Fatal Case of Pericardial Effusion Due to Myroides Odoratus: A Rare Case Report
Shashank Prateek1, Priyanka Gupta2, Garima Mittal3, Amit K. Singh4
1 Consultant Microbiologist, Department of Microbiology, Metro Heart and Multispeciality Institute, Haridwar, Uttarakhand, India.
2 Senior Resident, Department of Microbiology, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India.
3 Associate Professor, Department of Microbiology, Himalayan Institute of Medical Sciences, Dehradun, Uttarakhand, India.
4 Assistant Professor, Department of Microbiology, Mayo Institute of Medical Sciences, Lucknow, Utter Pardesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shashank Prateek, Consultant Microbiologist, Department of Microbiology, Metro Heart and Multispeciality Institute, Sidcul, Haridwar, Uttarakhand- 249403, India. E-mail : shashankprateek@gmail.com
Myroides spp., previously known as Flavobacterium odoratum, are rare clinical isolates and are often considered non-pathogenic. Natural habitat includes soil, fresh and marine waters, in foods and in sewage treatment plants. We present an unusual case of fatal pericardial effusion due to Myroides odoratus in a patient suffering from chronic kidney disease and undergoing maintenance haemodialysis. This case is presented to show the increasing incidence of rare isolates causing localized and systemic infections and due to their high intrinsic resistance to many antibiotics they can be fatal. Thus isolation of these pathogens is of great clinical importance.
Flavobacterium odoratum, Immunocompromised, Myroides spp., Resistance, Systemic infection
Case Report
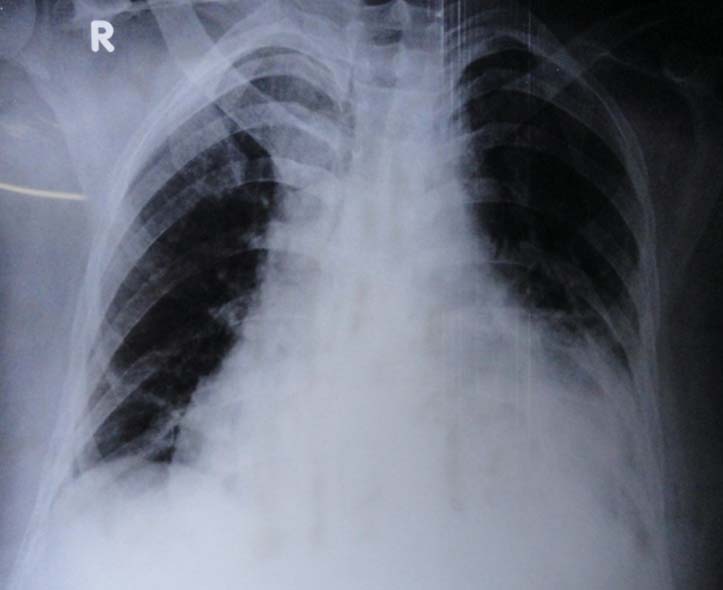
A 69-year-old male, known case of chronic kidney disease, presented with dyspnoea and chest pain associated with few episodes of high grade fever. On general examination patient was conscious and oriented. He also had pallor and pedal oedema. BP was 100/70 mmHg and pulse rate was 90/min. No significant findings were noted on systemic examination. On investigation, haemoglobin was 9.5gm% and TLC was 16700/cumm, Serum creatinine and albumin were 5.3mg/dl and 3.0 g/dl respectively. X-Ray showed diffuse cardiomegaly, with no signs of consolidation [Table/Fig-1] and on echocardiography, Left ventricular dilatation with normal LV contractibility, along with diffuse pericardial effusion was recorded. Pleuropericardial window was created and drain was put in pericardial space to drain out effusion. Pericardial fluid was then sent for ADA levels, cytological and microbiological examination. ADA level was found to be normal (22.0 U/l) and TLC was 120 cells/cubic mm (mostly polymorphs). FNAC of pericardium showed fibrocollageneous tissue with flattened pericardial lining. No granulomatous pathology was seen.
Chest X-ray showing diffuse cardiomegaly with no signs of consolidation
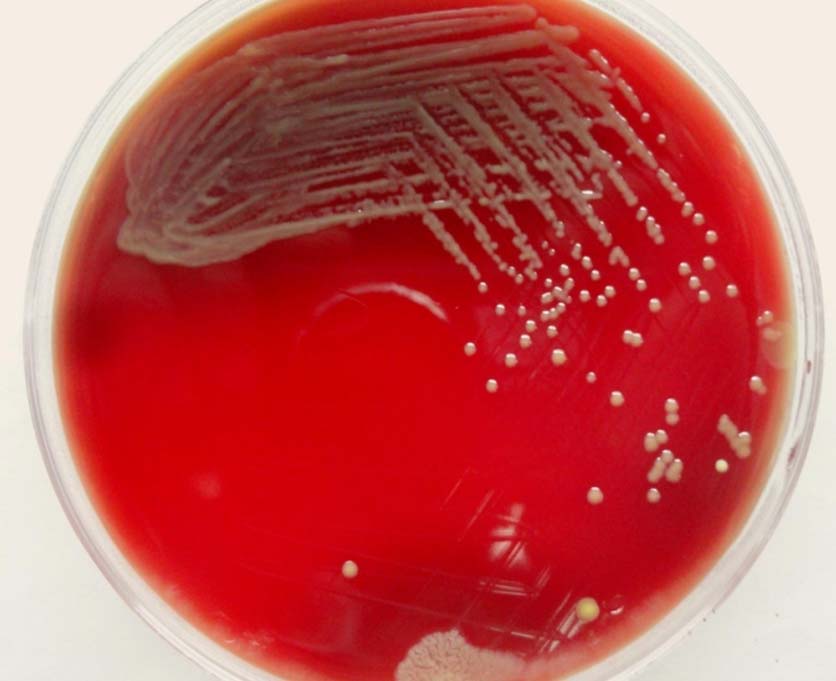
On microbiological investigation, Gram stain showed few inflammatory cells and Gram negative bacilli which on bacterial culture showed nonhaemolytic, pale yellow coloured colonies on blood agar [Table/Fig-2] and Non lactose fermenting colonies on MacConkey agar. Fungal culture of fluid was sterile after 2 weeks. In view of suspicion of Non-fermenter organism, BD Phoenix Identification panel was put up which identified the organism to be Myroides odoratus. Blood culture and urine culture were sterile after 5 days and 48 hours respectively. Antibiotic susceptibility of the isolate was determined by broth microdilution (BD Phoenix automated identification system) and the isolate was found to be pan resistant to all the antibiotics [Table/Fig-3]. Depending upon the microbiological culture and AST report, the patient was started on antibiotics Imipenem and Colistin after clinician’s discretion. Initially patient responded but gradually he developed high grade fever, cough and expectoration by 12th day of admission and there was gradual rise in TLC. On 15th day the pericardial fluid collection was sent for bacterial culture and sensitivity testing which again yielded Myroides odoratus from the sample with similar sensitivity pattern as before. Patient finally succumbed to death due to cardiac arrest.
Blood agar plate showing non-haemolytic pale yellow pigmented colonies suggestive of Myroides spp
Invitro susceptibility of the Myroides odoratus isolate
| Antibiotics | MIC value (ug/ml) | Interpretation (S, I, R) |
|---|
| Amikacin | >32 | R |
| Gentamicin | >8 | R |
| Imipenem | >8 | R |
| Meropenem | >8 | R |
| Ceftazidime | >16 | R |
| Cefepime | >16 | R |
| Cefoperazone-Sulbactam | >16 | R |
| Aztreonam | >16 | R |
| Ampicillin | >16 | R |
| Amoxicillin-clavulanate | >16/8 | R |
| Piperacillin-tazobactam | >64/4 | R |
| Colistin | >2 | R |
| Trimethoprim- sulfamethoxazole | >2/38 | R |
| Ciprofloxacin | >2 | R |
| Levofloxacin | >4 | R |
(MIC, minimum inhibitory concentration; S, susceptible; I, intermediate; R, resistant)
Discussion
Myroides odoratus was first isolated by Stutzer et al., [1]. The genus Myroides comprises of two species Myroides odoratus and Myroides odoratimimus. It belongs to Family Flavobacteriaceae, the species of this genus were formerly classified as Flavobacterium odoratum and later re-classified based on genotypic, phenotypic data [1,2]. This is an aerobic, non- fermentative Gram-Negative bacilli, nonmotile, nonsaccharolytic, oxidase, catalase, urease, and gelatinase positive. They reduce nitrate and do not produce indole. Myroides species grow on most media, including MacConkey agar and colonies are yellow on blood agar and produce a fruity odour [3]. Myroides spp. rarely causes clinical infections and so is generally not considered pathogenic. They are not part of normal human microflora and behave as low grade pathogens, and can cause infections not only in immunocompromised but also in immunocompetent host. Deepa R et al., reported isolation of Myroides odoratus from sputum of an immunocompromised patient leading to pulmonary infection [4]. Another case of Myroides odoratimimus cellulitis following a pig bite in an immunocompetent child was reported by Sofia Maraki et al., [5]. Similarly, Benedetti P et al., also reported a case of soft tissue infection, septic shock and pneumonia due to M. odoratimimus in an immunocompetent male [2]. Few cases of central venous catheter blood stream infections, soft tissue infections, endocarditis and ventriculitis have also been reported due to Myroides spp. [5–8]. Ktari et al., reported a nosocomial outbreak of urinary tract infection caused by Myroides odoratimimus in the urology unit of a Tunisian hospital [9]. The present case is the first case reporting pericardial effusion caused by Myroides odoratus. Myroides spp. mainly affects immunocompromised patients such as those with diabetes, chronic obstructive pulmonary disease and patients on long term steroids. In this case, patient was on long term maintenance haemodialysis which could have been a risk factor for acquiring this rare pathogen. Till date, only two cases have been described in immunocompetent hosts [2,5].
Identification and antibiotic susceptibility testing plays a significant role due to its multi-drug resistant nature. The present isolate showed resistance to all the antibiotics in the panel. Similarly Holmes et al., also reported these strains to be resistant to wide range of antibiotics such as β-lactams, monobactams, carbapenems and aminoglycosides [10]. Mammeri et al., has reported resistance to β-lactams mainly due to the production of chromosomally encoded metallo- β-lactamases (TUS-1 and MUS-1) [11]. Cases have been reported where clinical isolates of Myroides had been found to be susceptible to quinolones and trimethoprim-sulfamethoxazole and clinical cure was attained [6,7] but in our case, the isolate was pan resistant to all the antibiotics.
Conclusion
Infections due to Myroides spp. are being increasingly reported in both immunocompromised and immunocompetent hosts. To the best of our knowledge, this case is first of its kind to be reported from India. This case highlights the fact that a rare pathogen like Myroides spp. should be considered in differential diagnosis of septicaemia and other systemic infections, and clinicians must be aware of its pathogenic role.
(MIC, minimum inhibitory concentration; S, susceptible; I, intermediate; R, resistant)
[1]. Vancanneyt M, Segers P, Torck U, Hoste B, Bernardet JF, Vandamme P, Reclassification of Flavobacterium odoratum (Stutzer 1929) strains to a new genus, myroides, as myroides odoratus comb. nov. and myroides odoratitimus sp. novInter J of Syst bacterial 1996 46(4):926-32. [Google Scholar]
[2]. Benedetti P, Rassu M, Pavan G, Sefton A, Pellizzer G, Septic shock, pneumonia, and soft tissue infection due to Myroides odoratimimus: report of a case and review of Myroides infectionsInfection 2011 39:161-65. [Google Scholar]
[3]. Winn WC Jr, Koneman EW, Allen SD, Procop GW, Janda WM, Schreckenberger PC, The Non-fermentative Gram- negative BacilliKoneman’s Colour Atlas and Textbook of Diagnostic Microbiology. Ch 7 2006 6th edPhiladelphiaLipincott Williams and Wilkins:304-91.In: [Google Scholar]
[4]. Deepa R, Venkatesh KG, Parveen JD, Banu ST, Jayalakshmi G, Myroides odoratus and Chryseobacterium indologenes: Two rare isolates in the immunocompromisedIndian J Med Microbiol 2014 32:327-30. [Google Scholar]
[5]. Maraki S, Sarchianaki E, Barbagadakis S, Myroides odoratimimus soft tissue infection in an immunocompetent child following a pig bite: case report and literature reviewThe Braz J Infect Dis 2012 16(4):390-92. [Google Scholar]
[6]. Ferrer C, Jakob E, Pastorino G, Juncos LI, Right-sided bacterial endocarditis due to Flavobacteriun odoratum in a patient on chronic haemodialysisAm J Nephrol 1995 15:82-84. [Google Scholar]
[7]. MacFarlane DE, Baum-Thureen P, Crandon I, Flavobacteriun odoratum ventriculitis treated with intraventricular cefotaximeJ Infect 1985 11:233-38. [Google Scholar]
[8]. Motwai B, Krezolek D, Symeonides S, Khayr W, Myroides odoratum cellulitis and bacteraemia: a case reportInfect Dis Clin Pract 2004 12:343-44. [Google Scholar]
[9]. Ktari S, Mnif B, Koubaa M, Mahjoubi F, Ben Jemaa M, Mhiri MN, Nosocomial outbreak of Myroides odoratimimus urinary tract infection in a Tunisian hospitalJ Hosp Infect 2012 80(1):77-81. [Google Scholar]
[10]. Holmes B, Snell JJ, Lapage SP, Flavobacterium odoratum: a species resistant to a wide range of antimicrobial agentsJ Clin Pathol 1979 32:73-77. [Google Scholar]
[11]. Mammeri H, Bellais S, Nordmann P, Chromosome-encoded metallo-β-lactamases TUS-1 and MUS-1 from Myroides odoratus and Myroides odoratimimus (formerly Flavobacterium odoratus), new members of the lineage of molecular subclass B1 metalloenzymesAntimicrob Agents Chaemother 2002 46:3561-67. [Google Scholar]