Though the concept of neutral zone in making complete denture and its significance are well known, the material of choice has always been experimented to achieve better results. Recording of neutral zone using irreversible hydrocolloid (Alginate) as a material of choice would make the way of recording the neutral zone easier, as well as comfortable for the patient, when compared with other materials used for the purpose. This article describes the method of recording the biometric denture space (neutral zone) using hydrocolloid impression material which is most commonly used in everyday dental practice.
Alginate, Complete dentures, Potential denture space, Resorbed ridges, Zone of minimal conflict
Case Report
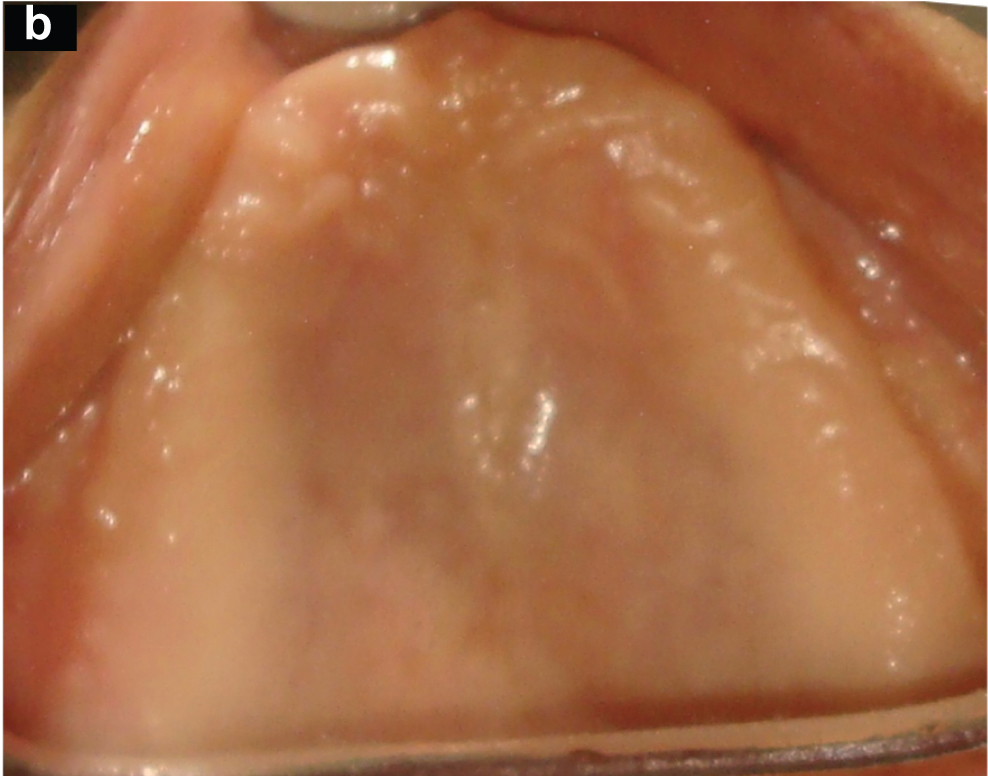
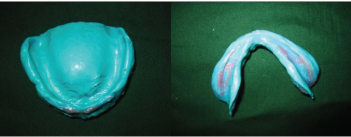
A 70-year-old, female patient, reported to the dental hospital, with a complaint of ill fitting denture. These dentures were fabricated by conventional technique six months ago and were unsatisfactory. On examination patient had an adequate maxillary ridge and severely resorbed mandibular ridge [Table/Fig-1a,b]. Therefore the concept of Biometric dentures or neutral zone (NZ) dentures was adopted for fabrication.
Lower resorbed residual ridge

Steps in fabrication of complete denture based on neutral zone recording: Primary Impression & Diagnostic Casts.
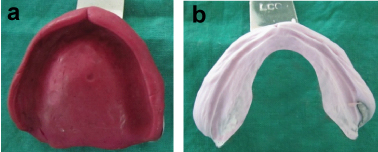
Primary impressions were made using impression compound (Pyrax) and the lower impression was relined using alginate (Tropicalgin- Zhermack) for more accurate recording of details [Table/Fig-2a,b]. The diagnostic casts were fabricated using type II dental stone (Kalstone, Kalabhai Karson Pvt. Ltd, Mumbai, India) [1].
Primary Impression (a)upper arch with impression compound, (b) lower arch with impression compound relined with alginate impression material
Record Base Fabrication and its modification
Using the diagnostic casts, record bases were fabricated using autopolymerising resin (DPI Self Cure, Dental Products of India, Mumbai, India) and occlusal rims were constructed over the record bases with modelling wax (The Hindustan Dental products, Hyderabad, India).
A tentative jaw relationship was performed and the records were transferred on to a mean value articulator. After casts were mounted, tentative records were removed and new denture bases were fabricated using over autopolymerising resin. In order to maintain the vertical dimension while being transferred to the patient’s mouth, occlusal stops were designed using plastic straws filled with autopolymerising resin bilaterally in the canine and first molar region connecting maxillary and mandibular record bases [Table/Fig-3].
Recorded bases are tried in the patient’s mouth, with the vertical stops establishing the vertical dimension

Neutral zone recording
A hydrocolloid impression material– Alginate (AccuTray, Ivoclar) was chosen as a material of choice.
The record bases were checked in the patient’s mouth for stability, while movements like swallowing and pursing of lips were made to be performed by the patient. After sufficient training alginate was loaded on the record base and inserted into the patient’s mouth. The patient was asked to perform movements like sucking, swallowing and exaggerated ‘EEE’ and ‘OOO’ sounds repeatedly. The alginate was maintained in position by the modified tray design with vertical supports [2].
The excess material was trimmed with the help of curved scissors [Table/Fig-4] and the anatomical structures were used as guidelines to mark the references plane. Anteriorly the vermillion border of the lower lip, corner of the mouth and posteriorly the retromolar pad were taken as reference points and occlusal plane was drawn using an indelible (eosin) pencil. Care was taken to note the incisal exposure of the patient which dictates the aesthetics of the finished denture [Table/Fig-5].
Trimming of excess alginate

Marking of occlusal plane

The Plaster Index
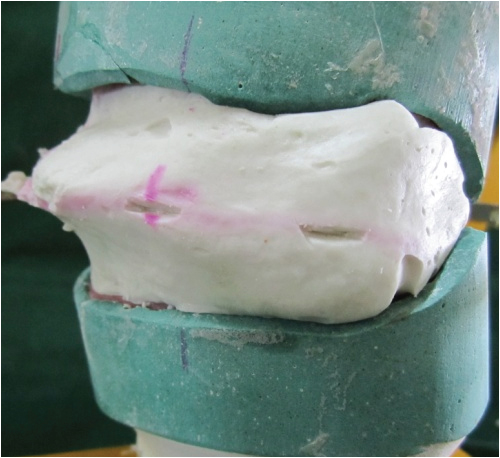
Before indexing it was necessary to create small notches over the occlusal plane on the moulded alginate surface [Table/Fig-6], which acts as orientation grooves or reference marks on the fabricated wax rims [Table/Fig-7].
Recorded impression of denture space is transferred onto the cast
Occlusal rims mounted onto their respective casts
Dental plaster (type II) was first painted over the alginate surface. Then thick patty plaster was mixed and stabilised over the obtained impression surface. Since alginate has a desirable but limited range of dimensional stability, laboratory procedures were performed with in the stipulated time of 10 to 15 minute. Once the plaster had set, it was sectioned using a die cutting model saw (Yeti) and separated as anterior and posterior sections. The alginate was then removed and the plaster index was reassembled. Elastics were used for stabilising the plaster index. Modelling wax (The Hindustan Dental products, Hyderabad, India) was softened over direct flame, melted and poured into the mould space [3].
Arrangement of teeth and try-in
The notches created over the occlusal plane reflect on the set occlusal rims. Casts with the wax rims were then articulated and teeth setting following the setting principles were done within the confines of the mould space, the biometric denture space.
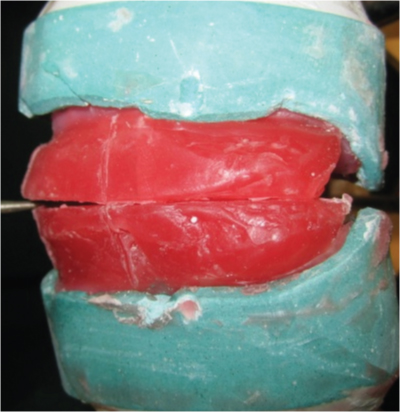
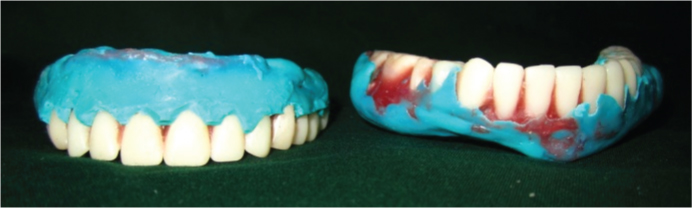
Since it was a severely resorbed ridge, a monoplane occlusion concept was adopted [4]. The records were reassembled and checked for teeth positioning within the neutral zone area [Table/Fig-8]. The trial dentures were checked in the patient’s mouth for aesthetics and occlusion [Table/Fig-9].
Rechecking of the record after teeth setting


External Surface Impression
After taking appropriate patients consent, external impressions were made for the upper and lower dentures along with the impression of the tissue surface (direct relining of both cameo and intaglio surfaces) [5] using Addition silicone impression material (Light body-Aquasil, DENSPLY), [Table/Fig-10,11]. This would help to record the polished surface as well as the tissue surface of the denture at a functional state [Table/Fig-12] [6].
External surface impression

Impression of polished surface of the denture
Functional impression made
Denture Processing
Casts were poured over the impression obtained during the wax try-in and the master cast was fabricated. The cast along with recorded impression was invested into patty of plaster in a denture processing flask (Varisity Flask) and then processed with heat activated polymerising resin (DPI Heat Cure, Dental Products of India, Mumbai, India). The dentures were trimmed, finished, polished [Table/Fig-13,14].
Finished and polished denture


The tissue surface of biometric dentures obtained using functional technique appears to be well formed when compared with conventional dentures. Then the dentures were inserted inside the patients mouth [Table/Fig-15] checked for aesthetics. Final occlusal adjustments were made after 24 hours. Post insertion review was done after twenty four hours and checked for occlusal discrepancies.
Patient with completed denture in biometric denture space

Discussion
In highly atrophic mandible, muscular control over the denture is the main retentive and stabilising factor during function. Management of resorbed ridges had always been a challenge in fabrication of complete dentures [7]. The ultimate objective of prosthodontics is to restore form, function and aesthetics and to fit the denture in biometric denture space to ensure that the muscular forces work effectively in harmony to stabilize the denture. In conventional dentures, teeth were arranged over the crest of the alveolar ridges, which favoured the mechanics of mastication. The function of lips, cheeks and tongue and their controlling action on the dentures during function is a fundamental principle behind biometric denture concept.
Materials like impression plaster advocated by Johnson and modeling plastic by Beresin and Schiesser are messy and cumbersome when compared with materials like Alginate, the material of choice in this case [8]. Other materials most commonly discussed in literature are tissue conditioner (phonetics method) by Joseph E. Makzoume which lacks strength and viscosity to withstand muscle forces and requires incremental addition of materials in layers over the retentive loops [9]. Whereas Alginate being the material used in this case can be added in bulk and are inexpensive.
Alginate is soft material which sets at oral temperature; it can be easily accepted even by very old debilitated patients with poor muscular coordination. Unlike the other materials used alginate lacks strength to withstand muscular forces during moulding. Hence the tray design has been modified with occlusal pillars suggested by Beresin to support the less viscous materials and to maintain the vertical dimension achieved at the preliminary stages.
Research by several authors suggested that use of balanced occlusion concept does not create any detectable advantages for patients, the law of parsimony (to use the simpler of two competing theories) supports monoplane occlusion, zero degree cuspless teeth that reduces lateral forces over the ridge and moreover use of acrylic posterior teeth and its ability to self adjust, improves stability and function of the dentures [10].
Conclusion
The Biometric denture space is the space that exists in each individual, where the denture is designed to function in harmony with the oral musculature neutralizing the forces of the tongue against the lips and cheeks. This space can be functionally recorded with material like alginate which has better flow properties and aid in construction of dentures with better function and aaesthetics.
[1]. Anderson John N, Storer Roy, Immediate and Replacement Dentures 1981 3rd edOxford, LondonBlackwell Publication [Google Scholar]
[2]. Wee AG, Cwynar RB, Cheng AC, Utilization of the neutral zone technique for a maxillofacial patientJournal of Prosthodontics 2000 9(1):2-7. [Google Scholar]
[3]. Beresin V E, Schiesser F J, The Neutral Zone in Complete dentures 1978 2nd edSaint Louis, MissouriThe Mosby company [Google Scholar]
[4]. Jones PM, The monoplane occlusion for complete denturesJ Am Dent Assoc 1972 85(1):94-100. [Google Scholar]
[5]. Neill DJ, Glaysher JKL, Identifying the denture spaceJournal of Oral Rehabilitation 1982 9(3):259-77. [Google Scholar]
[6]. Zenginel M, Buchtaleck J, Rehmann P, Wostmann B, Influence of two functional complete-denture impression techniques on patient satisfaction: dentist-manipulated versus patient-manipulatedInt J Prosthodont 2011 24(6):540-43. [Google Scholar]
[7]. Gahan MJ, The neutral zone impression revisitedBritish Dental Journal 2005 198(5):269-72. [Google Scholar]
[8]. Cagna DR, Massad JJ, Schiesser FJ, The neutral zone revisited: From historical concepts to modern applicationJ Pros Dent 2009 101:405-12. [Google Scholar]
[9]. Makzoume JE, Morphologic comparison of two neutral zone impression techniques: A pilot studyJ Pros. Dent 2004 92:563-68. [Google Scholar]
[10]. Fahmi FM, The position of the neutral zone in relation to the alveolar ridgeJournal of Prosthetic Dentistry 1992 67:805-09. [Google Scholar]