Background
Adverse pregnancy outcomes are undesirable events occurring during pregnancy and childbirth in mother or child, such as Preterm Low Birth Weight (PLBW) and preeclampsia. There is growing evidence that periodontitis may be a risk factor for preterm birth even after adjusting for known risk factors.
Aim
1. To determine the knowledge and attitude of pregnant females about oral health. 2. To evaluate the oral hygiene practices of pregnant females. 3. To evaluate their awareness regarding effect of oral health on adverse pregnancy outcomes. 4. To assess whether there was any significant difference from their non pregnant counter parts. 5. To evaluate whether their awareness towards dental treatment had increased after conceiving.
Materials and Methods
200 pregnant and 200 non-pregnant women filled up a validated questionnaire which comprised of questions on personal data, oral hygiene knowledge, attitude, oral hygiene practices and their awareness regarding the correlation of oral health to adverse pregnancy outcomes.
Statistical Analysis
Analyses were conducted using SPSS for Windows (version 15.0; SPSS Inc., Chicago, IL, USA).
Results
The results indicate no statistically significant differences in the variables assessed in both the groups, indicating that no further knowledge had been imparted to the women after they conceived. 96% women of both groups (p>0.05) had received no knowledge from the gynaecologist regarding the impact of oral health on pregnancy outcomes. 93.9% of pregnant women, and 89.5% of non pregnant women (p>0.05) did not go for routine dental check-ups. Only 3% of pregnant women were aware of oral health having a correlation with adverse pregnancy outcomes.
Conclusion
In our study, pregnancy did little to change future attitudes to dental care. To provide better oral health care, more knowledge needs to be made available to the pregnant women and the medical community.
Introduction
It has been suggested that periodontal disease during pregnancy could have a causal relationship with low birth weight (LBW) babies and other adverse pregnancy outcomes. Premature delivery implies labour that occurs at fewer than 37 complete weeks of gestation and is generally accompanied by Low Birth Weight <2500 gm [1]. It is important to emphasize that non-specific, general inflammatory mediators induced by periodontal disease are the same ones that play an important role in initiation of labour. In a normal parturition, labour occur when there is an increased level of inflammatory cytokines such as IL-1, TNF-α, and PGE2 in placenta. In case of periodontitis, due to increased bacteraemia there are prematurely raised levels of the inflammatory mediators which are involved in normal parturition, leading to premature rupture of placental membrane causing pre-mature birth [2–4].
Moreover, microbiological data indicate that primary microorganisms, associated with mature plaque and progressing, periodontitis- Bacteriodes forsythus, Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans and Treponema denticola were detected at higher levels in mothers with PLWB babies as compared to normal birth weight (NBW) controls [5–7]. This association has further been proved by finding higher mid-trimester maternal serum antibody levels against these micro-organisms specially Porphyromanas gingivalis and Capnocytophaga [8,9]. Thus it is logically reasonable as well as biologically plausible to hypothesize that periodontal infection contributes to adverse pregnancy outcomes in the form of premature delivery.
Low birth weight is a serious challenge for mother and child health. Perinatal and infant mortality, infant morbidity, mental retardation, and the high cost of special care needed by such children are few of the public health consequences.
In the National Database 2002-2003, approximately around 1,52,000 deliveries were included from 18 centres throughout India over a period of two years. According to the database, amongst the intramural (within the included centres) live births, 14.5% were preterm and out of the total live births, 31.3% were low birth weight infants. Extreme prematurity was a primary cause in approximately 26.3% cases of neonatal deaths. Amongst the extramural live births, 52.1% infants were low birth weight infants and 31.5% were preterm. Prematurity and related complications constitute 19.3% of the share of neonatal deaths. Of much significance is the fact that out of the total LBW stillbirths, 77.7% were preterm LBW infants. This data suggests that along with many other causes, preterm and its associated complications form an important reason for high percentage of total neonatal deaths or stillbirths in the region [10].
Mannem and Chava studied 104 pregnant women residing in Andhra Pradesh, India, by dividing them into two groups {control group (those who had term labour), and case group (those who had preterm labour)}, and measuring their Plaque Index, Bleeding Index and Birth weight of the newborn. They reported a statistically significant difference between the two groups p<0.05), and concluded that there exists a noticeable relationship between periodontal health and duration of pregnancy, and that periodontal disease could be a risk factor for preterm labour. Hence, oral hygiene maintenance should be a part of prenatal care protocol [11].
Ideally, women should begin their pregnancy without gingival and periodontal infection, and they should be educated and motivated to maintain a high level of oral hygiene prior to and throughout pregnancy. Therefore, researchers and health program planners should give increased attention to the oral health needs and behaviour of pregnant women.
Numerous evidence based studies are available which find a positive co- relationship between periodontitis and adverse pregnancy outcomes [2–9]. Offenbacher and colleagues were the first to report data that suggested periodontal diseases could represent a previously unrecognized and clinically significant risk factor for preterm low birth weight in humans [12]. They suggested that maternal periodontal disease could lead to a seven-fold increased risk of delivery of a PLBW infant. Tarannum et al., reported that Indian women who did not receive prenatal periodontal treatment were 3.4 to 4.5 times more likely to deliver infants who were preterm, low birth weight, or both [13]. Radnai et al., reported that women with threatened pre-term delivery and initial localized chronic periodontitis had significantly lower chance of adverse pregnancy outcome if they received periodontal therapy before the 35th gestational week [14].
If we are able to evaluate the knowledge and practices of pregnant women, and compare it with that of non-pregnant women, we can ascertain as to whether there is a significant difference in terms of the same, whether the would-be-mothers were educated regarding the role of oral health in adverse pregnancy outcomes or whether their knowledge and awareness levels remained the same, indicating no extra gain in knowledge after conceiving.
Materials and Methods
Data collection: The present study was designed as questionnaire based survey. After preliminary construction of the questionnaire, it was sent to Dr Alka Sehgal, Associate professor, Department of Obstetrics and Gynaecology, Government Medical College and Hospital, Sector-32 to test its validity, and her suggestions regarding some modifications in the design of some of the questions were taken into account. Pilot study was conducted on 20 pregnant and 20 non pregnant women. These filled questionnaires were used to measure the reliability of the test using Cronbach’s alpha test. The coefficient of reliability was more than 0.7, indicating that the questionnaire is reliable, and meets the purpose of this study. The structured questionnaire was checked for validity by three experts from the field of Gynecology and Periodontology (annexure 1). The questionnaire was verbally explained in the local language to illiterate women and those facing any problem. Written consent was taken from all the participating women. Permission was taken from Medical Superintendants of the Government Hospitals. The ethical clearance for the study was received from Ethical Committee, Panjab University, Chandigarh.
Sample size was estimated based on the results of the pilot study. The mean difference for knowledge score between pregnant and non-pregnant group was 0.93 with a SD of 3.5. Hence sample size was estimated to bee 176 subjects per group at a power of 80 % and confidence interval of 95%. The study was conducted between September 2011 - December 2012 on 200 non-pregnant females (Group A) and 200 pregnant (Group B) females randomly selected amongst expecting mothers and the family members of the expecting mothers visiting the obstetrics and gynaecological departments of Government Medical College and Hospital, Sector-32 and Government Hospital Sector-16, Chandigarh. A computer generated randomisation was utilized for selecting them. Women not willing to participate in the study, having less than 20 teeth in their oral cavity, of <20 years or >50 years of age were excluded from the study.
Statistical Analysis
Discrete categorical data were presented as n (%). For categorical data comparisons were made by Pearson Chi-square test. All statistical tests were two-sided and performed at a significance level of α=0.05. An analysis was conducted using SPSS for Windows (version 15.0; SPSS Inc., Chicago, IL, USA).
Results
We applied factor analysis to the questionnaire. The Kaiser-Meyer- Olkin value (KMO value) was 0.737, and the questions in the questionnaire fell under 6 main subheadings, namely, questions on Socio-demographic background, Oral hygiene habits, Aetiology of dental caries, Signs and symptoms of gum disease, Assessment of awareness of both the groups regarding oral and systemic inter-relationship and Assessment of knowledge regarding correlation of oral health to adverse pregnancy outcomes in pregnant females.
Socio-demographic background: The mean range of age of women was 20-50 years. Respondents’ data has been compiled in [Table/Fig-1], and the variables which showed a statistically significant association with Education in [Table/Fig-2].
Characteristics of the participants
| Characteristics | Pregnant (%) | Non Pregnant (%) |
|---|
| Age group |
| 20-29 yrs | 79% | 43% |
| 30-39 yrs | 20% | 39.5% |
| 40-50 yrs | 1% | 17.5% |
| Education |
| No formal education | 5.5% | 16% |
| Primary school | 14.5% | 24.5% |
| Secondary school | 48.5% | 34% |
| Graduates | 16% | 18.5% |
| Post- Graduates | 15% | 7% |
| Employment Status |
| Self employed | 1% | 9% |
| Government Jobs | 3.5% | 8% |
| Private Jobs | 7% | 14% |
| Housewife | 88.5% | 61.5% |
| Retired and others | 0% | 7.5% |
Variables which showed a statistically significant association with Education (Chi-square test applied)
| Characteristic | No formal education | Primary school | Location | Size | Type | Grade |
|---|
| How often do you think the teeth should be brushed? |
| Pregnant | (n) correct response | 8 | 16 | 70 | 26 | 27 | 0.061 |
| Pregnant | (n) incorrect response | 3 | 13 | 27 | 6 | 4 | |
| Non Pregnant | (n) correct response | 14 | 27 | 35 | 30 | 8 | 0.018 |
| Non Pregnant | (n) incorrect response | 18 | 22 | 33 | 7 | 6 | |
| In your opinion, which is the best method for cleaning the teeth? |
| Pregnant | (n) correct response | 11 | 25 | 95 | 31 | 30 | 0.067 |
| Pregnant | (n) incorrect response | 0 | 4 | 2 | 1 | 1 | |
| Non Pregnant | (n) correct response | 25 | 44 | 65 | 37 | 14 | 0.004 |
| Non Pregnant | (n) incorrect response | 7 | 5 | 3 | 0 | 0 | |
| Which food can lead to dental caries? |
| Pregnant | (n) correct response | 6 | 10 | 55 | 23 | 27 | 0.001 |
| Pregnant | (n) incorrect response | 5 | 19 | 42 | 9 | 4 | |
| Non Pregnant | (n) correct response | 19 | 35 | 50 | 33 | 14 | 0.10 |
| Non Pregnant | (n) incorrect response | 13 | 14 | 18 | 4 | 0 | |
| In your opinion, when teeth start to decay, what is the treatment? |
| Pregnant | (n) correct response | 1 | 6 | 27 | 19 | 26 | 0.000 |
| Pregnant | (n) incorrect response | 10 | 23 | 70 | 13 | 5 | |
| Non Pregnant | (n) correct response | 6 | 16 | 30 | 23 | 12 | 0.000 |
| Non Pregnant | (n) incorrect response | 26 | 33 | 38 | 14 | 2 | |
| What is calculus? |
| Pregnant | (n) correct response | 0 | 3 | 3 | 7 | 6 | 0.005 |
| Pregnant | (n) incorrect response | 11 | 26 | 94 | 25 | 25 | |
| Non Pregnant | (n) correct response | 8 | 9 | 11 | 10 | 3 | 0.683 |
| Non Pregnant | (n) incorrect response | 24 | 40 | 57 | 27 | 11 | |
| Do you think oral health has any role in overall health? |
| Pregnant | (n) correct response | 10 | 19 | 72 | 25 | 28 | 0.141 |
| Pregnant | (n) incorrect response | 1 | 10 | 25 | 7 | 3 | |
| Non Pregnant | (n) correct response | 11 | 20 | 42 | 27 | 12 | 0.001 |
| Non Pregnant | (n) incorrect response | 21 | 29 | 26 | 10 | 2 | |
p ≥ 0.05 indicates Not significant results, p < 0.05 indicates Statistically significant results, p <0.001 indicates Statistically Highly significant results
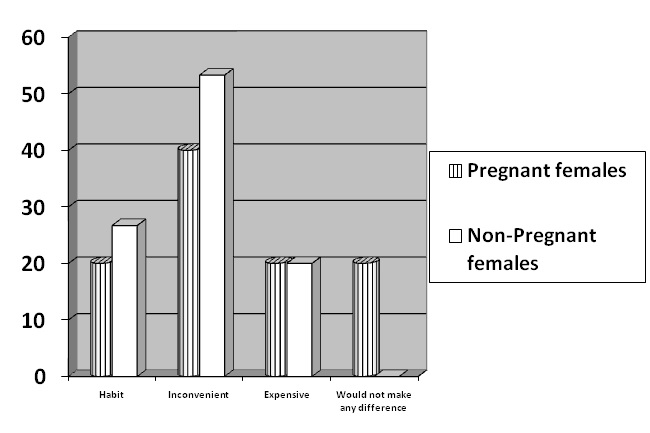
Oral hygiene habits: Majority reported quite favourable oral hygiene habits [Table/Fig-3]. The reasons for the gap between knowledge and practice of the best methods of tooth cleaning have been depicted in [Table/Fig-4].
Frequency distribution of the participants according to oral hygiene habits
| Characteristics | Pregnant (%) | Non Pregnant (%) |
|---|
| Do you clean your teeth |
| Yes | 100% | 100% |
| No | 0% | 0% |
| Means of cleaning teeth |
| Manjan | 1.5% | 1% |
| NeemDatun | 0.0% | 3.5% |
| Tooth Powder | 0.0% | 4% |
| Tooth Paste | 98.5 % | 91.4% |
| Frequency of changing toothbrush |
| Every month | 12.6% | 21.8% |
| Every 3-5 months | 26.1% | 39.9% |
| Every 6-12 months | 23.6% | 16.5% |
| When bristles lose alignment | 37.7% | 21.8% |
| Do you rinse after meals |
| Yes | 95.5% | 91.5% |
| No | 4.5% | 8.5% |
If there is a gap between practice and knowledge, the reason for not using the best method for cleaning the teeth
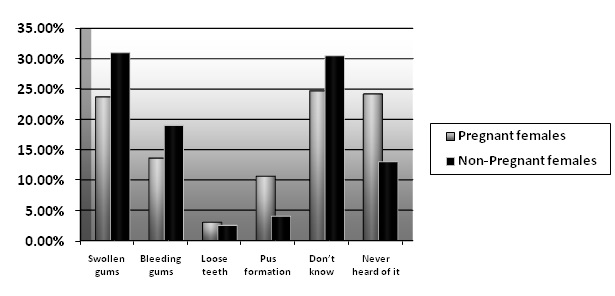
Aetiology of dental caries: Out of total, 33.5% of women in Group A and 19.0% in Group B had no knowledge about cariogenic food. [Table/Fig-5] depicts the awareness of both the groups regarding signs and symptoms of periodontal/ gum diseases.
Awareness regarding signs and symptoms of gum disease
Assessment of awareness of both the groups regarding oral and systemic inter-relationship has been tabulated in [Table/Fig-6]. Majority of women of both groups (97.5% of Group A and 94% of Group B respectively, p>0.05) were of the opinion that if they were made aware about the relationship of oral and overall health they would have been more careful in maintaining a good oral health.
Assessment of awareness of both the groups regarding oral and systemic inter-relationship (Chi-square test applied)
| Questions asked | Options given | Pregnant | Non Pregnant | p-values |
|---|
| Oral health has any role in overall health | Yes | 77.4% | 56.0% | 0.010 |
| No | 3.5% | 22.5% | 0.001** |
| Do not know | 14.6% | 15.0% | 0.896 |
| Never heard of it | 4.5% | 6.5%% | 0.394 |
| Did your physician tell you about the impact of oral health on systemic health | Yes | 4.0% | 4.0% | 0.003 |
| No | 96.0% | 96.0% | 0.959 |
| If yes, What diseases are related to oral health | Diabetes | 29.2% | 0% | 0.673 |
| Heart attack | 4.2% | 18.8% | 0.317 |
| Pregnancy outcome | 4.2% | 37.5% | .059 |
| All of the above. | 62.5% | 43.8% | 0.088 |
| How important is oral health | Very important | 71.9% | 76.5% | 0.673 |
| Not important | 1.5% | 1.5% | 0.317 |
| Doesnot matter | 0% | 1.0% | 0.059 |
| Somewhat important | 26.6% | 21.0% | 0.088 |
| Are you suffering from any systemic disease | Yes, heart disease | 0% | 5.6% | 0.655 |
| Yes, diabetes | 1.0% | 2.5% | 0.876 |
| Yes, both | 0% | 0.5% | _ |
| None | 98.5% | 88.9% | 0.349 |
| Suffering from disease and isn’t under medication | 0.5% | 2.5% | 0.102 |
| Do you go for regular medical check-up | Yes | 20.1% | 21.5% | 0.742 |
| No | 79.9% | 78.5% | 0.955 |
| Do you for regular dental check up | Yes | 6.1% | 10.5% | 0.117 |
| No | 93.9% | 89.5% | 0.714 |
| When did you last visit dentist | Last week | 0% | 2.5% | 0.564 |
| Last month | 2.5% | 11.6% | 0.001** |
| Last 3-6 months | 1.5% | 11.6% | 0.001**. |
| 6 months-1 year | 15.2% | 11.1% | 0.267 |
| More than 1 year | 22.2% | 23.1% | 0.833 |
| Never | 58.6% | 40.2% | 0.010** |
| What influences the frequency of your visit to dentist | Fear | 1% | 6.95 | 0.005** |
| Cost | 0.5% | 3.2% | 0.059 |
| Lack of time | 5.7% | 10.6% | 0.106 |
| No need | 91.7% | 79.4% | 0.150 |
| If you are told that improving health can possibly help you in improving your overall health, would you be more careful in maintaining good health | Yes | 97.5% | 94.0% | 0.798 |
| No | 0% | 0.5% | _ |
| Do not know | 2.5% | 5.5% | .134 |
p ≥ 0.05 indicates Not significant results, p < 0.05 indicates Statistically significant results, p <0.001 indicates Statistically Highly significant results as marked by (**)
Assessment of knowledge regarding correlation of oral health to adverse pregnancy outcomes in pregnant females has been tabulated in [Table/Fig-7]. Among pregnant women (Group B): 25.8% had history of abortion and 14.7% reported that their previous child was born prematurely.
Assessment of knowledge regarding correlation of oral health to adverse pregnancy outcomes in pregnant females
| Parameter | Variable | Percentage |
|---|
| History of pregnancy | First pregnancy | 38.4% |
| Twice | 11.6% |
| Thrice | 49.0% |
| More than thrice | .5% |
| Any history of abortion | Yes | 25.8% |
| No | 70.7% |
| Weight of your previous child at the time of birth | ≤1.5 kg | 5.0% |
| 1.6-2.0 kg | 11.3% |
| 2.1-2.5 kg | 27.5% |
| 2.6-3 kg | 36.3% |
| ≥3.1 kg | 20% |
| Was your child born prematurely | Yes | 14.7% |
| No | 85.3% |
| Are you diabetic | Yes before pregnancy | 3% |
| Yes after pregnancy | 5.6% |
| No | 88.9% |
| Do not know | 1.0% |
| Do you think there is a correlation between oral health and pregnancy outcome | Yes | 18.2% |
| No | 22.2% |
| Never heard of this | 58.6% |
| History of gum enlargement during pregnancy | Yes | 7.6% |
| No | 87.9% |
| Don’t know | 4.0% |
| Do your gums bleed | Yes | 23.2% |
| No | 74.2% |
| Don’t know | 2.0% |
| Have you consulted a dentist for your bleeding gums | Yes | 4.5% |
| No | 94.4% |
| Is pain in gums or bleeding from gums normal during pregnancy | Yes | 6.6% |
| No | 66.2% |
| Do not know | 26.8% |
| Do you think visiting a dentist during pregnancy is safe | Yes | 76.3% |
| No | 23.2% |
| Do you think pregnancy is a cause of loosing teeth | Yes | 17.2% |
| No | 82.3% |
| Do you believe that after delivery teeth shouldnšft be brushed | Yes | 40.9% |
| No | 52.5% |
| Don’t know | 6.1% |
| Do you think that treatment of dental related problems during pregnancy is safe | Yes | 57.1% |
| No | 41.9% |
Discussion
The majority of studied population had quite favourable tooth brushing habits (brushing at least once a day and rinsing after every meal) which are in agreement with the findings of Hullah et al., and Hashim [15,16]. One of the main finding in the present study was that the majority of pregnant women (96%) had not been educated by the gynaecologist about the impact of oral health on pregnancy outcomes. These findings coincide with that of Gunay et al., who conducted a German study and found that 71% had received no information regarding oral hygiene during pregnancy [17]. Similar results were seen in a UK study which reported that only 25% of the women had received specific advice concerning their teeth and pregnancy, mostly related to gingival and periodontal health [18].
Patil et al., in their study on 36 gynaecologists and general dental practitioners in the city of Bangalore, India, reported that 85.7% of the gynaecologists never examined the oral cavity of the patient during routine check-up. Lack of knowledge, lack of time for prenatal and health counselling, lack of demand for service and limited access to Oral health care professionals were identified as the barriers among the gynaecologists for inappropriate oral health care of the pregnant patients. A 39% of the dentists had limited knowledge on prenatal oral health care and 92% of the dentists reported need for continuing dental education programmes. They concluded that there was a need for pregnancy specific education to provide appropriate preventive and curative care to the pregnant patient [19].
In our study, pregnancy did little to change future attitudes to dental care. The difference between oral health knowledge, attitude and practices among pregnant and non pregnant female population was statistically non- significant. There was no gain in knowledge by the females after conceiving. The expecting mothers had not been educated regarding the role of periodontal diseases in adverse pregnancy outcomes or regarding the importance of regular dental check-ups. It is a cause of concern that many medical professionals are unfamiliar with the oral cavity and oral health research. We must reach out to the medical community to improve patient care through education & communication. It is our duty as periodontists to educate, motivate and reinforce our medical counterparts and the patients regarding the same.
Another crucial finding was that there was several myths related to dentistry still prevalent in India. A 52.5% opined that teeth should not be brushed after pregnancy, 23.4% were of the opinion that visiting a dentist during pregnancy was not safe and 17.2% were of the opinion that pregnancy is a cause of loosening teeth. A total of 40.9% believed that after delivery teeth should not be brushed, and another 41.9% thought dental treatment to be unsafe during pregnancy.
Majority of studied population feel that there is no need to visit a dentist. These findings are in agreement with the findings of the study among pregnant women in USA [20]. In UK, 39% did not visit a dentist during pregnancy even though dental care is free of charge for pregnant women; reasons for not seeing a dentist were the feeling that it was not necessary, fear or not liking the dentist [18].
In a study on 750 pregnant women visiting the maternity hospitals in United Arab Emirates, Hashim R reported that although a large proportion of the pregnant women in his study had oral health problems, more than 40% had not visited a dentist during their pregnancy, and the majority only utilized dental services when they had dental pain [16].
In a study on 95 pregnant women of Darussalem, Bamaniker and Kee reported that although 96.8% of the respondents agreed that women should have a dental check-up during pregnancy, only 55.9% actually practiced this. This raises serious concern since pregnant women may need extra oral and dental care due to susceptibility to gum diseases during pregnancy, which may contribute to low birth weight babies and premature births [21].
The results of our study are in accordance with those of Avula H et al., who conducted a KAP assessment of oral health and adverse pregnancy outcomes among 359 pregnant women visiting three maternity care centres in Hyderabad, India, 87.2% of their respondents were not aware of the importance of oral hygiene and its probable association with adverse pregnancy outcomes. None of the respondents ever used dental floss and only a few (1.4%) had heard about it. Avula H et al., identified poor knowledge regarding various parameters, brushing only once daily and infrequent visits to the dentist as the probable risk indicators for gingival bleeding during pregnancy in their study group [22].
Amit et al., in their study on 400 pregnant women attending the Antenatal clinic at the SMS Medical College, Jaipur, India, also reported important gaps in dental knowledge and practices related to oral health care amongst them. Only 22% of the women believed that pregnancy predisposes to dental or gum problems. Tooth ache was the driving factor for 27.7% of the women. A 54% cleaned their teeth only once daily. An 88.2% had not consulted a dentist in the previous 12 months, and only 7% had visited the dentist in their most recent pregnancy. A 40.5% were of the opinion that every painful tooth should be removed. And although most of the women displayed a reasonable level of oral health knowledge and positive attitude to oral health, it was not reflected in their oral hygiene practices [23].
Mothers play a crucial role in transferring and demonstrating health habits to their children (Rayner, Blinkhorn), so pregnant women should be a target group for oral health education especially in a country like India where population growth is very high [24,25]. Patient education is a priority. Acceptable oral hygiene techniques need to be taught, reinforced and monitored throughout pregnancy. Expecting mothers should be made aware that periodontal treatment during pregnancy is safe for both mother and child.
In order to promote health, it is necessary for the would-be -mothers to be aware of disease symptoms and to be encouraged to adopt appropriate health behaviour. Pregnant women are more likely to seek dental care if their gynecologist/antenatal care giver recommends. They are better than the dentists to counsel and convince the patients regarding oral health care during the prenatal and postnatal period. This should involve all health agencies, Midwives and gynecologists involved in antenatal care to influence, educate and promote well-being in mothers. We would also like to recommend that periodic dental checkups be incorporated in the antenatal health cards, and routine dental checkups be clubbed with their visits to the Gynecologist in each trimester. This is a doable exercise, which would ensure that even the most ignorant of the expecting mothers, would be visiting the dentist for a checkup, thereby giving the dentist the opportunity to further stress upon the importance of good oral hygiene on a one-to-one basis.
Limitations
This being a questionnaire study has certain limitations of its own. It had a relatively small sample size, hence the results should be interpreted with caution. The relationship between the level of oral health knowledge and various maternal factors such as spacing between children, care during pregnancy, and maternal nutritional status was not evaluated.
Conclusion
There was no gain in knowledge by the females after conceiving. An oral health history, oral health education, dental screening, and dental referral, if needed, should be a routine part of prenatal care and annual examinations.
p ≥ 0.05 indicates Not significant results, p < 0.05 indicates Statistically significant results, p <0.001 indicates Statistically Highly significant results
p ≥ 0.05 indicates Not significant results, p < 0.05 indicates Statistically significant results, p <0.001 indicates Statistically Highly significant results as marked by (**)
[1]. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maynor G, Periodontal infection as a possible risk factor for preterm low birth weightJ Periodontol 1996 67:1103-13. [Google Scholar]
[2]. Contreas A, Herrera JA, Soti JE, Arce RM, Jaramillo A, Botero JE, Periodontitis is associated with preclampsia in pregnant womenJ Periodontol 2006 77:182-88. [Google Scholar]
[3]. Scannapieco F, Bush RB, Paju S, Periodontal disease is a risk factor for adverse pregnancy outcomes. A systematic reviewAnn Periodontol 2003 8:70-78. [Google Scholar]
[4]. Mokkem SA, Molla GN, Al-Jewair TS, The prevalence and relationship between periodontal disease and pre- term low birth weight infants at King Khalid University Hospital in Riyadh, Saudi ArabiaJ Contemp Dent Pract 2004 5:40-45. [Google Scholar]
[5]. Offenbacher S, Jared HL, O’Reilly PG, Wells SR, Salvi GE, Lawrence HP, Potential pathogenic mechanisms of periodontitis associated pregnancy complicationsAnn Periodontol 1998 3:233-50. [Google Scholar]
[6]. Katz J, Chegini N, Shiverick KT, Lamont RJ, Localization of P gingivalis in preterm delivery placentaJ Dent Res 2009 88:575-78. [Google Scholar]
[7]. Fardini Y, Chung P, Dumm R, Joshi N, Han YW, Transmission of diverse oral bacteria to murine placenta: evidence for the oral microbioma as a potential source of intrauterine infectionInfect Immun 2010 78:1789-96. [Google Scholar]
[8]. Dasanayake AP, Boyd D, Madianos PN, Offenbacher S, Hills E, The association between Porphyromonas gingivalis-specific maternal serum IgG and low birth weightJ Periodontol 2001 72:1491-97. [Google Scholar]
[9]. Dasanayake AP, Russell S, Boyd D, Madianos PN, Forster T, Hill E, Preterm low birth weight and periodontal disease among African AmericansDent Clin North Am 2003 47:115-25. [Google Scholar]
[10]. National Neonatology Forum NNPD Network National neonatal-perinatal database: report for 2002-2003. New Delhi: National Neonatology Forum NNPD Network; 2005 [Google Scholar]
[11]. Mannem S, Chava VK, The relationship between maternal periodontitis and preterm low birth weight: A case-control studyContemp Clin Dent 2011 2:88-93. [Google Scholar]
[12]. Offenbacher S, Periodontal Dieseases: PathogenesisAnn Periodontol 1996 1:821 [Google Scholar]
[13]. Tarannum F, Faizuddin M, Effect of periodontal therapy on pregnancy outcome in women affected by periodontitisJ Periodontol 2007 78:2095-103. [Google Scholar]
[14]. Radnai M, Pál A, Novák T, Urbán E, Eller J, Gorzó I, Benefits of periodontal therapy when preterm birth threatensJ Dent Res 2009 88:280-84. [Google Scholar]
[15]. Hullah E, Turok Y, Nauta M, Self reported oral hygiene habits, dental attendance and attitudes to dentistry during pregnancy in a sample of immigrant women in North LondonArch Gynecol Obstet 2008 277:405-09. [Google Scholar]
[16]. Hashim R, Self reported oral health, oral hygiene habits and dental service utilization among pregnant women in United Arab EmiratesInt J Dent Hygiene 2012 10:142-46. [Google Scholar]
[17]. Gunay H, Goepel K, Stock KH, Schneller T, Position of health education knowledge concerninig pregnancyOralprophylaxe 1991 13:4-7. [Google Scholar]
[18]. Rogers SN, Dental attendances in a sample of pregnant women in Birmingham, UKCommunity Dent Health 1991 8:361-69. [Google Scholar]
[19]. Patil S, Thakur R, Madhu K, Paul ST, Gdicherla P, Oral Health Coalition: Knowledge, attitude and Practice behaviours among Gynaecologists and dental practitionersJ Int Oral Health 2013 5:8-15. [Google Scholar]
[20]. Mangskau KA, Arrindell B, Pregnancy and oral health utilization of the oral health care system by pregnant women in North DakotaNorthwest Dent 1996 75:823-28. [Google Scholar]
[21]. Bamanikar S, Kee LK, Knowledge, attitude and Practice of oral and dental health care in pregnant womenOman Med J 2013 28:288-91. [Google Scholar]
[22]. Avula H, Mishra A, Arora N, Avula J, KAP assessment of oral health and adverse pregnancy outcomes among pregnant women in Hyderabad, IndiaOral Health Prev Dent 2013 11:261-70. [Google Scholar]
[23]. Amit Mital P, Hooja N, Mital P, Salvi A, Fatima A, Oral and dental health knowledge, attitude and practice among pregnant womenSch Acad J Biosci 2014 2(9):627-32. [Google Scholar]
[24]. Rayner JF, Socio-economic status and factors influencing the dental health practices of mothersAm J Public Health Nations Health 1970 60:1250-58. [Google Scholar]
[25]. Blinkhorn AS, Dental preventive advice for pregnant and nursing mothers – sociological implicationsInternational Dental journal 1981 31:14-22. [Google Scholar]