An Open Label Parallel Group Study to Assess the Effects of Amlodipine and Cilnidipine on Pulse Wave Velocity and Augmentation Pressures in Mild to Moderate Essential Hypertensive Patients
Rama Mohan Pathapati1, Sujith Tumkur Rajashekar2, Madhavulu Buchineni3, Rajesh Kumar Meriga4, Chirra Bhakthavasthala Reddy5, Kolla Praveen Kumar6
1 Associate Professor, Department of Pharmacology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
2 Post Graduate Student, Department of Pharmacology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
3 Associate Professor, Department of Pharmacology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
4 Professor, Department of General Medicine, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
5 Associate Professor, Department of Cardiology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
6 Professor, Department of Nephrology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rama Mohan Pathapathi, Associate Professor, Department of Pharmacology, Narayana Medical College and Hospital, Nellore, Andhra Pradesh-524003, India.
E-mail: pill4ill@yahoo.co.in
Introduction
Hypertension is a major cardiovascular risk factor, which affects both large and small arteries. Because of the associated morbidity and mortality and the cost to society, it is an important public health challenge. Population based studies have reported that large artery stiffness is an important determinant of cardiovascular events and mortality in general population and in patients with hypertension. This study was designed to compare the effects of 8 weeks blood pressure control using Amlodepine and cilnidipine on haemodynamic parameters and vascular indices in mild to moderate hypertensive patients.
Materials and Methods
A total of 60 patients were enrolled in the study. Thirty patients were randomly allocated to either Amlodipine 5 mg OD or Cilnidipine 10 mg OD for duration of eight weeks. Blood Pressure (BP), Heart Rate (HR), carotid-femoral Pulse Wave Velocity (cf PWV), Augmentation Index (AIx) and Aortic augmentation pressure (AoAP) were measured at baseline and at the end of eight weeks.
Results
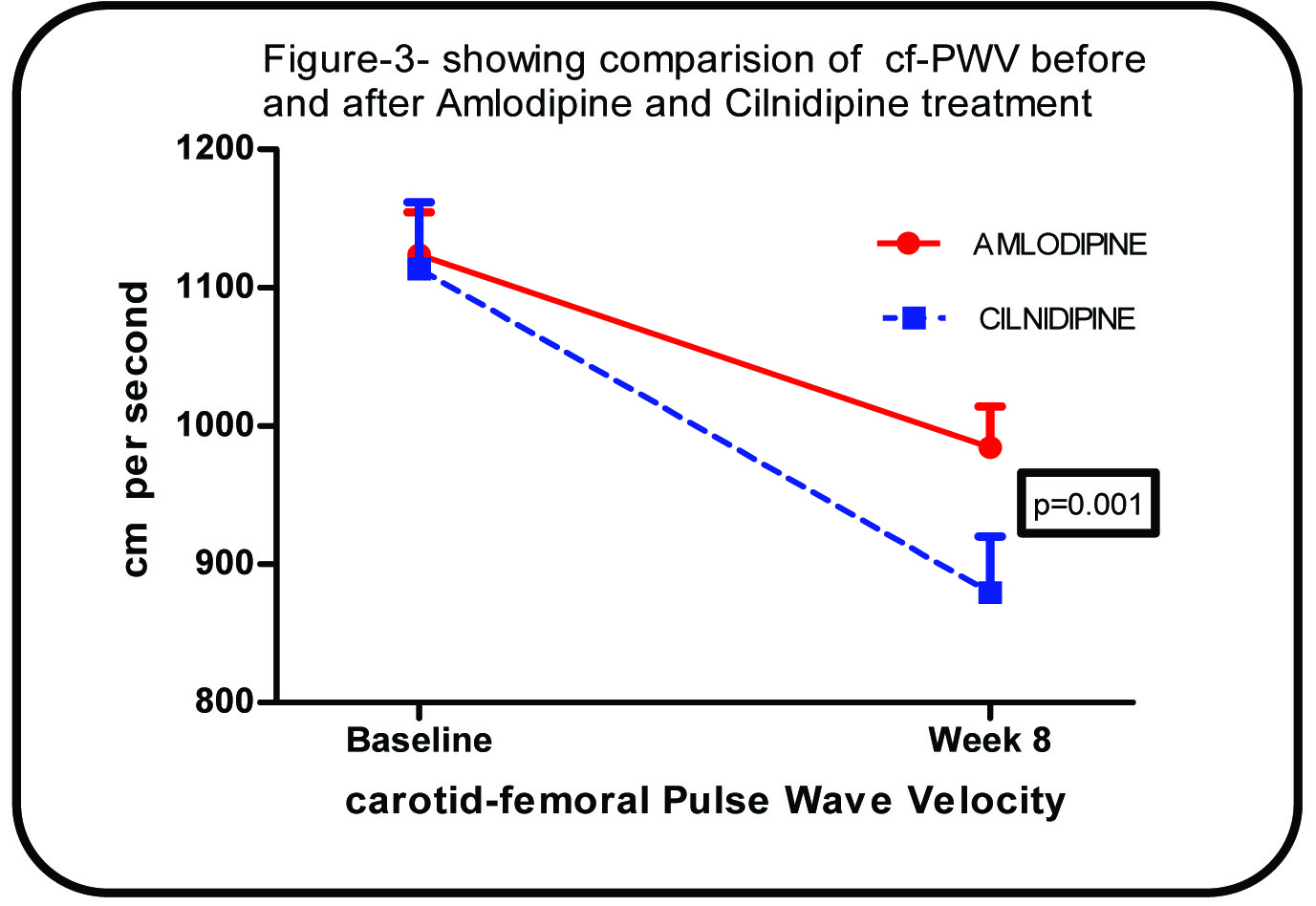
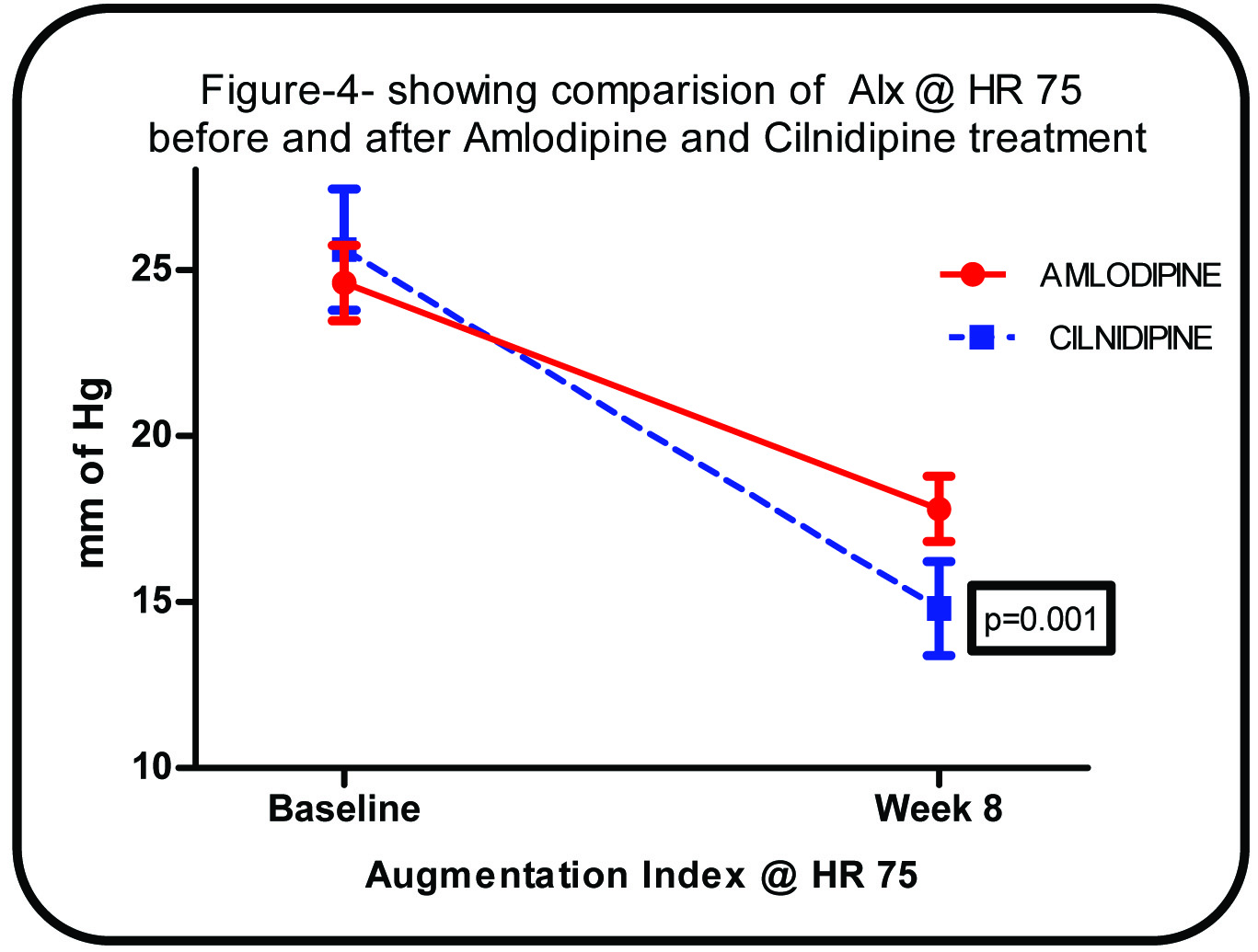
The mean change in the central artery stiffness from baseline to week-8 in the Amlodipine group as compared to Cilnidipine group cf PWV -139.3±27.7 vs. -234.1±74.8 cm/s p=<0.0001, AoAP -3.8±1.5 vs. -5.6±3.3 mm of Hg p=0.008 and AIx -6.8±2.4 vs. -10.8±4.4 %, p=<0.0001 respectively.
Conclusion
This study showed that the L/N-type calcium channel antagonist Cilnidipine has a similar antihypertensive action to Amlodipine, but is superior in improving the arterial stiffness.
Arterial stiffness, Augmentation Index, Carotid-femoral pulse wave velocity
Introduction
Hypertension is one of the most common disease afflicting humans throughout the world. Because of the associated morbidity and mortality and the cost to society, it is an important public health challenge as well [1].
The associated cardiovascular risk factors with hypertension syndrome [2] are obesity, accelerated atherogenicity, left ventricular hypertrophy and dysfunction, changes in blood clotting mechanisms, changes in renal function, abnormalities in neurohormonal functions, abnormal insulin and glucose metabolism, endothelial dysfunction and decreased arterial compliance (increased arterial stiffness).
Increase in arterial stiffness may results in higher systolic blood pressure (SBP); lower diastolic blood pressure (DBP) and wide pulse pressure (PP) all conferring greater cardiovascular and total mortality risk. Increased arterial stiffness through an elevation of SBP enhances the left ventricular load and favours cardiac hypertrophy and, through reduction of DBP, results in a decrease in the perfusion pressure of the coronary arteries, thus contributing to myocardial ischemia. The degree of arterial stiffness, obtained in various populations, has been found to be a powerful independent marker of vascular target organ damage and an independent prognostic predictor for cardiovascular morbidity, as well as cardiovascular and all cause mortality [2–7]. Measuring pulse wave velocity (PWV) to assess arterial stiffness is a simple and reproducible method. The underlying principles and technique of this method have been described in detail previously. Several experimental studies have shown that PWV is related to the arterial wall structure, function, geometry and endothelium functions [8]. Amlodipine and Cilnidipine both were calcium channel blockers with greater effect in reducing blood pressure (BP) and decrease intraglomerular pressure by dilating the efferent arterioles [9,10].
This study was designed to compare the effects of 8 weeks blood pressure (BP) control using Amlodepine and cilnidipine on haemodynamic parameters and vascular indices in mild to moderate hypertensive patients.
The aortic PWV is the “gold standard” marker for measuring arterial stiffness, and is widely used to estimate vascular stiffness and “vascular health” [11]. Dihydropyridine (DHP) calcium channel blockers (CCBs) like Amlodipine are frequently used in the treatment of hypertension, stable angina pectoris and cerebrovascular disease by blocking L-type voltage-gated Ca2+ channels. Cilnidipine is a unique Ca2+ channel blocker used for hypertensive patients, which inhibits sympathetic N-type Ca2+ channels in addition to vascular L-type Ca2+ channels [12].
Materials and Methods
The Institutional Ethical Committee approved this open label randomized parallel group study protocol conducted during period 2012-2013. Informed consent was obtained from study participants. All the participants who were receiving Amlodepine in the age group between 20 to 60 years with sitting systolic blood pressure between 140-160 mm Hg and diastolic blood pressure between 90-100 Hg. Patients were excluded, if the hypertension was secondary to hepatic, renal, cardiac or endocrine disorders, pregnant or lactating. In the present study, 84 patients were screened and after meeting the inclusion and exclusion criteria, a total of 60 patients were enrolled in the study. Thirty patients received either Amlodipine 5 mg OD or Cilnidipine 10 mg OD for duration of eight weeks. Blood Pressure (BP), Heart Rate (HR), carotid-femoral Pulse Wave Velocity (cf PWV), Augmentation Index (AIx) and Aortic augmentation pressure (AoAP) were measured at baseline and at the end of eight weeks. Demographic, clinical and laboratory records of the enrolled patients were also recorded. After the completion of the study, the patients were instructed to consult their physician for further management; however, none of the patients were deprived of antihypertensive medication.
Pulse Wave Velocity
The Carotid Femoral (CF) PWV was measured using a Volume-plethysmographic apparatus. (Periscope, M/s Genesis Medical Systems, Hyderabad India). This instrument also records blood pressure and electrocardiogram. The subjects were examined in the spine position after a 10 minutes rest, with electrodes connected to all the four limbs and cuffs wrapped on both the brachia and ankles. The plethysmographic sensor and the oscillometric pressure sensors positioned in these cuffs records volume waveforms and blood pressure respectively. Initially the brachial ankle pulse wave velocities (baPWV) of the right and left were obtained from the stored wave forms. Subsequently, cf PWV was calculated automatically from the mathematical equation. cf PWV= 0.833* average baPWV-233.3 [13–15]. Augmentation index (AIx) was calculated as the increment in pressure from the first shoulder in the ascending aortic pressure wave to the peak of this wave, expressed as a percentage of the peak ascending aortic pressure wave. AIx=100*ΔP/PP. where ΔP is Augmentation pressure [16].
Statistical Analysis
The statistical analysis was carried using Graph pad prism software (Version-5, USA) continuous data was presented as Mean±SD and Categorical as actual numbers and percentages. For normally distributed data, with-in group analysis was performed by using paired t-test and between group analyses by unpaired t-test. Non-normally distributed data was analysed by using non-parametric “Mann-Whitney U test”. Categorical variables were analysed with “Fischer’s exact test”. All the efficacy parameters were presented as absolute change from baseline. A negative sign indicates decrease and vice versa. For statistical significance, a two tailed probability value of less than 0.05 was considered. A sample of 25 patients per group was required to demonstrate an estimated change in primary efficacy variable cf PWV of 1 m/s from baseline in both groups, with 80% power to detect the difference and two sided alpha error of 0.05 [17]. Additionally 5 patients were added to pay off for drop outs.
Results
In the present comparative study, there were 21 males and 9 females in the Amlodipine group and 24 males and 6 females in the Cilnidipine group. There was no statistically significant difference in demographic, anthropometric and clinical characteristics of Amlodipine and Cilnidipine groups. Additionally, baseline haemodynamic and vascular indices parameters were also similar between the two groups as shown in [Table/Fig-1]. After eight weeks of treatment with Amlodipine and Cilnidipine, it was found that [Table/Fig-2] there was a significant change in the haemodynamic and vascular indices from baseline in each group. [Table/Fig-3,4,5 and 6]. When we evaluated the absolute change from baseline to eight weeks in the peripheral haemodynamic parameters between Amlodipine and Cilnidipine groups [Table/Fig-7], it became apparent that there was no statistically significant difference between the two groups. However, we found a statistically significant change in the central haemodynamic and vascular indices in the Cilnidipine group as compared to Amlodipine. All the subjects who participated in the study showed good compliance and none of them developed side effects.
Baseline demographic, haemodynamic and vascular indices of mild-moderate essential hypertensive patients according to treatment group.
| Parameters | Amlodipine | Cilnidipine | p-value |
|---|
| N=30 | N=30 |
|---|
| Demographic | Mean ±SD | Mean ±SD |
|---|
| Age (years) | 50.7±6.8 | 49.9±8.9 | 0.72 |
| Gender (M/F) | 21/9 | 24/6 | 0.55 |
| Weight (kg) | 67.03±14.2 | 65.27±13.7 | 0.62 |
| Height(cm) | 162.4±10.1 | 158.77±11.1 | 0.19 |
| BMI(kg/m2) | 25.3±4.2 | 25.9±4.7 | 0.63 |
| Diabetes | 12(40%) | 10(33.3%) | 0.79 |
| Smoking | 8(26.7%) | 7(23.3%) | 1.00 |
| Alcohol | 5(16.6%) | 4(13.3%) | 1.00 |
| Statins | 13(43.3%) | 9(30%) | 0.42 |
| Antiplatelets | 6(20%) | 8(26.7%) | 0.76 |
| Peripheral Haemodynamic |
| SBP(mm Hg) | 152.4±6.7 | 149.2±7.0 | 0.07 |
| DBP(mm Hg) | 81.6±8.8 | 81.5±10.6 | 0.99 |
| PP(mm Hg) | 70.8± 8.8 | 67.6 ±11.7 | 0.23 |
| HR(bpm) | 82.3±15.5 | 81.9±11.0 | 0.89 |
| Central Haemodynamic |
| Aortic SBP(mm Hg) | 123.8±14.6 | 125.8±14.7 | 0.60 |
| Aortic DBP(mm Hg) | 78.1±10.6 | 81.7±10.5 | 0.20 |
| Aortic PP(mm Hg) | 45.6 ±12.3 | 44.1± 10.9 | 0.60 |
| Vascular Indices |
| AoAP (mm Hg) | 11.5±5.4 | 12.1±6.4 | 0.72 |
| AoAIx | 24.6±6.2 | 25.6±10.0 | 0.65 |
| Cf PWV(cm/sec) | 1123.9±167 | 1113.6±263 | 0.86 |
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
Comparison of haemodynamic and vascular indices before and after Amlodipine and Cilnidipine treatment
| Parameters | AMLODIPINE N=30 | p-value | CILNIDIPINE N=30 | p-value |
|---|
| Peripheral Haemodynamic | Baseline | Week 8 | Baseline | Week 8 |
|---|
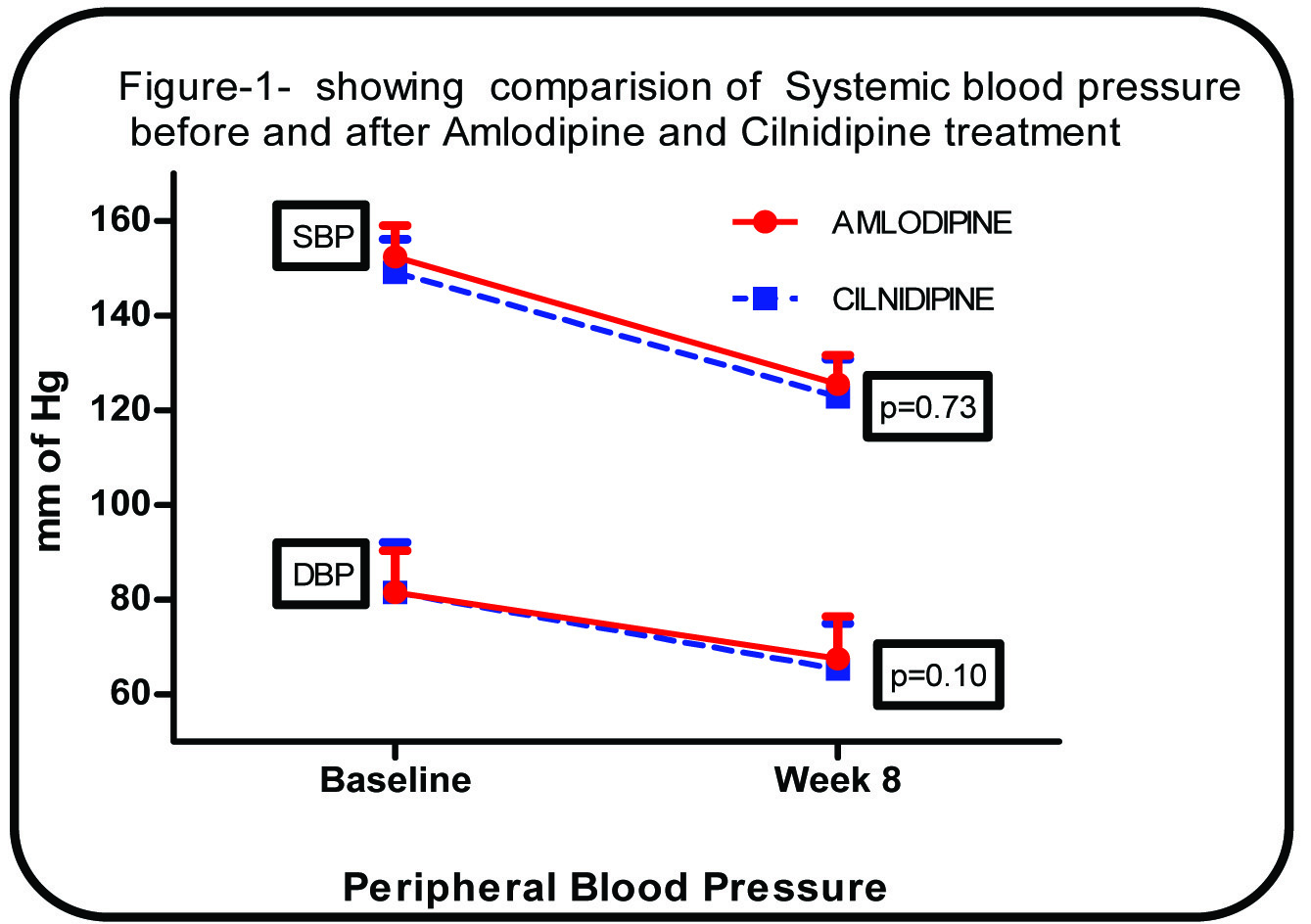
| SBP(mm Hg) | 152.4±6.7 | 125.5±6.1 | <0.0001 | 149.2±7.0 | 122.8±8.0 | <0.0001 |
| DBP(mm Hg) | 81.6±8.8 | 67.6±8.8 | <0.0001 | 81.5±10.6 | 65.3±9.7 | <0.0001 |
| PP(mm Hg) | 70.8± 8.8 | 57.9± 8.1 | <0.0001 | 67.6 ±11.7 | 57.5 ±9.3 | <0.0001 |
| HR(bpm) | 82.3±15.5 | 84.2±11.9 | 0.24 | 81.9±11.0 | 80.6±10.2 | 0.23 |
| Central Haemodynamic |
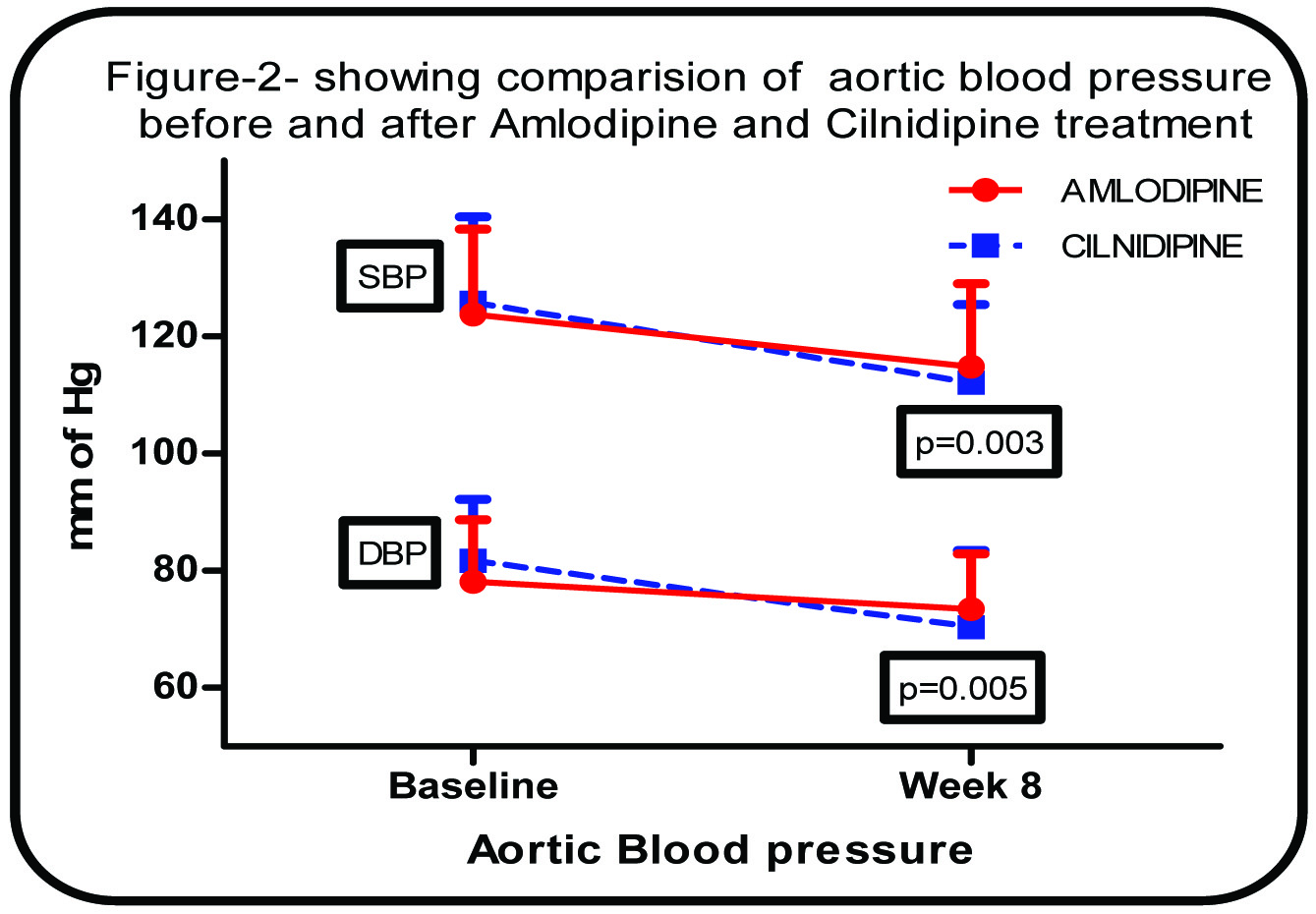
| Aortic SBP(mm Hg) | 123.8±14.6 | 114.8±14 | <0.0001 | 125.8±14 | 112.1±13 | <0.0001 |
| Aortic DBP(mm Hg) | 78.1±10.6 | 73.5±9.4 | 0.02 | 81.7±10.5 | 70.3±13.1 | <0.0001 |
| Aortic PP(mm Hg) | 45.6 ±12.3 | 41.4 ±14.9 | 0.02 | 44.1± 10.9 | 41.8 ±10.9 | 0.22 |
| Vascular Indices |
| AoAP (mm Hg) | 11.5±5.4 | 7.7±4.8 | <0.0001 | 12.1±6.4 | 6.5±4.1 | <0.0001 |
| AoAIx | 24.6±6.2 | 17.8±5.4 | <0.0001 | 25.6±10.0 | 14.9±7.8 | <0.0001 |
| Cf PWV(cm/sec) | 1124±167 | 984±162 | <0.0001 | 1113±263 | 879±223 | <0.0001 |
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
Showing comparison of Systemic blood pressure before and after Amlodipine and Cilnidipine treatment
Showing comparison of aortic blood pressure before and after Amlodipine and Cilnidipine treatment
Showing comparison of cf-PWV before and after Amlodipine and Cilnidipine treatment
Showing comparison of AIx @ HR 75 before and after Amlodipine and Cilnidipine treatment
Comparison Of mean change from baseline in the haemodynamic & vascular indices between Amlodipine and Cilnidipine Groups.
| Mean Change in Parameters | Amlodipine | Cilnidipine | p-value |
|---|
| Peripheral Haemodynamic | Baseline | Week 8 |
|---|
| ΔSBP(mm Hg) | -26.9±4.9 | -26.3±7.6 | 0.73 |
| ΔDBP(mm Hg) | -14.0±3.6 | -16.2±6.3 | 0.10 |
| ΔPP(mm Hg) | -4.6± 5.4 | -5± 8.2 | 0.82 |
| ΔHR(bpm) | 1.8±8.4 | -1.3±5.8 | 0.10 |
| Central Haemodynamic |
| ΔAortic SBP(mm Hg) | -8.9±2.3 | -13.7±8.1 | 0.003 |
| ΔAortic DBP(mm Hg) | -4.6±10.3 | -11.4±7.2 | 0.005 |
| Aortic PP(mm Hg) | -4.29± 9.6 | -2.26± 9.8 | 0.42 |
| Vascular Indices | | | |
| ΔAoAP(mm Hg) | -3.8±1.5 | -5.6±3.3 | 0.008 |
| ΔAoAIx | -6.8±2.4 | -10.8±4.4 | 0.001 |
| Δcf-PWV(cm/sec) | -139.3±27.7 | -234.1±74.8 | 0.001 |
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
Discussion
Hypertension is a major cardiovascular risk factor, which affects both large and small arteries. Population based studies have reported that large artery stiffness is an important determinant of cardiovascular events and mortality in general population and in patients with hypertension [9]. Calcium channel blockers (CCB) are frequently used drugs to treat hypertensive patients in our hospital setup. The mechanism of action in hypertension is due to its inhibition of calcium influx into vascular smooth muscle cells (VMC) that causes relaxation of VMC, decreased after load and systemic blood pressure. It is also evident from the reports that dihydropyridine calcium antagonists improve arterial wall stiffness [18,19].
We studied the haemodynamic and vascular effects of Amlodipine and Cilnidipine and found that there was a statistically significant decrease in peripheral blood pressure when compared to baseline in both the groups after eight weeks but not in Heart rate. Satoshi Morimoto et al., also reported that Amlodipine at 5 mg daily dosage and Cilnidipine at a daily dose of 10 mg per day are equally effective in reducing the blood pressure in patients with mild to moderate hypertension [20]. Additionally, they also improved central blood pressure as well as indices of arterial stiffness (cf PWV & AIx). On comparison between the medications; the decrease in peripheral blood pressure between two groups was not statistically significant. For a similar reduction in peripheral blood pressures, we observed that Cilnidipine showed significantly higher improvement in aortic blood pressure and AoAP as well as markers of arterial stiffness (cf-PWV & AIx) than with Amlodipine.
The proposed mechanisms for such an improvement in cf PWV and AIx by CCBs are acute changes in the functional properties such as vascular smooth muscle relaxation, reduction in wave reflections, improvement in endothelial dysfunction or regulation of sympathetic nervous system. It is unlikely that the structural changes would occur after 8 weeks of therapy, the likely mechanism for the improvement in arterial compliance in present study may be due to improved vascular smooth muscle relaxation possibly by increased bioavailability of NO.
Studies have reported that CCBs also have an anti-inflammatory and anti-oxidative effect independent of their effect on lowering BP [21]. Amlodipine has been reported to increase endothelial nitric oxide synthase (eNOS) activity [22] and to improve endothelial functions [23] in experimental models. Hok Sum Leung et al., showed that Cilnidipine also increases release or bioavailability of NO, due to elevated endothelial Ca2+ ions in arteries [24]. Chandra et al., in his study confirmed Cilnidipine significantly induced eNOS activity, as well as increased eNOS concentration in rats when compared with Amlodipine. Also, Cilnidipine is both an L/N-type CCB, has an inhibitory effect on cardiovascular sympathetic neurotransmission in contrast to L type CCB like Amlodipine [25]. One or all of such mechanisms could be the possible explanations for such an improvement over Amlodipine. This makes it useful in the treatment of cardiovascular diseases associated with diminished NO release, such as atherosclerosis. Moreover, this mechanism is independent of its effect on L/N-type receptors [26].
Study Limitations
In the present study, we have used non-invasive method, which simultaneously records blood pressure, pressure waves and also calculates the parameters of velocity at different points from these recordings. Although the present equipment data is well validated, however, the accuracy cannot be comparable to the invasive haemodynamic monitoring. Due to ethical reasons, invasive monitoring was not attempted. Cilnidipine showed a better improvement in arterial stiffness than Amlodipine without much difference in blood pressure reduction. However, such an interpretation needs carefulness because the time at which they took the medication before each study day, concomitant medications, co-morbid conditions and wider confidence intervals in electrophysiological parameters could have been confounding factors. Larger-scale studies are required to confirm above stated results.
Conclusion
This study showed that the L/N-type calcium channel antagonist cilnidipine has a similar antihypertensive action to the L-type calcium channel antagonist amlodipine, but is superior in terms of improving arterial stiffness and central aortic pressures. Cilnidipine can be recommended as the treatment of choice for patients with essential hypertension. However Larger-scale studies are required to confirm above stated results.
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
SBP-Systolic Blood Pressure, MBP-Mean Blood Pressure, DBP-Diastolic Blood Pressure, PP—Pulse Pressure, HR-Heart Rate, AoAP-Aortic Augmentation pressure, AoAIx- Aortic Augmentation Index, cf PWV- Carotid femoral Pulse Wave Velocity
[1]. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 reportJAMA 2003 289(19):2560-72. [Google Scholar]
[2]. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM, Impact of aortic stiffness on survival in end-stage renal diseaseCirculation 1999 99(18):2434-39. [Google Scholar]
[3]. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patientsHypertension 2001 37(5):1236-41. [Google Scholar]
[4]. Laurent S, Katsahian S, Fassot C, Tropeano AI, Gautier I, Laloux B, Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. StrokeA journal of cerebral circulation 2003 34(5):1203-06. [Google Scholar]
[5]. Meaume S, Benetos A, Henry OF, Rudnichi A, Safar ME, Aortic pulse wave velocity predicts cardiovascular mortality in subjects >70 years of ageArteriosclerosis, thrombosis, and vascular biology 2001 21(12):2046-50. [Google Scholar]
[6]. Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley P, Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients: a longitudinal studyHypertension 2002 39(1):10-15. [Google Scholar]
[7]. Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general populationCirculation 2006 113(5):664-70. [Google Scholar]
[8]. Asmar R, Arterial stiffness and pulse wave velocity – Clinical applications 1999 ParisElsevier:9-43. [Google Scholar]
[9]. Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trialLancet (London, England) 2004 363(9426):2022-31.PubMed PMID: 15207952. Epub 2004/06/23. eng [Google Scholar]
[10]. Hayashi K, Wakino S, Sugano N, Ozawa Y, Homma K, Saruta T, Ca2+ channel subtypes and pharmacology in the kidneyCirculation research 2007 100(3):342-53.PubMed PMID: 17307972. Epub 2007/02/20. eng [Google Scholar]
[11]. Jochen S VB, Dan EB, Daniel N, Vascular Stiffness and Increased Pulse Pressure in the Aging Cardiovascular SystemCardiology Research and Practice 2011 1:1-6. [Google Scholar]
[12]. Takahara A, Cilnidipine: a new generation Ca channel blocker with inhibitory action on sympathetic neurotransmitter releaseCardiovascular therapeutics 2009 27(2):124-39.PubMed PMID: 19426250. Epub 2009/05/12. eng [Google Scholar]
[13]. Raju DS, Mohan PR, Naidu M, Effect of allopurinol on arterial stiffness and endothelial function in patients with chronic renal failureIndian Journal of Nephrology 2007 17(3) [Google Scholar]
[14]. Pathapati RM, Reddy CB, Buchineni M, Sujith TR, Kumar MR, Praveen K, An open-label study to assess the effect of a single dose of Nebivolol and Ivabradine on heart rate and pulse wave velocity in hypertensive patients receiving amlodipineInt J Basic Clin Pharmacol 2015 4(2):219-23. [Google Scholar]
[15]. Naidu MU, Reddy BM, Yashmaina S, Patnaik AN, Rani PU, Validity and reproducibility of arterial pulse wave velocity measurement using new device with oscillometric technique: a pilot studyBiomedical engineering online 2005 4:49 [Google Scholar]
[16]. Naidu MUR, Reddy CP, Non-invasive measurement of aortic pressure in patients: Comparing pulse wave analysis and applanation tonometryIndian Journal of Pharmacology 2012 44(2):230-33. [Google Scholar]
[17]. Pathapati RM, Rajesh Kumar M, Chirra BR, Buchineni M, Sujith TR, Devaraju SR, Acute Effects of Two Angiotensin Receptor Blockers on Vascular Haemodynamics, Arterial Stiffness, and Oxidative Stress in Patients with Mild to Moderate Hypertension: An Open Label Parallel Group StudyISRN Vascular Medicine 2013 2013:5 [Google Scholar]
[18]. Safar ME, Pannier B, Laurent S, London GM, Calcium-entry blockers and arterial compliance in hypertensionJournal of cardiovascular pharmacology 1989 14(Suppl 10):S1-6.discussion S59-62 [Google Scholar]
[19]. Kim KH, Jeong MH, Cho SH, Moon JY, Hong YJ, Park HW, Clinical effects of calcium channel blocker and Angiotensin converting enzyme inhibitor on endothelial function and arterial stiffness in patients with angina pectorisJournal of Korean medical science 2009 24(2):223-31. [Google Scholar]
[20]. Morimoto S, Yano Y, Maki K, Iwasaka T, Renal and vascular protective effects of cilnidipine in patients with essential hypertensionJournal of hypertension 2007 25(10):2178-83. [Google Scholar]
[21]. Yoshii T, Iwai M, Li Z, Chen R, Ide A, Fukunaga S, Regression of atherosclerosis by amlodipine via anti-inflammatory and anti-oxidative stress actionsHypertension research: official journal of the Japanese Society of Hypertension 2006 29(6):457-66. [Google Scholar]
[22]. Berkels R, Taubert D, Bartels H, Breitenbach T, Klaus W, Roesen R, Amlodipine increases endothelial nitric oxide by dual mechanismsPharmacology 2004 70(1):39-45. [Google Scholar]
[23]. InvestigatorsE. Effect of nifedipine and cerivastatin on coronary endothelial function in patients with coronary artery disease: the ENCORE I Study (Evaluation of Nifedipine and Cerivastatin On Recovery of coronary Endothelial function)Circulation 2003 107(3):422-28. [Google Scholar]
[24]. Leung HS, Yao X, Leung FP, Ko WH, Chen ZY, Gollasch M, Cilnidipine, a slow-acting Ca2+ channel blocker, induces relaxation in porcine coronary artery: role of endothelial nitric oxide and [Ca2+]iBritish journal of pharmacology 2006 147(1):55-63. [Google Scholar]
[25]. Chandra KS, Ramesh G, The fourth-generation Calcium channel blocker: cilnidipineIndian heart journal 2013 65(6):691-95. [Google Scholar]
[26]. Adams DJ, Barakeh J, Laskey R, Van Breemen C, Ion channels and regulation of intracellular calcium in vascular endothelial cellsFASEB journal: official publication of the Federation of American Societies for Experimental Biology 1989 3(12):2389-400. [Google Scholar]