Chromium, an essential trace element as well as a vital antioxidant, plays an important role in glucose and lipid metabolism by improving glucose intolerance and lowering elevated lipids. Chromium deficiency affects the maintenance of normal glucose tolerance and healthy lipid profiles [1]. Chromium deficient type 2 diabetic were noted to have decreased insulin binding & reduced number of insulin receptors, thereby leading to glucose intolerance [2]. Low molecular weight chromium binding substance (LMWCr), otherwise called as chromomodulin, has been postulated to be a part of an insulin signal amplification mechanism [3]. LMWCr is an oligopeptide which is composed of cysteine, glutamate, aspartate and glycine [4]. The binding of chromium ions to the apo-form of LMWCr results in the stabilisation of the active conformation of insulin receptor tyrosine kinase, thereby facilitating the action of insulin [5]. LMWCr also causes inhibition of phosphotyrosine phosphatase, an inactivator of enzyme tyrosine kinase [6]. Chromium deficiency also manifests separately as neuropathy, encephalopathy and impaired immune response. As age advances, the levels of chromium in hair, sweat and blood decreases significantly [7].
The most often used approach to assess the total body chromium status is the measurement of serum chromium levels. Rajpathak et al., reported lower serum chromium levels in type 2 diabetic when compared with nondiabetic healthy control subjects [8]. In addition to chromium, levels of zinc and manganese were also found to be decreased in diabetics when compared with the normal population [9]. A recent study from South India also showed a decrease in chromium levels in gestational diabetics [10]. The relationship of chromium levels to glycaemic control in type 2 diabetic have not been studied in detail. In this background, the study was designed to assess the level of serum chromium in newly diagnosed type 2 diabetic and its association with their glycaemic control.
Materials and Methods
Study Design and Patient Selection
This was a hospital based cross-sectional comparative study to determine the serum chromium levels among newly diagnosed type 2 diabetes mellitus patients who satisfy the American Diabetes Association criteria. Newly diagnosed type 2 diabetic patients without any pre-existing complications between the age of 30 and 60 years were screened from the diabetic outpatient clinic of a tertiary care hospital in a semiurban area of Tamilnadu.
Patients with renal failure, hepatic failure, cardiac failure, thyroid disorders, alcoholics, lactating and pregnant females and those who were under treatment with chromium supplements, cisplatin, amiloride, quinolones, ACE inhibitors, tetracyclines and thiazide diuretics were excluded to avoid potential confounding factors.
From the review of literature, it was established that in order to have a significant difference between the two groups, it was necessary to identify a difference of atleast 0.5ng/ml between the two groups at a significance level of 95%, with the power of atleast 80%, so a minimum of 19 patients had to be enrolled in each group. Hence the study proceeded with the enrollment of eligible patients after obtaining due permission from the Institutional scientific Review Board and Institutional Ethics Committee.
One hundred and seventy patients were identified in the study period who were willing to undergo the study after giving written informed consent. The patients were divided into two groups depending on whether their HbA1c value was more than 7.0% or less than or equal to 7.0%. There were 85 patients with HbA1c more than 7.0% and 85 patients with HbA1c less than 7.0%. The selection of study participants was done by systematic random sampling with every fourth patient being enrolled for the study, thus 21 patients were identified for each group.
A 5ml of blood was collected in a trace element free vacutainer irrespective of when the last meal was taken. The sample was centrifuged at 2000g within one hour of collection. Serum chromium was estimated using inductively coupled Plasma – Optical Emission Spectrophotometer (ICP- OES) which is a sequential plasma emission instrument. From the observed spectrophotometric values, serum chromium concentration was estimated. The values of serum chromium were expressed in mcg/L.
Statistical Analysis
Data obtained were compared between well controlled and uncontrolled type 2 diabetic individuals using unpaired t – test for significance at 95% confidence levels. Variables like BMI, Systolic and Diastolic Blood Pressure were also analysed. The mean serum chromium levels were also categorized age wise. Statistical analysis was done using IBM – SPSS 20 for Windows statistical software.
Results
The present study had 13 males (62%) and 8 females (38%) in each group [Table/Fig-1] with a mean age of 46.71± 8.3 years in group 1 and 49.1±6.7 years in group 2. Though systolic and diastolic blood pressures were with in normal limits in both groups, average BMI revealed “overweight” in uncontrolled group [Table/Fig-2].
Descriptive data for controlled and uncontrolled diabetic group
| Data | Controlled Diabetic Patients | Uncontrolled Diabetic Patients |
|---|
| Number of subjects (n) | 21 | 21 |
| Age (In Years) | 46.71 ± 8.3 | 49.1 ± 6.71 |
| Sex |
| Male | 13 (62%) | 13 (62%) |
| Female | 8 (38%) | 8 (38%) |
The Mean±SD values for some variables of the studied group
| Variables | Controlled Diabetic group (n = 21) | Uncontrolled Diabetic group (n = 21) |
|---|
| Body Mass Index – BMI (Kg/ m2) | 25.96 ± 3.27 | 27.94 ± 3.03 |
| Systolic BP (mm of Hg) | 119.33 ± 4.07 | 125.14 ± 5.20 |
| Diastolic BP (mm of Hg) | 79.33 ± 3.43 | 81.05 ± 4.27 |
| Glycated Haemoglobin HbA1c (%) | 7.04 ± 0.69 | 10.32 ± 1.72 |
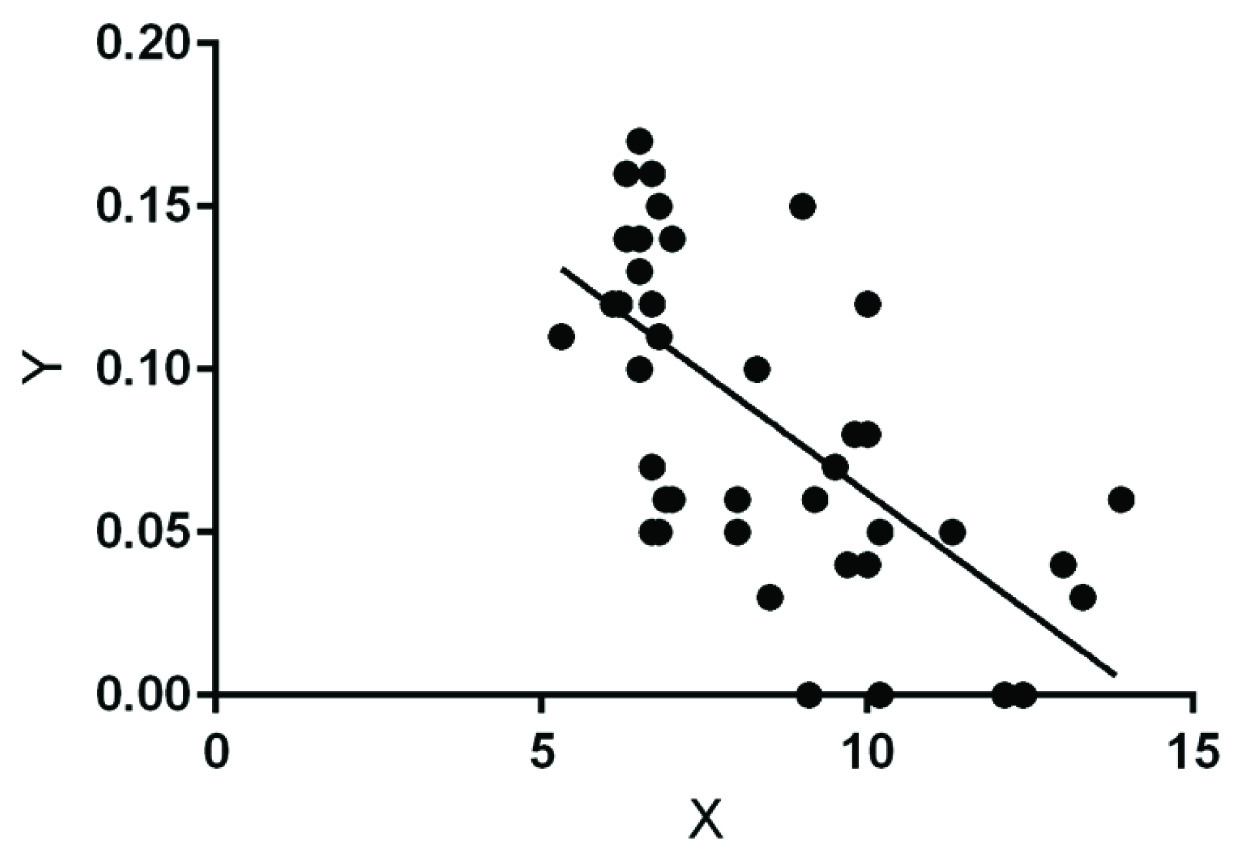
The mean chromium concentration in the controlled and uncontrolled group was 0.103 ± 0.04mcg/L and 0.065 ± 0.03 mcg/L respectively [Table/Fig 3]. This indicates a significant decrease in mean serum chromium concentration in uncontrolled type 2 diabetic patients when compared with controlled type 2 diabetic patients (p=0.0012). There was a decrease in the mean serum chromium levels in both the groups with increasing age. This difference was statistically significant in age groups above 40 years [Table/Fig 4]. In our study the mean serum chromium levels were lower in females when compared to males which was however insignificant (p=0.3487) [Table/Fig-5]. The correlation analysis between serum HbA1c levels and serum chromium concentrations using linear regression showed a significant inverse relationship (r = -0.6514, p < 0.0001), [Table/Fig-6].
Mean Serum chromium concentration in our study group
| Serum Chromium concentration | Controlled Diabetic patients (n = 21) | Uncontrolled Diabetic patients (n = 21) |
|---|
| Mean ± SD (mcg/l) | 0.103 ± 0.04 | 0.065 ± 0.03 |
Age wise distribution of serum chromium concentration
| Age (In Years) | Serum Chromium level (mcg/l) |
|---|
| Controlled Diabetic group | Uncontrolled Diabetic group |
|---|
| 31 - 40 | 0.1 ± 0.05 | 0.08 ± 0.06 |
| 41 - 50 | 0.1 ± 0.03 | 0.07 ± 0.02 |
| 51 - 60 | 0.09 ± 0.05 | 0.06 ± 0.02 |
Gender wise distribution of serum chromium levels
| Sex | Serum Chromium level (mcg/l) |
|---|
| Controlled Diabetic group (n = 21) | Uncontrolled Diabetic group (n = 21) |
|---|
| Female | 0.1038 ± 0.04 | 0.059 ± 0.02 |
| Male | 0.1025 ± 0.047 | 0.074 ± 0.04 |
Scatter plot showing HbA1c values and serum chromium concentrations with the line of best fit.
[r = -0.6514, R2 = 0.4243, Y = –0.01468*X + 0.2087, p < 0.0001, F=29.48 DFn=1 DFd=40]
Discussion
The present study suggests that type 2 diabetic have a lower serum chromium levels when compared to healthy individuals (0.08 mcg/L vs 0.05 – 0.5mcg/L). This is similar to observations reported from earlier studies [11–14]. However, the minimum serum chromium value found in our study was lower than the lowest value reported by a number of studies carried out in the Western countries [13,14]. The daily intake of chromium may be sufficient in western countries whereas Asian foods may be deficient in chromium or have substances inhibiting its absorption, which might account for lower serum chromium concentration among Asians [13].
Diwan et al., compared serum chromium level using Atomic Absoption Spectrophotmetry (AAS) in Indian diabetics and healthy controls and found that chromium levels were undetectable in both the groups; though this may also be due to the limitations of the method (AAS) used. Such undetectable range of serum chromium may also implicate profound deficiency of chromium among the diabetics and its important role in the pathogenesis of diabetic complications [12]. In the present study the use of ICP – OES for estimating serum chromium levels, which is more sensitive incomparison to AAS utilized in most of the Indian studies, minimized the blood requirement for estimation and gave us measurable values. However, in a study by Ghosh et al., it was found that chromium levels in non diabetic Indian population was higher when compared with those with diabetes and the response to insulin improved with chromium supplementation [11]. This probably suggests geographical variations even within the country.
In this study, there was a decrease in serum chromium level as the age increased; this finding reflects the findings of Ding et al., from China who showed that elderly diabetics have a significantly lower levels of serum chromium [13]. Throughout the world, siginificant number of people have deficient serum levels of chromium without any clinically evident state of chromium deficiency [2]. Volpe et al., demonstrated that chromium supplementation has no significant effect on insulin, glucagon or C-peptide levels in normal population in contrast to those with diabetes [14]. But chromium levels dip further in those with diabetes, especially in those who are uncontrolled and about to go into complications [15].
The present study showed that the mean serum chromium levels were lower in uncontrolled group (0.065 ± 0.03 mcg/l) when compared to the well controlled group (0.103 ± 0.04 mcg/l) and this difference was statistically significant (p = 0.0012). A lower mean serum chromium value was noticed among females when compared to males in both groups (0.09 ± 0.05 vs 0.08 ± 0.05), which was however not statistically significant (p=0.3487). This is in line with studies by Olsen et al., and Nsonwu et al., which showed no significant difference in chromium levels between males and females [16,17]. An Indian study among pregnant females by Sundararaman et al., showed that women with gestational Diabetes Mellitus (GDM) showed lower levels of serum chromium as compared to pregnant women without GDM [10]. Another study by Hasan et al., showed that postmenopausal women with type 2 diabetes mellitus have lower serum chromium levels [18]. Though effects of chromium supplementation on glycaemic control varies in different studies across the world, as was in many Indian studies, the present study also depicted low serum chromium levels in well controlled diabetic patients and a much lower levels in uncontrolled diabetic patients.
The oxidative stress in retina during an episode of diabetic hyperglycaemia leads to retinal basement membrane thickening, the hallmark of microangiopathy, seen in diabetic retinal disease [19]. The retina is rich in polyunsaturated lipid membrane making it sensitive to oxygen free radicals and lipid peroxidation inducing vascular leakage, increase in retinal vascular permeability and perhaps causing vision loss due to diabetic retinopathy [20].
A recent experimental study found that chromium supplementation in streptozotocin induced diabetic mice resulted in improvement in retinal disruption when compared with nonsupplemented mice. Significant upregulation in insulin, GLUT-1 and GLUT-3, which regulate glucose uptake in all mammalian cells, were noted in diabetic retina and this was reversed when treated with chromium supplementation [21]. These findings point to the need to assess the role of chromium supplementation in diabetics to avoid or delay microvascular and macrovascular complications. Hence the lower level of chromium in uncontrolled diabetics when compared with controlled diabetics in the present study, maybe a warning of the impending microvascular complications, especially diabetic retinopathy in those individuals.
Based on the results of our small study, we wish to recommend that large scale cohort studies within the diabetic population itself must be carried out to verify and establish our results before recommending chromium supplementation for diabetics. This is because cell culture studies have indicated the possibility of DNA damage in addition to serious side effects like kidney damage associated with supraphysiological doses of Chromium picolinate, the most absorbable form so far. In addition, a meta analysis by Althuis et al., suggests no role for chromium supplementationin type 2 diabetic who do not have dietary deficiency of chromium [22].
Limitations
The limitations of our study were the small target population, exclusion of persons with complications, absence of normal controls, prediabetic patient groups and dietary habits were not taken into account.
Conclusion
Serum chromium levels were reduced in type 2 diabetes mellitus patients irrespective of their HbA1c values. The levels of chromium were reduced to a more significant level in uncontrolled type 2 diabetic when compared to controlled type 2 diabetic. As in many previous studies, the present study also noted that as the age of the study population increased, serum chromium levels were more markedly reduced. Hence role of maintaining chromium levels in delaying microvascular complications in diabetics needs to be investigated further, though current evidence is not adequate to recommend supplementation of chromium. Though the difference between the study groups was statistically significant, it is very early to suggest chromium supplementation in patients with low levels of chromium. In future, similar large scale studies need to validate the similar results in the community in order to consider chromium supplementation to diabetic patients.