Laparoscopic Excision of Retroperitoneal Schwannoma
J S Rajkumar1, Deepa Ganesh2, J R Anirudh3, S Akbar4, C M Kishore5
1 Chairman & Advanced Laparoscopic Surgeon, Life Line RIGID Hospitals Pvt. Ltd., Kilpauk, Chennai, India.
2 Consultant Laparoscopic Surgeon, Life Line RIGID Hospitals Pvt. Ltd., Kilpauk, Chennai, India.
3 Assistant Surgeon, Life Line RIGID Hospitals Pvt. Ltd., Kilpauk, Chennai, India.
4 Assistant Surgeon, Life Line RIGID Hospitals Pvt. Ltd., Kilpauk, Chennai, India.
5 Consultant Laparoscopic Surgeon, Life Line RIGID Hospitals Pvt. Ltd., Kilpauk, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepa Ganesh, Life Line RIGID Hospitals Pvt. Ltd., No: 47/3, New Avadi Road, Kilpauk, Chennai- 600 010, India.
E-mail: drdeepa@gmail.com
Schwannomas are tumours that arise from the myelin sheath of the nerves. A very unusual location for schwannoma is the retro peritoneal areas (less than 2%). We present herewith a patient who had a 4x5cm Schwannoma arising from the nerve root of L2 on the right side, which presented as a lump in the psoas major muscle. This was treated by total laparoscopic excision after splitting open the psoas major. In the published english medical literature we could find only 16 cases of laparoscopic resection of retroperitoneal schwannoma and we believe ours to be the first case that was done through a psoas muscle split technique. Technical and histopathological details are discussed elaborately in this article.
Laparoscopy, Psoas muscle, Retroperitoneum, Schwannoma
Case Report
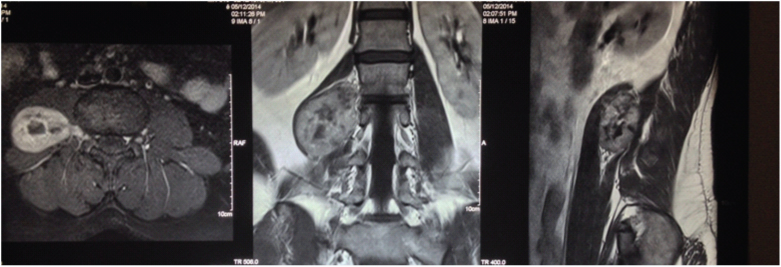
A 30-year-old male presented at our hospital with pain in the front of the right thigh, for which he had undergone a series of investigations by the neurologists. MRI [Table/Fig-1] showed a large lump within the right psoas muscle, in close relationship to L2 nerve root, and at a level that was 2cm below the lower pole of the right kidney. There were areas of degeneration in the central aspect of the tumour, which showed medial intracanalicular extension along the root of L2. The radiological appearance was highly suggestive of schwannoma with an extension to L2 nerve root. The anatomical position of the schwannoma was intra-psoas. After detailed discussion with the patient about a possible need of open surgery and probability of injury to the lumbar sacral plexus in close relation to the tumour, we proceeded with laparoscopic surgery.
MRI showing a large lump within the right psoas muscle, in close relationship to L2 nerve root, and at a level that was 2cm below the lower pole of the right kidney
Technique
Patient was placed in supine position with legs split, surgeon stood between the legs of the patient and the camera person was to the left side of the surgeon, first assistant to the right side. We decided to proceed with an intraperitoneal approach to the retroperitoneum, with medial colonic reflection. Initially it was accessed through the suprapubic port with the left hand working port in the right iliac fossa and the right hand working port in the left iliac fossa, augmented by a 10mm port through the umbilicus that was used initially for right hand working, and was later used for the telescope.
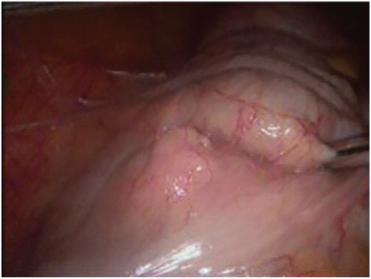
Initially the terminal ileum, the appendix, and the caecum were mobilized and lifted off the retroperitoneum. Then the port in the left iliac fossa was used to grasp these structures and reflect them medially and right hand working port through the umbilicus was used to continue the right paracolic dissection upto to the hepatic flexure and then to turn medially in order to expose the complete retroperitoneum [Table/Fig-2].
Medial reflection of the ascending colon
The anterior surface of the Gerota’s fascia was completely exposed upto the level of the adrenal gland. The right ureter was identified and traced throughout its course [Table/Fig-3].
Dissection of right ureter
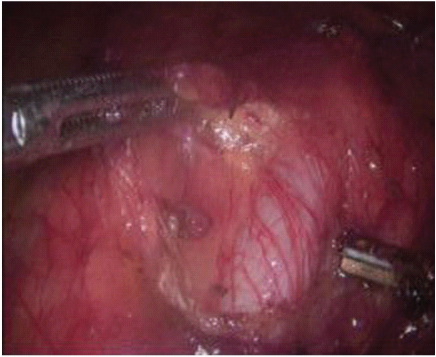
Progressive medial mobilization of the right colon allowed us to identify and preserve the duodenum and the complete Inferia Vena Cava (IVC). At this stage the psoas and the ilio-psoas tendon were both seen clearly. By correlation with the MRI we were able to then do a psoas split (a longitudinal 5cm muscle split of the psoas major lateral to genito-femoral nerve which was identified and preserved).
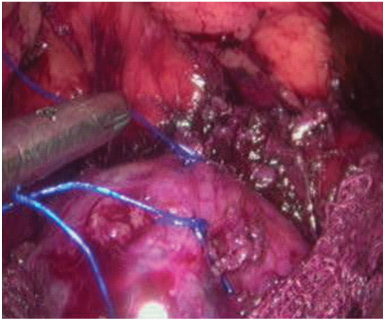
Wide longitudinal splitting of psoas major helps to expose the anterior surface of the capsule of the tumour [Table/Fig-4]. By careful dissection just outside the capsule, and by coagulating and dividing all the feeding vessels to and from the tumour, a plane was developed all around. We found the suture traction technique to be useful, and would like to recommend it too. Sutures were taken on the capsule of the tumour with 2-0 polypropolene which were held with the needle holder for retraction to expose further the surface and edges of the tumour [Table/Fig-5].
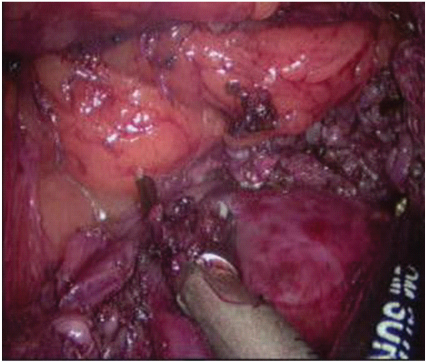
Suture traction technique
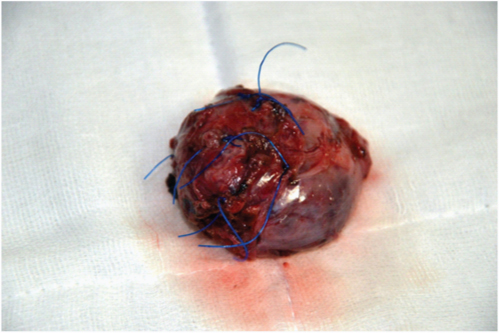
The medial dissection was kept towards the end as the MRI had shown some intracanalicular extension. After the lateral superior inferior and deep dissection had been completed, suction dissection was performed and the tumour was gently eased out of its intracanalicular extension. After the tumour was completely dissected out it was placed in an indigenous plastic bag with a silk purse string and removed [Table/Fig-6] via a 3cm extension of the umbilical port, along with the gauze swabs that were put in for pressure haemostasis.
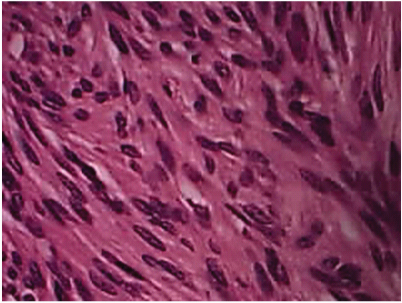
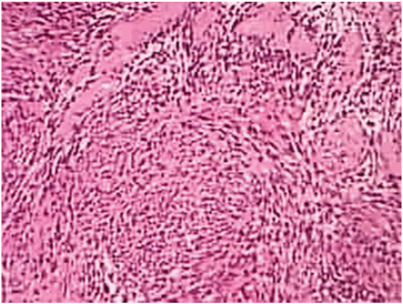
Operative time was 165 minutes, and the operating blood loss was about 20ml. After closed suction drainage of the area, the caecum and the ascending colon were repositioned on to the right side of the abdomen. The patient had a completely uneventful postoperative period, except for a little pain down the right thigh towards the lesser trochanter, possibly explicable by a little post operative ooze at the site of the psoas major. Histopathology showed capsulated lesion composed of schwann cells, fibroblasts, neural fibres with myxoid areas and the characteristic Veracoy bodies [Table/Fig-7,8].
Discussion
Primary retroperitoneal schwannoma remain very rare nerve sheath tumours [1–3]. Otherwise known as Neurilemmomas, these arise from the myelin sheath of the nerves [4]. Schwannomas are diffusely S-100 positive, CD34 & CD117 negative, neuron specific enolase positive tumours that arise from the nerve sheath [5]. A variety of schwannoma often found retroperitoneally is the so called “Ancient” schwannoma that have much cystic degeneration due to growth outgrowing the blood supply. Characteristic histopathological change that are found, are the presence of spindle shape cells with the myxoid background appearance, with areas of dense cellular infiltration (Antoni A) and less cells and more abundant myxoid cytoplasm (Antoni B) [3,4].
Schwannomas in the retroperitoneum are often malignant (0.3 to 3.2%). Here, they pose certain special difficulties, especially due to their close relationship to great vessels and to the bones (transverse processes of the vertebras [6–9]. Compared to the usual locations in the flexor aspect of the arm and the appendicular skeleton, retroperitoneal schwannomas have a slightly higher incidence of malignancy. Laparoscopic excision of schwannomas was once deprecated against, on the grounds of possible injuries to surrounding structures. But better optics and increasing skills of tissue handling have rendered this once difficult task much simpler, and few published reports are available of laparoscopic excision [2,3,8–12].
Review of the literature showed no report of intra-psoas schwannoma that was taken out laparoscopically [13–17]. We found that the following steps were critical to a successful laparoscopic outcome: (1) Anterior approach with right colonic mobilization to the medial side. This allowed us to expose the ureter and the genito-fermoral nerve, which we traced back to its roots. This permitted us to identify the upper medial tip of the tumour with its intracanlicuar extension, (2) Looping the right ureter and the genito-femoral nerve permitted us to operate on the fibers of the psoas and reach the tumour, (3) The 5cm psoas spilt allowed us to reach the capsule of the schwannoma. The distracted fibers were later closed with interrupted suturesm, (4) Multiple sutures with polypropylene, on the capsule of the tumour were grasped sequentially by the needle holder. The resultant traction opened up a relatively avascular plane close to the capsule so that the dissection was proceeded with, and the retroperitoneal veins were undisturbed. The combination of all these factors engendered an excellent clinical outcome.
Conclusion
This paper has been published with two objectives. The first is to reiterate the trend of using the laparoscopic approach to tackle retroperitoneal tumours. The open approach is quite traumatic, and will gradually be used as a salvage option if minimal access surgery is unsuccessful. The second is to highlight two innovations that we have introduced in this operation, viz, the psoas spilt maneuver to reach the deeply located schwannoma, and the suture traction technique to dissect around the margin of the tumour. To our knowledge, these two techniques have not yet been described in the literature pertaining to excision of retroperitoneal tumours. Although a handful of papers have already established endoscopic schwannoma excision, we hope that with the help of advancing technologies, this is soon registered as the treatment of choice.
[1]. Sahoo MR, Anil Kumar T, Retroperitoneal neurilemmoma with cystic degeneration mimicking hydatid cystIJCRI 2013 10:382-CR-11. [Google Scholar]
[2]. Yoshino T, Yoneda K, Laparoscopic Resection of a Retroperitoneal Ancient schwannoma: a case report and review of the literatureAnticancer Research 2008 28(5B):2889-91. [Google Scholar]
[3]. Narasimha A, Harendra Kumar ML, Kalyani R, Retroperitoneal cystic shcwannoma: A case report with review of literatureJ Cytol 2010 27(4):136-39. [Google Scholar]
[4]. Cho YH, Kim DH, Lee SH, Laparoscopic resection of a 12cm sized retroperitoneal schwannoma adjacent to retroperitoneal vital vessels: are large retroperitoneal schwannomas not suitable for the laparoscopic approach?J Korean Surg Soc 2010 78(4):253-57. [Google Scholar]
[5]. Bindal V, Bhatia P, Kalhan S, Robot-assisted excision of a large retroperitoneal schwannomaJSLS 2014 18:150-54. [Google Scholar]
[6]. Cury J, Coelho RF, Retroperitoneal schwannoma : case series and literature reviewClinics (Sao Paulo) 2007 62(3):359-62. [Google Scholar]
[7]. Gorgun M, Sezer TO, Laparoscopic resection of retroperitoneal schwannoma near the inferior venaAnnales de Chirurgie Vasculaire 2010 24(4):601.e1-601.e4. [Google Scholar]
[8]. Sakalauskaite M, Stanaitis J, Cepkus S, Retroperitoneal giant schwannoma eroding lumbal vertebra: A case report with a literature reviewCentral European Journal of Medicine 2008 3(2):233-44. [Google Scholar]
[9]. Ahn KS, Han HS, Yoon YS, Laparoscopic resection of nonadrenal retroperitoneal tumoursArch Surg 2011 146(2):162-67. [Google Scholar]
[10]. Akihito N, Wataru A, Laparoscopic resection of a retroperitoneal schwannomaSurgical laparoscopy, endoscopy & percutaneous technique 1999 9(4):306 [Google Scholar]
[11]. Rao W, Xiu WG, Laparoscopic resection of a retroperitoneal schwannoma adherent to vital vesselsSurgical Laparoscopy, Endoscopy & Percutaneous Techniques 2009 19(1):e21-3. [Google Scholar]
[12]. Wakabayashi G, Laparoscopic excision of retroperitoneal tumours: Report of three casesSurgery Today 2010 40(2):176-80. [Google Scholar]
[13]. Melvin WS, Laparoscopic resection of a pelvic schwannomaSurgical Laparoscopy & Endoscopy 1996 11(2):88-91. [Google Scholar]
[14]. Seo IY, Boldbaatr Y, Choi KH, Laparoscopic resection of ancient schwannoma embedded in the psoas muscleSurgical Laparoscopy, Edoscopy & Percutaneous Techniques 2011 21(6):e336-38. [Google Scholar]
[15]. Kameyama N, Tomita M, Mitsuhashi H, Single port transumbilical laparoscopic excision of retroperitoneal schwannoma mimicking a nonfunctional endocrine tumour in the body of the pancreas – a case reportSURG INNOV 2013 20(6):NP30-34. [Google Scholar]
[16]. Zhipeng Z, Dianrong X, Laparoscopic surgery for primary retroperitoneal tumours: a single institution experience of 14 casesSurgical laparoscopy, Edoscopy & Percutaneous Techniques 2010 20(6):399-403. [Google Scholar]
[17]. Misra MC, Bhattacharjee HK, Hemal AK, Bansal VK, Laparoscopic management of rare retroperitoneal tumoursSurgical laparoscopy, Edoscopy & Percutaneous Techniques 2010 20(3):e117-22. [Google Scholar]