A Rare Case of Intra- Abdominal Bronchogenic Cyst- A Case Report
Munish Trehan1, Sanjeev Singla2, Jaspal Singh3, Nikhil Garg4, Anuj Mahajan5
1 Assistant Professor, Department of Surgery, DMCH, Ludhiana, Punjab, India.
2 Professor, Department of Surgery, DMCH, Ludhiana, Punjab, India.
3 Professor and Head, Department of Surgery, DMCH, Ludhiana, Punjab, India.
4 Resident, Department of Surgery, DMCH, Ludhiana, Punjab, India.
5 Resident, Department of Surgery, DMCH, Ludhiana, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nikhil Garg, C/o Dr. Bimal Garg, Near Clock Tower, Faridkot- 151203, Punjab, India. E-mail : Nikhilgarg9490@gmail.com
Bronchogenic cysts are developmental foregut anomalies usually located in the mediastinum. A 90% of the bronchogenic cysts occur in the posterior aspect of superior mediastinum. Retroperitoneal location of a bronchogenic cyst is rare. We report a rare case of intra abdominal bronchogenic cyst. A CT scan was done for a 34-year-old female who presented with complains of heaviness in the right flank. CT scan revealed a large cyst of 10 x 6 cm in the right hypochondrium. Cyst was removed laparoscopically and the histopathology revealed a bronchogenic cyst.
Laparoscopically, Retroperitoneal cyst, Right hypochondrium
Case Report
A 34-year-old female presented to the Department of Surgery in Dayanand Medical College and Hospital which is a tertiary care centre in Ludhiana, Punjab with complaints of heaviness in right flank since 3 months. There was no history of abdominal pain, fever or vomiting. Physical examination revealed an intra-abdominal mass in the right hypochondrium with well defined margins, soft consistency and no mobility with respiration. USG and CECT revealed a cystic lesion of size 10 cm x 6 cm in the right hypochondrium with no evidence of calcification or septations [Table/Fig-1].
CECT abdomen showing a large cyst in the abdomen

After obtaining an informed consent from the patient laparoscopic exploration of the patient was performed. Intraoperatively, a large cyst was found in right retroperitoneum. Ascending colon and transverse colon was pushed medially. Anterolaterally, the cyst was attached to the abdominal wall. Posteromedially the cyst was attached to the psoas and colon. Cyst was aspirated which consisted of a yellow coloured serous fluid and the cyst wall was separated from the surrounding structures [Table/Fig-2]. The total operative time was about 80 minutes and there was no intraoperative or postoperative complication and the patient was discharged on the fifth postoperative day. The cyst was sent for histopathological examination. The lining of the cyst was columnar. In the wall, smooth muscle and respiratory-type mucous glands were seen [Table/Fig-3,4]. The final pathological diagnosis was bronchogenic cyst. The patient was completely asymptomatic on follow up 2 weeks after the surgery.
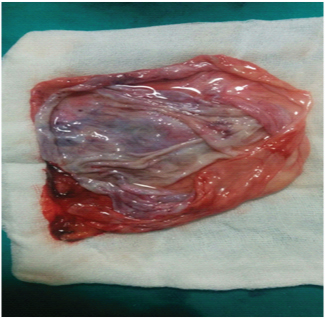
Cut section of the cyst postoperatively
Histopathology of the resected cyst wall (H&E, orig. magn, X400)

Histopathology of the resected cyst wall (H&E, orig magn X10)

Discussion
An accessory lung bud from the primitive foregut is mostly the site of origin of a bronchogenic cyst. Caudal migration with the oesophagous occurs later due to which they are mostly located in the posterior mediastinum with an attatchment to the tracheobronchial tree or to the oesophagus [1–3]. Pericardium, skin and abdomen are rare sites for occurrence of bronchogenic cysts. According to Coselli et al., if complete separation occurs a cyst may migrate to other unusual locations [4].
Subdiaphragmatic bronchogenic cysts are very rare. Although their mechanism of development is unknown, Sumiyoshi et al., proposed that early in embryonic life, the pericardioperitoneal canal connects the abdominal and thoracic cavities, and with closure of the pleuroperitoneal membranes, which form the future diaphragm, abnormal lung buds could be pinched off and trapped in the abdomen [5].
Due to the small size most of these cysts are diagnosed incidentally. Epigastric pain or left upper quadrant discomfort can be the presenting complaint in some cases. Malignant transformation on presentation is rare [6]. Due to lack of common symptoms and specific laboratory parameters, CT scan has a significant diagnostic role. Cyst contents can be evaluated with a CT scan to differentiate it from retroperitoneal cystic lymphangioma, hematoma or an abscess. Mesothelioma of the peritoneum, pearly tuberclousis or ovarian cysts is the commonly found intra abdominal cystic lesions. A large mesenteric cyst may also have the same presentation. CT abdomen is the investigation of choice for a final diagnosis.
Most of the cysts that are discovered incidentally are benign. If there are symptoms present due to the cyst, it should be resected. In case of presence of a diagnostic uncertainty surgery should be the treatment of choice. Complications such as bleeding, ulceration or obstruction may occur which warrants a surgical resection than observation [7]. Laparoscopic approach is a feasible and safe procedure for this pathology up to date [8]. Bronchogenic cysts must be considered in the differential diagnosis of retroperitoneal cystic lesions inspite of decreased incidence in retroperitoneum [9,10].
Conclusion
Intraabdominal bronchogenic cyst is very rare and retroperitoneal cysts even rarer. We report a rare case of a large retroperitoneal bronchogenic cyst in the right hypochondrium. Complete laparoscopic surgical excision of the cyst was done. Preoperative CT scan is diagnostic and helps to differentiate from other cystic lesions. Symptomatic cysts or cysts whose diagnosis is uncertain should be resected.
[1]. Laberge JM, Puligandla P, Flageole H, Asymptomatic congenital lung malformationsSemin Pediatr Surg 2005 14:16-33. [Google Scholar]
[2]. Chen CC, Bronchogenic cyst in the interatrial septum with a single persistent left superior vena cavaJ Chin Med Assoc 2006 69:89-91. [Google Scholar]
[3]. Ibanez Aguirre J, Marti Cabane J, Bordas Rivas JM, ValentiPonsa C, ErroAzcarate JM, De Simone P, A lump in the neck: cervical bronchogenic cyst mimicking a thyroid noduleMinerva Chir 2006 61:71-72. [Google Scholar]
[4]. Coselli MP, de Ipolyi P, Bloss RS, Diaz RF, Fitzgerald JB, Bron- chogenic cyst above and below the diaphragm: report of eight casesAnn Thorac Surg 1987 44:491-94. [Google Scholar]
[5]. Sumiyoshi K, Shimizu S, Enjoji M, Iwashita A, Kawakami K, Bronchogenic cyst in the abdomenVirchows Arch A Pathol Anat Histopathol 1985 408:93-98. [Google Scholar]
[6]. Sullivan SM, Okada S, Kudo M, Ebihara Y, A retroperitoneal bronchogenic cyst with malignant changePathol Int 1999 49:338-41. [Google Scholar]
[7]. Leepalao M, Wernberg J, Multiple Bronchogenic and Gastroenteric Cysts Arising from the Stomach in a Patient with Abdominal PainCase Reports in Surgery 2015 2015:601491 [Google Scholar]
[8]. Diaz Nieto R, Intraabdominal bronchogenic cystJ Gastrointest Surg 2010 14(4):756-58. [Google Scholar]
[9]. Govaerts K, Eyken PV, Verswijvel G, Speeten KV, A bronchogenic cyst, presenting as a retroperitoneal cystic massRare Tumors 2012 4(1):e13 [Google Scholar]
[10]. Chu P, Hwang TI, Teng T, Lee C, A retroperitoneal bronchogenic cyst successfully treated by laparoscopic surgeryAnn Saudi Med 2007 27:199-200. [Google Scholar]