Background
Dentinal hypersensitivity is a commonly observed problem after periodontal treatment procedures in periodontal patients. This further complicates preventive oral hygiene procedures by patients which jeopardize periodontal treatment, or even may aid in periodontal treatment failure.
Aims and Objectives
The aims and objectives of present study were to assess the problem of dentine hypersensitivity after non-surgical periodontal treatment and selection of cases for evaluation of commercially available milk at room temperature as mouth rinse for the treatment of dentinal hypersensitivity caused by periodontal treatment.
Materials and Methods
Patients were selected randomly for nonsurgical periodontal treatment and then were assessed for dentine hypersensitivity. Those having dentine hypersensitivity were assigned in two groups. Group one patients were advised to rinse with commercially available milk at room temperature, group two patients were advised to rinse with luke warm water as control. A four point Verbal Rating Score (VRS) was designed to record the numerical value of dentine hypersensitivity.
Results
The results show incidence of 42.5% and prevalence of 77.5% for dentine hypersensitivity after periodontal treatment procedures. After rinsing with milk following periodontal treatment procedures, there was found a significant reduction of dentine hypersensitivity with probability by unpaired t-test as 0.0007 and 0.0001 at tenth and fifteenth day post periodontal treatment procedures respectively.
Conclusion
This study demonstrated that the milk rinse is a suitable, cheaper, fast acting, home-use and easily available solution to the problem of dentine hypersensitivity after non-surgical periodontal treatment. Milk can be used as desensitizing agent and rinsing with milk for few days is effective in quick reduction of dentine hypersensitivity due to periodontal treatment procedures.
Cemental, Dental, Dentinal, Enamel, Hypersensitivity, Milk rinse, Milk, Periodontal, Procedures, Root planing, Root, Scaling, Sensitive teeth, Surgical, Sensitivity, Tooth, Treatment
Introduction
Dentine hypersensitivity (DH) is one of the most common clinical problems faced by the clinician to which there is no definitive treatment. It clinically can be described as an exaggerated response of exposed dentine to application of a stimulus, regardless of its location [1,2]. Dentin and pulp originate from ectomesenchyme but histologically they are different tissues [3]. Pulp is confined in the dentine and any physiologic and/or pathologic changes in one of the tissues will affect the other [4].
The literature has suggested various other terms for this clinical problem as cervical dentine sensitivity (CDS), cervical dentine hypersensitivity (CDH), dentine sensitivity (DS) or root dentine sensitivity (RDS), root dentine hypersensitivity (RDH), although, the term dentine hypersensitivity (DH) is the most preferred in the published literature. The European Federation of Periodontology [5] recently suggested root sensitivity (RS) to describe tooth sensitivity associated with periodontal disease and treatment. Von troil et al., could not find sufficient data available to accept term root sensitivity (RS) for hypersensitivity following periodontal therapy [6]. However, the literature suggested that dentine hypersensitivity following periodontal treatment among individuals with periodontal disease and treatment may have a higher prevalence than reported [7].
It was observed that after the periodontal treatment, complaints of dentine hypersensitivity are usually high. This further complicates preventive oral hygiene procedures by patients and prevents them from maintaining good oral hygiene which jeopardize periodontal treatment or may even aid in periodontal treatment failure.
Two phases are proposed in the pathogenesis of DH namely lesion localization and lesion initiation [8]. Lesion localization is loss of protective covering over the dentin like loss of enamel via attrition, abrasion, erosion or abfraction and gingival recession, which exposes it to external oral environment. Gingival recession can be due to toothbrush abrasion, pocket reduction surgery, tooth preparation for crown, excessive flossing or secondary to periodontal diseases [9]. For DH to occur, the lesion localization has to be initiated. Lesion initiation occurs after the protective covering of smear layer is removed causing exposure and opening of dentinal tubules, which culminates in lesion localization and DH [4].
Recent in the development of desensitizing agents, milk protein casein has been used to develop a remineralizing agent named GC Tooth Mousse (Recaldent, GC Corp, Japan). This milk protein casein phosphor-peptide (CPP) contains phosphoseryl sequences which by attaching with amorphous calcium phosphate (ACP) of teeth forms stabilized CPP–ACP. This stabilized CPP-ACP prevents the dissolution of calcium and phosphate ions and maintains a supersaturated solution of bioavailable calcium and phosphates [4]. It has also been shown that this stabilized CPP–ACP can effectively remineralize the subsurface enamel lesions [4]. This remineralizing capacity of CPP can also help in prevention and treatment of DH [4]. Cai F et al., proposed in his study that incorporation of casein phosphopeptide-amorphous calcium phosphate nanocomplexes (CPP-ACP) into lozenges significantly increases enamel subsurface lesion remineralization [10]. S Lata et al., concluded that amorphous calcium phosphate- casein phosphopeptide (CPP-ACP) GC Tooth Mousse, Recaldent, GC Corp, Japan, in cream form is less effective than fluoride varnish for enamel subsurface remineralization [11]. Ruchi Vashisht et al., in ex-vivo study on artificial early enamel lesions concluded that casein phosphopeptide amorphous calcium phosphate has the significant potential to remineralize the early enamel lesions [12].
Aims and Objectives
The Periodontal disease is very common in the general population and most of the patients seek treatment either in the form of nonsurgical or surgical periodontal therapy. It was observed that after periodontal treatment procedures, patients usually start complaining of hypersensitive teeth which may make them reluctant for oral hygiene preventive procedures and further periodontal treatment as well. The consequence of it may result in poor periodontal health.
The aims and objectives of this study were to assess the dentine hypersensitivity after non- surgical periodontal treatment procedure and selection of cases for evaluation of commercially available milk at room temperature as mouth rinse for treatment of dentine hypersensitivity following periodontal treatment procedures and finding a suitable, cheaper, fast acting, home-use and easily available solution to the problem.
Materials and Methods
The present study was conducted in specialty clinic of periodontics in College of Dentistry, Jazan University, Kingdom of Saudi Arabia. Periodontal specialist randomly selected the samples for thorough scaling and root planing for the study. Every selected case was having the diagnosis of moderate to severe chronic periodontitis. Systemically healthy patients were included in the study. Those with unrestored carious lesions and periodontal treatment in the last four month period were excluded from the study. Patients with current desensitizing therapy or had received professionally applied desensitizing treatment during four months prior to the study were also excluded.
After obtaining informed consent, 40 patients were randomly selected and checked for baseline dentine hypersensitivity (DH) scores. These patients were assigned group A (GA). After performing non-surgical periodontal procedure (scaling and root planing), these same patients were assigned group B (GB) and again checked for DH on second day (Visit I) of post procedure.
On the first visit (second day) after scaling and root planing, only 31 patients having dentine hypersensitivity were selected for the study and divided randomly into two groups namely group one (G1) and group two (G2). Seventeen patients were kept in G1 and fourteen in G2. Both group patients were instructed to return for follow up on 4th, 10th and 15th day post-treatment. Scores of dentine hypersensitivity at second day (visit-I) post treatment were considered as baseline for the study. At the first visit (second day) after treatment procedure, G1 patients were advised to rinse oral cavity with 30 ml commercially available milk at room temperature five times daily for five minutes for fifteen days and, G2 patients were advised to rinse with 30 ml luke warm water for five minutes, five times a day for fifteen days. The patients were instructed not to eat/drink for 30 minutes after rinse and not to use any other desensitizing agents and/or pain killers, during the study period.
A 4 point Verbal Rating Scale (VRS) was designed for this study. It is a clinical scale to find out the numerical values of the clinical problem of dentine hypersensitivity. It was described to find the values of dentine hypersensitivity as follows:
Score 1 – No hypersensitivity – No discomfort to thermal changes after drinking water at room temperature or cold water.
Score 2 – Mild hypersensitivity – Mild discomfort after drinking water at room temperature and cold water.
Score 3 – Moderate hypersensitivity – Moderate discomfort after drinking water at room temperature but cannot drink cold water.
Score 4 – Severe hypersensitivity – Pain after drinking water at room temperature. Pain on breathing. Cannot tolerate cold water (severe pain).
We have used the term dentine hypersensitivity (DH) for the problem described, throughout in our manuscript.
Statistics Analysis
The results were tabulated and analyzed using two tail paired Student’s t-test for GA and GB patients and two tail independent t-tests (unpaired student’s t-test) for G1 and G2 subjects using following internet website. http://www.physics.csbsju.edu/stats/t-test.html
Results
The result of paired Student’s t-test and statistics for GA and GB patients with DH at baseline pretreatment procedure and at second day post-periodontal treatment procedure (visit I post procedure) are shown in [Table/Fig-1].
| Scores of DH | Baseline DHPre-Periodontal Procedure(*GA) | DH at second Day Post-treatment Procedure(Visit I) (*GB) |
|---|
| Number ofPatients | % ofPatients | Number ofPatients | % ofPatients |
|---|
| Score 1 | 25 | 62.5 | 9 | 22.5 |
| Score 2 | 15 | 37.5 | 4 | 10 |
| Score 3 | 0 | 0 | 26 | 65 |
| Score 4 | 0 | 0 | 1 | 2.5 |
| Total | 40 | 100 | 40 | 100 |
| Incidence | 42.5 |
| Prevalence | 77.5 |
| Mean | 1.38 | 2.48 |
| 95% confidence interval for Mean | 1.218 thru 1.532 | 2.195 thru 2.755 |
| Standard Deviation | 0.490 | 0.877 |
| Median | 1.00 | 3.00 |
| Average Absolute Deviation from Median | 0.375 | 0.575 |
| t-value | -9.35 |
| Degree of Freedom | 39 |
| Probability | <0.05 |
* GA= Group A (Pre-procedure Patients group), GB= Group B (Post-procedure Patients group)
The results of the unpaired Student’s t-test for G1 and G2 at 95% confidence interval are summarized in the [Table/Fig-2] as follows:
Follow up Visits for G1 and G2 Patients.
| Parameters | Visit I(2nd Day) | Visit II(4th Day) | Visit III(10th Day) | Visit IV(15th Day) |
|---|
| *MeanG1 | 2.94 | 2.53 | 1.68 | 1.12 |
| **MeanG2 | 2.86 | 2.64 | 2.5 | 2.36 |
| t-value | 0.581 | -0.620 | -3.77 | -8.29 |
| Sdev | 0.401 | 0.507 | 0.626 | 0.414 |
| Probability | 0.57 | 0.54 | 0.0007 | 0.0001 |
Critical value at 95% level of significance for two tail t-test is 2.05 (p<0.05).
*MeanG1 – Mean of scores of group one (G1) at different visits.
**MeanG2 – Mean of scores of group two (G2) at different visits.
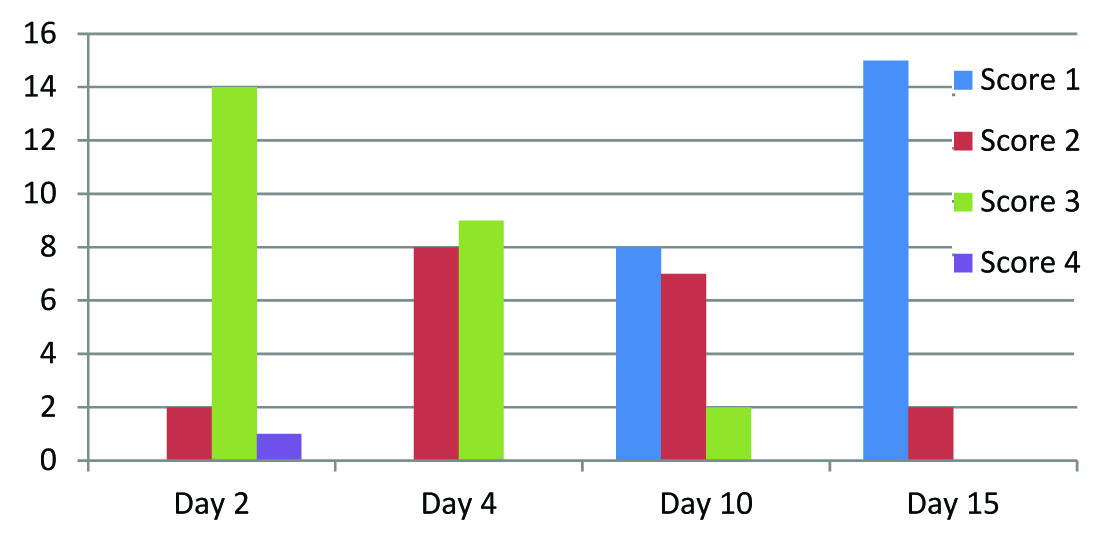
The original data analysis of the results for G1 and G2 patients groups is shown in [Table/Fig-3,4] as follows:
| No. of Visits | Score 1 | Score 2 | Score 3 | Score 4 |
|---|
| Visit I (2nd Day) | 0 | 2 (11.77%) | 14 (82.35%) | 1 (5.88%) |
| Visit II (4th Day) | 0 | 8 (47.06%) | 9 (52.94%) | 0 |
| Visit III (10th Day) | 8 (47.06%) | 7 (41.18%) | 2 (11.77%) | 0 |
| Visit IV (15th Day) | 15 (88.24%) | 2 (11.77%) | 0 | 0 |
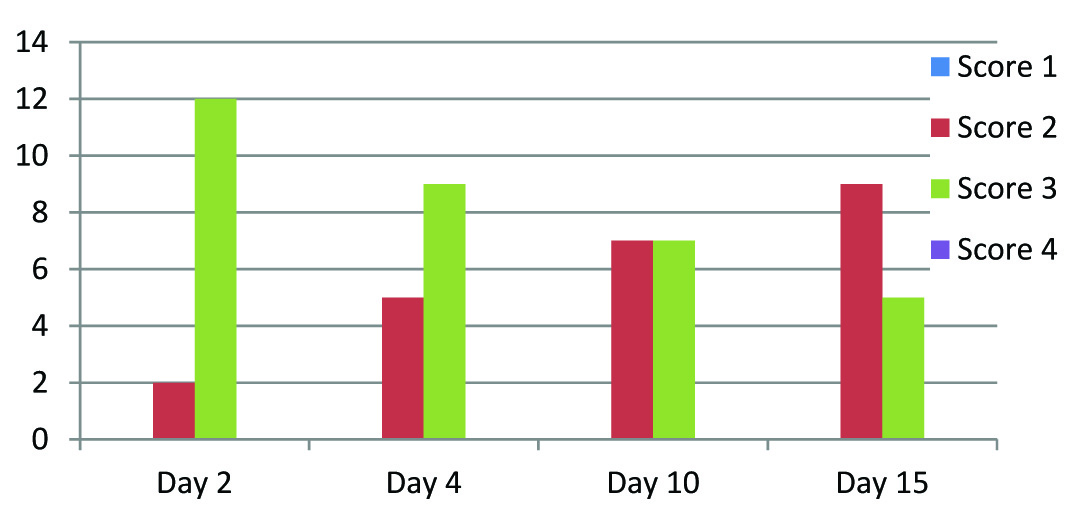
| No. of Visits | Score 1 | Score 2 | Score 3 | Score 4 |
|---|
| Visit I (2nd Day) | 0 | 2 (14.29%) | 12 (85.72%) | 0 |
| Visit II (4th Day) | 0 | 5 (35.72%) | 9 (64.29%) | 0 |
| Visit III (10th Day) | 0 | 7 (50%) | 7 (50%) | 0 |
| Visit IV (15th Day) | 0 | 9 (64.29%) | 5 (35.72%) | 0 |
Bar diagram representation tables: The results are depicted as bar diagram as follows [Table/Fig-5,6].
Cases with Luke warm water (G2)
Discussion
Periodontal therapy in the form of nonsurgical and surgical procedure is common and patients usually report discomfort/pain immediately following these procedures. Post-periodontal treatment procedure, dentine hypersensitivity is a common clinical condition and complaint. Discomfort and sometimes pain caused by DH may refrain a person from establishing and maintaining adequate oral hygiene, which further may complicate oral health. Dentine hypersensitivity is characterized by a sharp pain or discomfort arising as an overt response to thermal, chemical or osmotic stimuli which cannot be explained as arising from any other disease or dental problems [1,13]. Dentine hypersensitivity is caused due to exposeure of dentine after the enamel or cementum at the root surface has been lost by the treatment, underlying dental and gingival diseases or physiologic wear and tear of the teeth. Presence of gingival recession and loss of enamel exposes underlying cementum and dentine respectively which get abraded, worn or erode more quickly than enamel, as dentine and cementum have lower inorganic mineral contents than enamel so dentine abrades 25 times faster than enamel and cementum abrades 35 times faster [14].
B Von Triol et al., in their review described dentine hypersensitivity as a short and sharp, painful response to an external stimulus applied to exposed dentine (Chabanski & Gillam, Holland et al.,) [6,15,16]. B Von Troil found a prevalence of root sensitivity of 9-23% and 54-55% before and after periodontal therapy respectively and proposed that it occurs in approximately half of the patients following subgingival scaling and root planing and its intensity increases for a few weeks after therapy and decreases afterwards [6].
Dentine is a living tissue consisting of organic and inorganic components. Within the dentine, dentinal tubules run from the pulp to the outer dentinal surfaces. Brannstrom’s Hydrodynamic theory of fluid displacement within the dentinal tubules is the most accepted theory of dentinal hypersensitivity. The fluid movement within dentinal tubules stimulates the A-delta fibers resulting in the well localized sharp pain perceived as dentine hypersensitivity [6,17].
Over the years many treatment modalities of dentine hypersensitivity with varying outcomes have been reported but none provide definite conclusion as to which treatment is superior. They are either in-office procedures or self-administered for at home-use. These methods function through blocking the pain response either by occluding the dentinal tubules or by preventing the neural transmission. Even a large number of published studies are not able to provide a gold standard of treatment or product for treatment of dentinal hypersensitivity.
DG Gillam and R Orchardson stated that the individuals with periodontal disease have higher prevalence of dentinal hypersensitivity after periodontal therapy such as scaling and root planing procedures as compared to those presenting with healthy mouths and gingival recession [18]. Tammaro et al., concluded that successful periodontal treatment can be accomplished through good oral hygiene self-care measures, and by nonsurgical and surgical periodontal therapies which have unwanted side effects including gingival recession, exposure of underlying dentine following root cementum denudation with the risk of experiencing tooth sensitivity [19]. Acidic foods and drinks can change the oral environment which can dissolve the newly created smear layer [20].
The purpose of this study was to assess the dentine hypersensitivity after non-surgical periodontal treatment (scaling and root planing) and clinically evaluate the effectiveness of milk rinse as a desensitizing agent for post scaling and root planing dentine hypersensitivity. The values of DH at first visit are shown in [Table/Fig-1], which gives an estimate of 77.5% of DH after non-surgical periodontal therapy [Table/Fig-1]. This predicts about 42.5% incidence and 77.5% prevalence of DH after scaling and root planing procedure. Probability for patients of G1 is 0.0001 (p<0.05) at 15th day and a critical value of 2.05 at 95% confidence interval which strongly rejected null hypothesis and suggested strongly positive results for the treatment of DH with milk rinse [Table/Fig-2]. Therefore, it is evident from this study that at fifteenth day, the DH has reduced considerably (88.24% G1 cases has given score 1) and only 11.77% cases were having mild hypersensitivity (score 2) [Table/Fig-3] while at fifteenth day mild and moderate hypersensitivity cases from G2 patients were considerably high (64.29% and 35.72% respectively) [Table/Fig-4].
Milk is a mixture of emulsions, colloids, molecular and ionic solutions. Fresh milk has a pH of 6.7 and is slightly acidic. Milk is also an excellent buffering solution which can resist a change in pH on addition of acid or alkali. When the pH of milk is changed, the acidic or the basic groups of the milk proteins will be neutralized. With the fall of the pH of milk, the charge on the casein also falls and it precipitates. Milk comprises less than 1% salts mainly in the form of chlorides, phosphates, citrates of calcium, sodium and magnesium. Calcium, magnesium, phosphorus and citrates are distributed between the soluble and colloidal phases. Equilibria of salts in milk are altered by heating, cooling and change in pH. Milk also contains various enzymes like phosphatases, lipases, peroxidases and catalases etc [21].
It is proposed from this study that scaling and root planning may itself create a smear layer that could be supplemented by natural dentinal tubules mineralization process through frequent milk rinsing. Rinsing with milk may provide the rich bioavailability of calcium and phosphate which can aid in remineralization, acid buffer and reduce the acidic effect of plaque on tooth structure. Milk also contains immunoglobulins [22], which may provide defenses against plaque microorganisms.
Milk rinse could be an effective, suitable, cheaper, fast acting, easily available and home use substitute for dentine hypersensitivity. Thus, the results of this study suggested and indicated that dentine hypersensitivity in most of the cases occurs invariably after non-surgical periodontal treatment and rinsing with milk is very effective in reducing the dentine hypersensitivity after periodontal treatment procedures. This study clearly establishes the desensitizing therapeutic benefit of milk rinsing following non-surgical periodontal treatment.
Further studies are required to know the mechanism of milk rinse in prevention and treatment of dentine hypersensitivity. There are no other comparable studies available for milk rinse in the treatment of dentine hypersensitivity after periodontal treatment.
Conclusion
The present study demonstrated clearly that the rinsing with 30 ml milk at room temperature five times daily for few days is effective in reducing dentine hypersensitivity after periodontal treatment procedures. Milk is a suitable, cheaper, fast acting, home-use and easily available solution to the problem of dentine hypersensitivity and can be used as desensitizing agent for dentine hypersensitivity due to periodontal treatment procedures.
Abbreviations
*MeanG1: Mean of scores of group one at different visits.
**MeanG2: Mean of scores of group two at different visits.
* GA= Group A (Pre-procedure Patients group), GB= Group B (Post-procedure Patients group)
Critical value at 95% level of significance for two tail t-test is 2.05 (p<0.05).
*MeanG1 – Mean of scores of group one (G1) at different visits.
**MeanG2 – Mean of scores of group two (G2) at different visits.
[1]. Addy M, Dentine hypersensitivity: Definition, prevalence, distribution and etiology. In: Addy M, Embery G, Edgar WM, Orchardson R, editorsTooth wear and sensitivity: Clinical advances in restorative dentistry 2000 LondonMartin Dunitz:239-248. [Google Scholar]
[2]. Addy M, Etiology and clinical implications of dentine hypersensitivityDent Clin North Amer 1990 34:503-14.[PubMed: 2197124] [Google Scholar]
[3]. Orchardson R, Cadden SW, An update on the physiology of the dentine-pulp complexDent Update 2001 28:200-09.[PubMed: 11476036] [Google Scholar]
[4]. Miglani S, Aggarwal V, Ahuja B, Dentin hypersensitivity: Recent trends in managemenJ Conserv Dent 2010 13(4):218-24.[doi: 10.4103/0972-0707. 73385 PMCID: PMC3010026.] [Google Scholar]
[5]. Sanz M, Addy M, Group D SummaryJournal of Clinical Periodontology 2002 29(suppl 3):195-96. [Google Scholar]
[6]. Von Troil B, Needleman I, Sanz M, A systematic review of the prevalence of root sensitivity following periodontal therapyJ Clin Periodontol 2002 29(Suppl. 3):173-77. [Google Scholar]
[7]. Lin YH, Gillam DG, The prevalence of root sensitivity following periodontal therapy: a systematic reviewInternational Journal of Dentistry 2012 2012:40702312 pages, 2012. doi:10.1155/2012/407023 [Google Scholar]
[8]. Orchardson R, Gilliam D, Managing dentin hypersensitivityJ Am Dent Assoc 2006 137(7):990-98.quiz 1028-9. [PubMed: 16803826] [Google Scholar]
[9]. Dababneh R, Khouri A, Addy M, Dentine hypersensitivity: An enigma? A review of terminology, epidemiology, mechanisms, aetiology and managementBr Dent J 1999 187:606-11.[PubMed: 16163281] [Google Scholar]
[10]. Cai F, Shen P, Morgan MV, Reynolds EC, Remineralization of enamel subsurface lesions in-situ by sugar free lozenges containing casein phosphopeptide – amorphous calcium phosphateAust Dent J 2003 48:240-43.[PubMed: 14738126] [Google Scholar]
[11]. Lata S, Varghese NO, Varughese JM, Remineralization potential of fluoride and amorphous calcium phosphate-casein phospho peptide on enamel lesions: An In vitro comparative evaluationJ Conserv Dent 2010 13(1):42-6.[PMCID: PMC2883807] [PubMed: 20582219]. doi: 10.4103/0972-0707.62634 [Google Scholar]
[12]. Vashisht R, Kumar A, Indira R, Srinivasan MR, Ramachandran S, Remineralization of early enamel lesions using casein phosphopeptide amorphous calcium Phosphate: An ex-vivo studyContemp Clin Dent 2010 1(4):210-13.doi: 10.4103/0976-237X.76385 [Google Scholar]
[13]. Canadian Advisory Board on Dentin Hypersensitivity Consensus-based recommendations for the diagnosis and management of dentin hypersensitivityJ Can Dent Assoc 2003 69:221-26. [Google Scholar]
[14]. Kim JL, Karastathis D, Dentinal hypersensitivity management. In: Darby ML, Walsh MMDental Hygiene Theory and Practice 2010 3rd edSt. Louis, MOSaunders-Elsevier:726-35. [Google Scholar]
[15]. Chabanski MB, Gillam DG, Aetiology, prevalence and clinical features of cervical dentine sensitivityJournal of Oral Rehabilitation 1997 24:15-19. [Google Scholar]
[16]. Holland GR, Närhi MN, Addy M, Gangarosa L, Orchardson R, Guidelines for the design and conduct of clinical trials on dentine hypersensitivityJournal of Clinical Periodontology 1997 24:808-13. [Google Scholar]
[17]. Burwell A, Jennings D, Muscle D, NovaMin® and dentin hypersensitivity – In vitro evidence of efficacyJ Clin Dent 2010 21(Spec Issue):66-71. [Google Scholar]
[18]. Gillam DG, Orchardson R, Advances in the treatment of root dentine sensitivity: mechanisms and treatment principlesEndodontic Topics 2006 13:13-33. [Google Scholar]
[19]. Tammmaro S, Wennstrom JL, Bergenholtz G, Root–dentin sensitivity following non-surgical periodontal treatmentJ Clin Periodontol 2000 27:690-97. [Google Scholar]
[20]. Pashley DH, Smear layer: overview of structure and functionProc Finn Dent Soc 1992 88(Suppl 1):215-24. [Google Scholar]
[21]. Bylund G, The chemistry of milkDairy processing handbook/chapter 2 1995 Printed in [Google Scholar]
[22]. El-Loly MM, Bovine milk immunoglobulins in relation to human healthInternational Journal of Dairy Science 2007 2:183-95. [Google Scholar]