and fifty strains each of E. coli and Klebsiella spp. isolated from various clinical samples of inpatients were collected consecutively. Repeat isolates with the same antibiogram from the same patient were excluded from the study.
Processing of Specimens: Collection, transport and processing of specimens were done as per standard protocol [5,6].
Antimicrobial Susceptibility Tests
1) Disk Diffusion Tests: All identified strains were tested for antimicrobial susceptibility by Kirby-Bauer method on Mueller-Hinton Agar (MHA) medium according to criteria recommended by Clinical and Laboratory Standards Institute (CLSI) [7].
Following antimicrobial agents (Hi-Media) were used for antibiotic susceptibility testing: Amikacin (30 μg), Ampicillin (10 μg), Cotrimoxazole (1.25/23.75 μg), Ertapenem (10 μg), Aztreonam (30 μg), Gatifloxacin (5 μg), Cefazolin (30 μg), Imipenem (10 μg), Cefotaxime (30 μg), Norfloxacin (10 μg), Ceftazidime (30 μg), Tetracycline (30 μg), and Ciprofloxacin (5 μg).
2) Minimum Inhibitory Concentration (MIC) Determination: MIC of isolates which were positive for both ESBL and MBL was determined using microbroth dilution [8]. The isolates which showed multidrug resistance with this method were tested for NDM-1 production.
Detection of ESBL and MBL Production: The strains resistant to Ceftazidime and/or Cefotaxime were tested for ESBL production by ESBL E-test [9]. The strains which showed resistance to imipenem were tested for MBL production by MBL E-test [10].
Detection of NDM-1 Production: DNA was extracted from the strains by heat boil method and this DNA was subjected to single target PCR. Amplified products (250 bp) were analysed by electrophoresis in 2% agarose gels stained with ethidium bromide. E. coli NDM-1 positive controls were included. (Thermo Scientific Gene Ruler 1 kb DNA Ladder 250 to 10,000 bp).
Risk factor Analysis: The isolates positive for ESBL production and MBL production were analysed for various risk factors by means of a review of medical charts. Data obtained included age, sex, clinical specimen, hospital or community acquired infection, duration of hospital stay prior to collection of clinical sample, admitting ward, antimicrobial susceptibility, previous antibiotics used, presence of co-morbid illnesses like diabetes mellitus, immunodeficiency, low birth weight, respiratory/ neurological/ cardiac/ haematological/ liver diseases, malignancy, the presence of urinary or central venous catheter, ventilatory support, surgical procedures and dialysis. Nosocomial infections were defined according to Center for Disease Control and Prevention criteria.
Statistical Analysis
The association of variables was compared by the use of z-test or Fisher’s exact test as appropriate.
Results
E. coli: 192 two ESBL positive isolates were obtained from 186 patients. Analysis revealed female preponderance (65.1%) and the difference was statistically significant (p<0.001). Significantly higher isolates (p<0.0001) were obtained from males in >28 days -1 year age group and in females in >20-30 years age group [Table/Fig-1].
Correlation of isolates with age and sex of patients
| Age | E. coli | Klebsiella spp. |
|---|
| Male | Female | Total | Male | Female | Total |
|---|
| >0d - 28d | 5 (7.7) | 2 (1.7) | 7 (3.8) | 16 (21.3) | 7 (7.7) | 23 (13.9) |
| >28d - 1y | 21 (32.3) | 6 (5.0) | 27 (14.5) | 16 (21.3) | 2 (2.2) | 18 (10.8) |
| >1y - 5y | 8 (12.3) | 11 (9.1) | 19 (10.2) | 5 (6.7) | 8 (8.8) | 13 (7.8) |
| >5y - 10y | 6 (9.2) | 3 (2.5) | 9 (4.8) | 2 (2.7) | 9 (9.9) | 11 (6.6) |
| >10y - 20y | 1 (1.5) | 4 (3.3) | 5 (2.7) | 6 (8.0) | 8 (8.8) | 14 (8.4) |
| >20y - 30y | 3 (4.6) | 53 (43.8) | 56 (30.1) | 9 (12.0) | 30 (33.0) | 40 (23.5) |
| >30y - 40y | 5 (7.7) | 12 (9.9) | 17 (9.1) | 5 (6.7) | 13 (14.3) | 19 (10.8) |
| >40y - 50y | 5 (7.7) | 11 (9.1) | 16 (18.6) | 6 (8.0) | 2 (2.2) | 9 (4.8) |
| >50y - 60y | 7 (10.8) | 12 (9.9) | 19 (10.2) | 5 (6.7) | 6 (6.6) | 11 (6.6) |
| >60y - 70y | 3 (4.6) | 6 (5.0) | 9 (4.8) | 4 (5.3) | 4 (4.4) | 8 (4.8) |
| >70y - 80y | 1 (1.5) | 1 (0.8) | 2 (1.1) | 1 (1.3) | 1 (1.1) | 2 (1.2) |
| >80y - 90y | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.6) |
| Total | 65 (34.9) | 125 (65.1) | 186 | 75 (45.2) | 91 (54.8) | 166 |
Irrespective of gender, significantly higher number of isolates (p<0.001) were obtained from urine in both males and females (34.8% and 43.1% respectively). In males the frequency of isolation was followed by pus (30.4%) and blood (14.5%) (p <0.01), in females by female genital tract specimens (26.0%) (p<0.0001) and pus (17.9%) [Table/Fig-2].
Correlation of isolates with type of specimen and sex of patients
| Specimen | E. coli | Klebsiella spp. |
|---|
| Male | Female | Total | Male | Female | Total |
|---|
| Blood | 10 (14.5) | 5 (4.1) | 15 (7.8) | 13 (16.7) | 8 (8.8) | 21 (12.4) |
| Body Fluids | 5 (7.2) | 4 (3.3) | 9 (4.7) | 3 (3.8) | 0 (0.0) | 3 (1.8) |
| Female Genital Tract Specimens | 0 (0) | 32 (26.0) | 32 (16.7) | 0 (0.0) | 12 (13.2) | 12 (7.1) |
| Oral Secretions | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (2.6) | 1 (1.1) | 3 (1.8) |
| Pus | 21 (30.4) | 2 (17.9) | 43 (22.4) | 25 (32.1) | 22 (24.2) | 47 (27.8) |
| Respiratory Secretions | 8 (11.6) | 6 (4.9) | 14 (7.3) | 21 (26.9) | 9 (9.9) | 30 (17.8) |
| Stool | 1 (1.4) | 1 (0.8) | 2 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Urine | 24 (34.8) | 53 (43.1) | 77 (40.1) | 14 (17.9) | 39 (42.9) | 53 (31.4) |
| Total | 69 (35.9) | 123 (64.1) | 192 | 78 (46.2) | 91 (53.8) | 169 |
[Table/Fig-3] shows the distribution of number of ESBL producing E. coli isolates in relation to the duration of stay of the patient in the hospital prior to collection of clinical sample. Isolates showed equal percentage of hospital acquired and community acquired infection [Table/Fig-4]. However, on comparison of 50% of community acquired ESBL producing isolates individually with those isolated at different intervals from patients hospitalized for >48 hours, the observation was statistically significant (p<0.0001). Significantly higher number of isolates were received from surgical wards (55.8%) as compared to medicine (28.6%) and ICU/Post op (15.6%) wards [Table/Fig-5]. The ESBL producing isolates showed an overall high levels of resistance to cephalosporins, monobactam, penicillin, fluoroquinolones and tetracycline (>88%) but low levels to carbapenems and aminoglycosides (<25%) [Table/Fig-6] (p<0.0001).
Correlation of isolates with duration of stay in hospital
| Duration of Stay | E. coli | Klebsiella spp. |
|---|
| 0 - 48 hrs | 96 (50.0) | 74 (43.8) |
| >48 hrs - 7 days | 53 (27.6) | 58 (34.3) |
| >7 days - 14 days | 28 (14.6) | 26 (15.4) |
| >14 days - 21 days | 9 (4.7) | 7 (4.1) |
| >21 days - 28 days | 1 (0.5) | 4 (2.4) |
| >28 days | 5 (2.6) | 0 (0.0) |
| Total | 192 | 169 |
Correlation of isolates with type of infection
| Type of Infection | E. coli | Klebsiella spp. |
|---|
| Hospital acquired | 96 (50.0) | 95 (56.2) |
| Community acquired | 96 (50.0) | 74 (43.8) |
| Total | 192 | 169 |
Correlation of isolates with admitting wards
| Ward | E. coli | Klebsiella spp. |
|---|
| ICU/ Post op Ward | 30 (15.6) | 33 (19.5) |
| Medicine Ward | 55 (28.6) | 48 (28.4) |
| Surgery Ward | 107 (55.8) | 88 (52.1) |
| Total | 192 | 169 |
Antimicrobial resistance of E. coli strains isolated from different specimen
| Antibiotic | Blood(n=15) | BodyFluids (n=9) | Female GenitalTract Specimen(n=32) | Pus(n=43) | RespiratorySecretions(n=14) | Stool(n=2) | Urine(n=77) | TotalIsolates(n=192) |
|---|
| Amikacin | 7 (46.7) | 2 (22.2) | 10 (31.3) | 9 (20.9) | 3 (21.4) | 0 (0) | 18 (23.4) | 49 (13.3) |
| Ampicillin | 14 (93.3) | 9 (100.0) | 25 (78.1) | 37 (86.0) | 13 (92.9) | 2 (100.0) | 70 (90.9) | 170 (88.5) |
| Aztreonam | 15 (100.0) | 8 (88.9) | 31 (96.9) | 41 (95.3) | 13 (92.9) | 2 (100.0) | 76 (98.7) | 186 (96.9) |
| Cefazolin | 15 (100.0) | 9 (100.0) | 32 (100.0) | 43 (100.0) | 14 (100.0) | 2 (100.0) | 76 (98.7) | 191 (99.5) |
| Cefotaxime | 15 (100.0) | 9 (100.0) | 32 (100.0) | 43 (100.0) | 14 (100.0) | 2 (100.0) | 77 (100.0) | 192 (100.0) |
| Ceftazidime | 15 (100.0) | 9 (100.0) | 32 (100.0) | 43 (100.0) | 14 (100.0) | 2 (100.0) | 77 (100.0) | 192 (100.0) |
| Ciprofloxacin | 12 (80.0) | 8 (88.9) | 28 (87.5) | 40 (93.0) | 11 (78.6) | 2 (100.0) | 70 (90.9) | 171 (89.1) |
| Cotrimoxazole | 14 (93.3) | 6 (66.7) | 25 (78.1) | 32 (74.4) | 11 (78.6) | 2 (100.0) | 57 (74.0) | 147 (76.6) |
| Ertapenem | 4 (26.7) | 2 (22.2) | 2 (6.3) | 4 (9.3) | 1 (7.1) | 1 (50.0) | 13 (16.9) | 27 (14.1) |
| Gatifloxacin | 12 (80.0) | 8 (88.9) | 24 (75.0) | 37 (86.0) | 10 (71.4) | 2 (100.0) | 58 (75.3) | 151 (78.7) |
| Imipenem | 1 (6.7) | 1 (11.1) | 0 (0) | 2 (4.7) | 0 (0) | 0 (0) | 1 (1.3) | 6 (3.1) |
| Norfloxacin | 13 (86.7) | 8 (88.9) | 27 (84.4) | 39 (90.7) | 12 (85.7) | 2 (100.0) | 70 (90.9) | 171 (89.1) |
| Tetracycline | 13 (86.7) | 7 (77.8) | 24 (75.0) | 36 (83.7) | 10 (71.4) | 2 (100.0) | 72 (93.5) | 164 (85.4) |
Cephalosporins, carbapenems (p>0.05), penicillins, metronidazole and aminoglycosides were prescribed to patients infected with ESBL producing E. coli for 1-7 days prior to sending the sample. [Table/Fig-7].
Antibiotics taken prior to sending sample
| Antibiotic | E. coli | Klebsiella spp. |
|---|
| 1-7 Days | >7-14 Days | 1-7 Days | >7-14 Days |
|---|
| Amoxicillin-Clavulanic acid | 77 (40.1) | 5 (2.6) | 77 (45.6) | 1 (0.6) |
| Ampicillin | 32 (16.7) | 0 (0) | 13 (7.7) | 0 (0) |
| Piperacillin-Tazobactam | 18 (9.4) | 3 (1.6) | 58 (34.3) | 3 (1.8) |
| Metronidazole | 92 (47.9) | 14 (7.3) | 46 (27.2) | 2 (1.2) |
| Ciprofloxacin | 31 (16.1) | 9 (4.7) | 9 (5.3) | 2 (1.2) |
| Ofloxacin | 4 (2.1) | 1 (0.5) | 5 (3.0) | 0 (0) |
| Levofloxacin | 20 (10.4) | 0 (0) | 19 (11.2) | 1 (0.6) |
| Norfloxacin | 12 (6.3) | 0 (0) | 8 (4.7) | 0 (0) |
| Amikacin | 56 (29.2) | 7 (3.6) | 114 (67.5) | 4 (2.4) |
| Gentamicin | 35 (18.2) | 7 (3.6) | 11 (6.5) | 2 (1.2) |
| Clindamycin | 1 (0.5) | 0 (0) | 0 (0) | 2 (1.2) |
| Cefotaxime | 20 (10.4) | 0 (0) | 25 (14.8) | 0 (0) |
| Ceftriaxone | 45 (23.4) | 6 (3.1) | 34 (20.1) | 4 (2.4) |
| Ceftazidime | 2 (1.0) | 1 (0.5) | 3 (1.8) | 0 (0) |
| Cefixime-Sulbactam | 6 (3.1) | 0 (0) | 1 (0.6) | 0 (0) |
| Cefepime | 3 (1.6) | 1 (.5) | 2 (1.2) | 0 (0) |
| Aztreonam | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) |
| Imipenem | 11 (5.7) | 2 (1.0) | 6 (3.6) | 1 (0.6) |
| Meropenem | 8 (4.2) | 1 (.5) | 17 (10.1) | 2 (1.2) |
| Ertapenem | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) |
| Azithromycin | 3 (1.6) | 1 (0.5) | 3 (1.8) | 0 (0) |
| Tobramycin | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
| Colistin | 0 (0) | 0 (0) | 1 (0.6) | 1 (0.6) |
Significantly higher number of patients of ESBL positive isolates (p<0.0001) had undergone surgery (61.83%), 58.6% had urinary catheter in-situ, 18.28% had a haematological disease, 8.06% required ventilatory support (p<0.0001), 11.83% had diabetes mellitus and 5.91% had a neurological disease (p<0.01) [Table/Fig-8].
Analysis of Co-morbidities and other risk factors with ESBL producing and non-ESBL producing isolates
| Associated disease/ Risk factor | E. coli | Klebsiella spp. |
|---|
| ESBL positive | ESBL negative | ESBL positive | ESBL negative |
|---|
| DM | 22 (11.83) | 4 (2.63) | 14 (8.3) | 14 (7.7) |
| HIV Positive | 4 (2.15) | 1 (0.66) | 0 (0) | 1 (0.6) |
| Low Birth Weight | 3 (1.61) | 0 (0) | 0 (0) | 6 (3.3) |
| Respiratory Disease | 4 (2.15) | 2 (1.32) | 6 (3.6) | 7 (3.9) |
| Neurological Disease | 11 (5.91) | 0 (0) | 2 (1.2) | 5 (2.8) |
| Cardiac Disease | 10 (5.38) | 0 (0) | 2 (1.2) | 2 (1.1) |
| Chronic Liver Disease | 2 (1.08) | 0 (0) | 0 (0) | 4 (2.2) |
| Haematological Disease | 34 (18.28) | 2 (1.32) | 9 (5.3) | 17 (9.4) |
| Malignancy | 13 (6.99) | 0 (0) | 7 (4.1) | 12 (6.6) |
| Ventilator | 15 (8.06) | 1 (0.66) | 21 (12.4) | 26 (14.4) |
| Surgery | 115 (61.83) | 6 (3.95) | 44 (26.0) | 52 (28.7) |
| Dialysis | 3 (1.61) | 0 (0) | 2 (1.2) | 5 (2.8) |
| Central venous catheter | 3 (1.61) | 0 (0) | 0 (0) | 4 (2.2) |
| Urinary catheter | 109 (58.60) | 8 (5.26) | 52 (30.8) | 71 (39.2) |
Only 4 isolates were positive by the MBL E-test (all these were ESBL producers). Only 2 isolates showed NDM-1 production (one was strongly positive and one was weakly positive) [Table/Fig-9]. [Table/Fig-10] shows the characteristics of MBL and NDM-1 positive isolates.
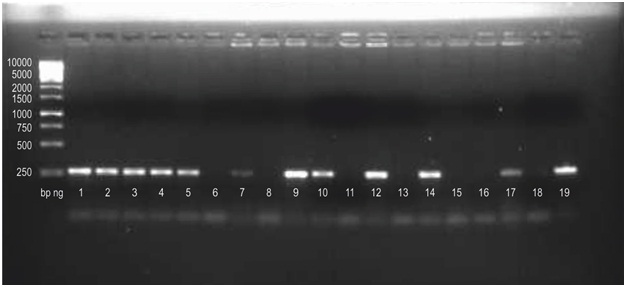
Gel picture of NDM-1 PCR results
bp ng is a molecular weight marker. Last lane (19) is NDM-1 plasmid (positive control). Lane nos. 1,2,3,4,5,9,10.12 and 14 are strongly positive, 7 and 17 are weakly positive, 6,8,11,13,15,16 and 18 are negative. (Lane nos. 1, 6 and 7 represent E. coli. rest are Klebsiella)
Characteristics of MBL producing and NDM-1 positive isolates
| No | Specimen | Admitting Ward | Age Group | Sex | Co-morbidity | Type of Infection | ESBL | NDM-1 |
|---|
| E. coli |
| 1 | Urine | Surgery | >5y - 10y | F | Urinary catheter | HA | Positive | Strongly positive |
| 2 | Body fluid | Surgery | >0d - 28d | F | Surgery | HA | Positive | Weakly positive |
| 3 | Urine | Medicine | >10y - 20y | F | | HA | Positive | Negative |
| 4 | Female genital tract specimen | Surgery | >20y - 30y | F | Surgery | HA | Positive | Not tested |
| Klebsiella spp. |
| 1 | Blood | Surgery | >50 - 60y | F | | HA | Positive | Strongly positive |
| 2 | Blood | Surgery | >60y - 70y | F | Surgery, Ventilator, Urinary catheter | HA | Positive | Strongly positive |
| 3 | Pus | Surgery | >30y - 40y | F | Surgery, Urinary catheter, Haematological disease | HA | Positive | Strongly positive |
| 4 | Respiratory secretion | ICU/Post-op | >28d - 1y | M | Ventilator, Urinary catheter | HA | Positive | Strongly positive |
| 5 | Respiratory secretion | ICU/Post-op | >1y - 5y | M | Surgery, Ventilator, Urinary catheter | HA | Positive | Strongly positive |
| 6 | Respiratory secretion | ICU/Post-op | >20y - 30y | F | Ventilator, Urinary catheter, Diabetes mellitus | HA | Positive | Strongly positive |
| 7 | Respiratory secretion | ICU/Post-op | >40y - 50y | F | Ventilator, Urinary catheter, Haematological disease | HA | Positive | Strongly positive |
| 8 | Respiratory secretion | ICU/Post-op | >20y - 30y | F | Ventilator, Urinary catheter | HA | Positive | Strongly positive |
| 9 | Blood | ICU/Post-op | >0d - 28d | M | Ventilator, Urinary catheter | CA | Positive | Weakly positive |
| 10 | Pus | Surgery | >20y - 30y | F | Surgery, Urinary catheter | CA | Positive | Negative |
| 11 | Pus | Surgery | >20y - 30y | M | Surgery, Urinary catheter, Neurological disease | HA | Positive | Negative |
| 12 | Respiratory secretion | ICU/Post-op | >0d - 28d | M | | HA | Positive | Negative |
| 13 | Respiratory secretion | ICU/Post-op | >0d - 28d | M | Ventilator, Urinary catheter | HA | Positive | Negative |
| 14 | Urine | ICU/Post-op | >20y - 30y | F | Surgery, Urinary catheter | HA | Positive | Negative |
| 15 | Urine | Surgery | >10y - 20y | F | Urinary catheter | HA | Positive | Negative |
| 16 | Female genital tract specimen | Surgery | >30y - 40y | F | | CA | Negative | Not tested |
| 17 | Pus | Medicine | >50y-60y | M | Diabetes Mellitus | CA | Negative | Not tested |
| 18 | Pus | Surgery | >20y - 30y | F | Surgery, Urinary catheter | HA | Positive | Not tested |
| 19 | Respiratory secretion | ICU/Post-op | >28d - 1y | F | Ventilator, Urinary catheter | HA | Positive | Not tested |
| 20 | Urine | ICU/Post-op | >60y-70y | M | Ventilator, Urinary catheter | HA | Negative | Not tested |
| 21 | Urine | ICU/Post-op | >30y - 40y | F | | HA | Negative | Not tested |
Klebsiella spp.: 169 isolates positive for ESBL production by E-test were received from 166 patients. Two isolates were of E. coli.
Female preponderance (54.8%) was seen. Amongst males, 21.3% each were in the age group of >0-28 days and >28 days-1 year followed by 12% from the age group of >20-30 years. Among the females, 33% isolates were from the age group >20-30 years followed by 14.3% from the age group >30-40 years [Table/Fig-1].
In males, 32.1% ESBL producing Klebsiella spp. isolates were obtained from pus followed by 26.9% from respiratory secretions and17.9% from urine. In females, the frequency of isolation was maximum for urine (42.9%) followed by pus (24.2%) [Table/Fig-2]. The difference in frequency of isolation between males and females was statistically significant (p<0.01) except for pus, blood and body fluids (p>0.05).
[Table/Fig-3] shows the distribution of number of ESBL producing Klebsiella spp. isolates in relation to the duration of stay of the patient in the hospital prior to collection of clinical sample. Both the K. oxytoca strains were isolated from patients with stay <48 hours. Therefore, majority of the infections were hospital acquired [Table/Fig-4].
Upon correlating with the admitting wards, significantly higher numbers were received from surgical wards (52.1%) as compared to medicine wards (28.4%) and ICU and postoperative wards (19.5%) (p<0.0001) [Table/Fig-5]. Both the K. oxytoca isolates were received from surgical wards.
Irrespective of type of specimen, the ESBL producing isolates showed high levels of resistance to cephalosporins, fluoroquinolones, monobactam, tetracycline and penicillin but low levels to carbapenems [Table/Fig-11].
Antimicrobial resistance of Klebsiella spp. strains isolated from different specimens
| Antibiotic | Blood(n=15) | BodyFluids (n=9) | Female GenitalTract Specimen(n=32) | Pus(n=43) | RespiratorySecretions(n=14) | Stool(n=2) | Urine(n=77) | TotalIsolates(n=192) |
|---|
| Amikacin | 10 (47.6) | 1 (33.3) | 2 (16.7) | 13 (27.7) | 12 (40.0) | 2 (66.7) | 13 (24.5) | 53 (31.4) |
| Ampicillin | 21 (100.0) | 2 (66.7) | 11 (91.7) | 45 (95.7) | 30 (100.0) | 3 (100.0) | 52 (98.1) | 164 (97.0) |
| Aztreonam | 21 (100.0) | 3 (100.0) | 11 (91.7) | 47 (100.0) | 28 (93.3) | 3 (100.0) | 53 (100.0) | 166 (98.2) |
| Cefazolin | 21 (100.0) | 3 (100.0) | 11 (91.7) | 47 (100.0) | 30 (100.0) | 3 (100.0) | 53 (100.0) | 168 (99.4) |
| Cefotaxime | 21 (100.0) | 3 (100.0) | 11 (91.7) | 47 (100.0) | 30 (100.0) | 3 (100.0) | 53 (100.0) | 168 (99.4) |
| Ceftazidime | 21 (100.0) | 3 (100.0) | 11 (91.7) | 47 (100.0) | 30 (100.0) | 3 (100.0) | 53 (100.0) | 168 (99.4) |
| Ciprofloxacin | 12 (57.1) | 1 (33.3) | 9 (75.0) | 36 (76.6) | 20 (66.7) | 2 (66.7) | 37 (69.8) | 117 (69.2) |
| Cotrimoxazole | 17 (81.0) | 2 (66.7) | 10 (83.3) | 46 (97.9) | 24 (80.0) | 2 (66.7) | 48 (90.6) | 149 (88.2) |
| Ertapenem | 4 (19.0) | 0 (0) | 1 (8.3) | 10 (21.3) | 6 (20.0) | 1 (33.3) | 7 (13.2) | 29 (17.2) |
| Gatifloxacin | 8 (38.1) | 1 (33.3) | 8 (66.7) | 31 (66.0) | 16 (53.3) | 3 (100.0) | 31 (58.5) | 98 (58.0) |
| Imipenem | 2 (9.5) | 0 (0) | 1 (8.3) | 6 (12.8) | 2 (6.7) | 0 (0) | 4 (7.5) | 15 (8.9) |
| Norfloxacin | 13 (61.9) | 1 (33.3) | 8 (66.7) | 33 (70.2) | 19 (63.3) | 3 (100.0) | 36 (67.9) | 113 (66.9) |
| Tetracycline | 19 (90.5) | 2 (66.7) | 11 (91.7) | 38 (80.9) | 23 (76.7) | 2 (66.7) | 42 (79.2) | 137 (81.1) |
In patients infected with ESBL producers, penicillins, aminoglycosides and cephalosporins were prescribed upto 7 days prior to sending the sample for investigation [Table/Fig-7] while relatively fewer patients had received antibiotic beyond 7 days and the difference was statistically significant (p<0.0001). No significant difference was observed between ESBL producing and non-producing Klebsiella isolates when correlated with co-morbidities and other risk factors [Table/Fig-8].
Twenty one isolates were positive by the MBL E-test (17 were also ESBL producers). Eight isolates were strongly positive for NDM-1 production while 1 was weakly positive [Table/Fig-9]. [Table/Fig-10] shows the characteristics of MBL and NDM-1 positive isolates.
Discussion
Our study detected high incidence of ESBL production amongst E. coli and Klebsiella spp. although incidence of MBL production was not very high.
E. coli
The present study revealed female preponderance (65.1%), with significantly higher isolates from males in >28 days - 1 year age group and in females > 20 - 30 years. Rodriguez-Bano et al., also found female preponderance (57%) but the median age was 70 years (age range, 15 to 92 years) [11]. However, the study done by Lautenbach et al., showed male preponderance in the median age of 54 years (17-80 years) [12].
Similar to our study, Lautenbach et al., found specimens from urinary tract (51.5%), wound (15.2%), CVP lines (12.1%), respiratory (9.1%) and abdomen (3%) as sites of infection [12]. Rodriguez-Bano et al., isolated ESBL producing E. coli from urine (92%) and blood (12%) [11].
In contrast to our study, Lautenbach et al., observed that ESBL positive patients were more likely to have nosocomial infection (97%) and longer hospitalization prior to infection (median 11 days) and did not find any significant difference when hospital locations of case and control patients were compared [12].
Overall high levels of resistance to cephalosporins, monobactam, penicillin, fluoroquinolones and tetracycline (>88%) was seen but low levels to carbapenems and aminoglycosides (<25%) (p< 0.0001). This finding was in conformity with Shobha et al., who detected resistance of ESBL producing E. coli as 0% for imipenem, 11.5% for amikacin, 70% for gentamicin, 58% for trimethoprim-sulfamethoxazole, 93.4% for ciprofloxacin, 90% for norfloxacin and 93.4% for nalidixic acid [13]. Similarly Chaudhuri et al., detected very low resistance levels to imipenem (3%) and ertapenem (5%), amikacin (15%) and piperacillin-tazobactam (24%) [14]. Rodriguez-Bano et al., detected low resistant levels to imipenem (0%), amikacin (4%), gentamicin (26%) and high resistance levels to ciprofloxacin (78%), cotrimoxazole (71%) and amoxicillin-clavulanate (52%) [11]. Similarly Jitsurong et al., demonstrated high resistance levels to ampicillin (100%), ceftazidime and cefotaxime (66.7% each) and cotrimoxazole (100%) and low resistance levels to amikacin and imipenem (0%) [15].
With respect to co-morbidities and other variables in present study, Lautenbach et al., also observed that ESBL positive patients were more likely to have urinary catheter (55%) or central venous catheter (58%) in place, less likely to have malignant disease (12%) and more likely to have renal insufficiency (36%) and diabetes mellitus (36%), had significant greater prior cumulative antibiotic exposure including extended-spectrum cephalosporins, fluoroquinolones, aminoglycosides, cotrimoxazole, vancomycin and metronidazole [12]. Rodriguez-Bano et al., observed that previous antimicrobial agent use (67%) especially use of fluoroquinolones (41%), diabetes mellitus (41%), neoplasia (12%), respiratory disease (10%), chronic liver disease (2%), presence of urinary catheter (22%), surgery (8%), old age and male gender were frequently associated with ESBL-producing E. coli infection [11].
In the present study, amongst the MBL producing strains, one each was isolated from body fluid (NDM-1 positive) and female genital tract specimen and two from urine (one was NDM-1 positive). All were females, 3 were admitted in surgical wards (including both NDM-1 isolates) and 1 in medicine ward, all had hospital acquired infections. NDM-1 positive isolates patients belonged to age groups >5-10 year and >0-28 days and underwent surgery and required urinary catheter. This was in contrast to the finding of Deshpande et al., who isolated 9 MBL (NDM-1) positive E. coli from respiratory secretion (1), blood (2) and urine (6) and 7 samples were from wards while 2 from ICU [16], and Chakraborty et al., who observed that MBL positive isolates were mainly from male patients in the old age group (61-80 years) and 54.16% patients suffered from diabetes mellitus [17]. However, Kumarasamy et al., isolated NDM-1 producing E. coli primarily from community acquired urinary tract infections, pneumonia and blood stream infections. The age range was 4-66 years with a mean of 36 years and a female to male ratio of about two to one [18].
Klebsiella spp.
The present study showed female preponderance (54.8%) with significantly higher isolates from males in the age group of >0 day - 1 year and in females in >20-30 years of age group. Marra et al., did not find any significant age or gender difference between ESBL producing and non-producing K. pneumoniae [19]. Lautenbach et al., observed ESBL producers to be significantly younger and more frequently males [12].
Similar to our study, Lautenbach et al., found specimen for urinary tract (51.5%), wound (15.2%), CVP lines (12.1%), respiratory (9.1%) and abdominal (3%) as sites of infection and observed that ESBL positive patients were more likely to have nosocomial infection (97%) and longer hospitalization prior to infection (median 11 days) and did not find any significant difference when hospital locations of case and control patients were compared [12].
Both Marra et al., and Mathur et al., found the proportion of ESBL positive isolates to be highest from ICU in contrast to our study [19,20].
High levels of resistance to cephalosporins, fluoroquinolones, monobactam, tetracycline and penicillin but low levels to carbapenems was seen in this study which was in conformity with Shobha et al., who detected antibiotic resistance of ESBL-producing Klebsiella spp. as 0% for imipenem, 14% for amikacin, 69% for gentamicin, 71% for trimethoprim-sulfamethoxazole, 90% for ciprofloxacin, 94% for norfloxacin and 94% for nalidixic acid [13]. Similarly Chaudhuri et al., detected low levels of resistance to imipenem (6%) and ertapenem (20%), amikacin (26%) and piperacillin-tazobactam (41%) [14]. Jitsurong et al., demonstrated high levels of resistance to ampicillin (100%), ceftazidime (100%), cefotaxime (56.3%) and cotrimoxazole (81.3%) and low levels of resistance to amikacin (16.8%) and imipenem (0%) [15].
In the present study, penicillins, aminoglycosides and cephalosporins were prescribed upto 7 days in patients infected with ESBL producing Klebsiella prior to sending the sample for investigation (p<0.0001). No significant difference was observed between ESBL producing and non-producing Klebsiella isolates when correlated with co-morbidities and other risk factors. However, the need for ventilatory support and central venous catheters was more in ESBL producing Klebsiella strains as reported by Marra et al., [19]. Lautenbach et al., observed that ESBL positive patients had urinary catheter (55%) or central venous catheter (58%) in place, were less likely to have malignant disease (12%) and more likely to have renal insufficiency (36%) and diabetes mellitus (36%), had significant greater prior cumulative antibiotic exposure including to extended-spectrum cephalosporins, fluoroquinolones, aminoglycosides, cotrimoxazole, vancomycin and metronidazole [12].
The 21 MBL producing isolates were mainly from females (61.9%) (p<0.001) isolated from respiratory secretions (8), pus (5), urine (4), blood (3) and female genital tract specimens (1). The 9 NDM-1 positive isolates were mainly from females, obtained from pus (1), blood (3) and respiratory secretions (5) with age range from 0 days to 70 years. This was similar to the finding of Deshpande et al., who isolated 10 MBL (NDM-1) positive K. pneumoniae obtained from blood, pus and swab (1 each), urine (3) and respiratory secretions (4) [16] and Chakraborty et al., who observed that MBL positive isolates were mainly from male patients in the old age group (61-80 years) and 54.16% patients suffered from diabetes mellitus [17]. Kumarasamy et al., detected 21.3% of isolates as MBL producing K. pneumoniae from community acquired urinary tract infections, pneumonia and blood-stream infections. The age range was 4-66 years (mean 36 years) and female to male ratio of about two to one [16].
In the present study, patients with MBL positive (including NDM-1 positive) isolates were mainly admitted to ICU/postoperative wards similar to Deshpande et al., [16]. We observed that 76.2% of MBL positive patients had urinary catheter in-situ, 47.6% required ventilatory support, 33.3% underwent surgery, 9.5% had diabetes mellitus, 9.5% haematological diseases and 4.8% neurological disease. The respective percentages of NDM-1 positive isolates was 88.9%, 77.8%, 33.3%, 11.1%, 22.2% and 0%. Cagnacci et al., observed that all patients infected with MBL producing K. pneumoniae had an underlying disease, had undergone surgery (55.6%), had malignancy (22.2%) and all had nosocomial infections [21].
Conclusion
ESBL and MBL production is now a significant problem in hospitalised patients globally and have a significant impact on several important clinical outcomes. The present study identified prior antibiotic use, surgery, haematological disease, diabetes mellitus, neurological disease, respiratory disease, urinary catheterisation and mechanical ventilation as important risk factors associated with ESBL and MBL producing organisms. Risk factors for infections due to these should be clearly identified so that effective strategies are developed to reduce spread of these infections and to optimise antibiotic use.