Pharmacoeconomics is analytical tool to know cost of hospitalization and its effect on health care system and society [1]. Cost of hospitalization includes direct medical cost, indirect cost and intangible cost. Cost of hospital bed charge, laboratory charge, diagnostic charge, doctor consulting charge, etc. were included in direct medical cost [1].
In India, apart from the government health services, private sector also play big role to provide health care services. Government of India reported that the private sector delivers about 60% of all inpatient care [2]. In India, during hospitalization 80% patients have to pay out of their pocket for health care service due to lack of insurance cover and more than 40% admitted patient had to borrow money or sell their assets [3].
Information about cost of hospitalization is helpful for policy makers to allocate better health facilities and services [4]. It is also helpful in developing country for reimbursement of social security system [5].
There is lack of data about direct medical cost of hospitalization in admitted patients at private hospital in Western India. Hence we carried out this study to analyze direct medical cost of hospitalization and cost of drug therapy in admitted patients at private hospital in a metro city of Western India.
Materials and Methods
The study was retrospective syudy conducted at one private hospital in metro city of Western India. A study approval was taken from medical director of hospital after assurance to maintain confidentiality of patients and hospital. To know direct medical cost, investigator collected data of 400 admitted patients’ billing record for a period of 01/01/2013 to 31/12/2014. Data was selected randomly from patient registration number. Data like age, gender, admission in medical or surgical ward, outcome of patient, cost of hospitalization including investigation charge, doctor consulting charge, ICU charge etc. were recorded in preformed case record form. Direct medical cost, total cost of drug therapy and cost of group of drugs were calculated. Charges of hospitalization was converted from Indian to United States currency (₹62.19 INR = 1$ USD) exchange rate as per on date on 02/04/2015 available from official Reserve Bank of India’s website. The data were analysed at the end of study by Z, x2 and unpaired t-test.
Results
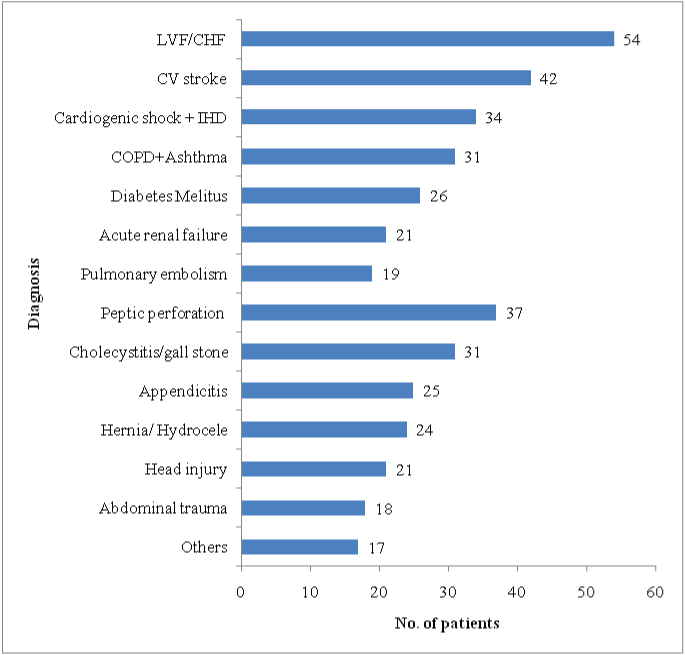
Total 400 patients’ billing record were collected and studied. Patients were divided into medical and surgical patients according to their admission into medical or surgical ward respectively. Patients’ age above 45 years significantly (p<0.05) higher as compared to less than 45 years. Male patients were significantly (p<0.05) higher as compared to female patients. Mortality and average duration of stay, ICU admission, patients on ventilator support were significantly (p<0.05) higher in medical patients as compared to surgical patients [Table/Fig-1]. Out of 400 patients it was observed that 98 (60.12%) patients admitted for surgical procedures (for appendicitis, gall stone, peptic perforation etc), 88(37.13%) patients admitted for cardiovascular disorder (CHF, LVF, IHD) and 63 (26.58%) patients admitted for Central Nervous System (CNS) disorder, CV stroke [Table/Fig-2].
Analysis of demographic data of patients (n=400)
| Demographic data | Medical Patientsn=237 (%) | Surgical Patientsn=163 (%) | Total Patientsn=400 (%) |
|---|
| Age> 45 years | 174(73.41)# | 99 (60.73)# | 273(68.25)# |
| Age ≤ 45 years | 63(26.59) | 64(39.27) | 127(31.75) |
| Male | 127(53.58)@ | 108(66.25)@ | 235(58.75)@ |
| Female | 110(46.42) | 55(33.75) | 165(41.25) |
| Mortality | 84(35.44)* | 41(25.77) | 123(30.75)* |
| Patients on ventilator | 92(38.81)* | 38(23.31) | 130(32.5)* |
| ICU admission | 124(52.32)* | 68(41.17) | 192(48)* |
| Duration of stay in hospital (days) | 8.37±2.16** | 6.41±2.23 | 7.57±2.03** |
| Procedure (surgical/diagnostic) | 46(19.4) | 98(60.12)& | 144(36)& |
*p <0.05 (z-test) significantly higher as compared to surgical patients
**p <0.05 (t-test) significantly higher as compared to surgical patients
&p<0.05 (z-test) significantly higher as compared to medical patients
#p <0.05 (X2 test) significantly higher as compared to age ≤ 45 years
@p <0.05 (X2 test) significantly higher as compared to female
Analysis of diagnosis of patients (n=400)
(CHF=Congestive Heart Failure, LVF- Left Ventricular Failure, IHD- Ischemic Heart Disease COPD- Chronic Obstructive Pulmonary Disease)
Analysis of direct medical cost of hospitalization
Ward bed charge, ICU bed charge and ventilator charge per patient were significantly (p<0.05) higher in medical patients as compared to surgical patients while Operation Theatre (OT) charge and procedural charge were significantly (p<0.05) higher in surgical patients as compared to medical patients. Consultation charge per patient and total cost of drug therapy were significantly (p<0.05) higher in medical patients as compared to surgical patients. Direct medical cost of hospitalization was significantly (p<0.05) higher in medical patients as compared to surgical patients [Table/Fig-3].
Analysis of direct medical cost of hospitalization per patient (n=400)
| Group | Medical Patients(n=237) Mean±SD | % oftotalcost | Surgical Patients(n=163) Mean±SD | % oftotalcost | Total Patients(n=400) Mean±SD | % oftotalcost |
|---|
| Cost inIndianRupee | Cost inUS dollar | Cost inIndianRupee | Cost inUS dollar | Cost inIndianRupee | Cost inUS dollar |
|---|
| Ward bed cost | ₹7534±1250*# | $121±20 | 11.82 | ₹5769±1756 | $92±28 | 10.42 | ₹6815±1465* | $109±23 | 11.29 |
| ICU bed cost | ₹18291±11234*# | $294±180 | 28.67 | ₹7513±3540 | $120±56 | 19.88 | ₹15325±9825* | $246±158 | 25.38 |
| Ventilator cost | ₹8278±4324*# | $133±69 | 12.98 | ₹3791±2236 | $60±35 | 6.85 | ₹6450±3762* | $103±60 | 10.68 |
| OT cost(per hour) | ₹359±124 | $5±2 | 0.56 | ₹3776±2631** | $60±42 | 6.82 | ₹1710±1246** | $27±20 | 2.90 |
| Consultation cost | ₹4123±2764*# | $66±44 | 6.46 | ₹3182±2486 | $51±39 | 5.74 | ₹3707±2216* | $59±39 | 6.2 |
| Lab Investigation cost | ₹1208±984 | $19±15 | 1.89 | ₹1193±1046 | $19±16 | 2.15 | ₹1202±892 | $19±14 | 1.99 |
| Radiology cost | ₹1434±892 | $23±14 | 2.25 | ₹1265±972 | $20±15 | 2.29 | ₹1328±1026 | $21±16 | 2.26 |
| Procedural cost | ₹3006±2182 | $48±38 | 4.71 | ₹9500±6408**# | $152±103 | 17.15 | ₹5652±3876** | $90±62 | 9.37 |
| Drug cost | ₹16206±3286*# | $ 260±52 | 25.41 | ₹13326±2486 | $214±39 | 24.06 | ₹15032±2402* | $241±38 | 24.90 |
| Others (food, nursing care etc) | ₹3348±1258*# | $53±20 | 5.25 | ₹2564±1682 | $41±27 | 4.63 | ₹3029±1928* | $48±31 | 5.01 |
| Total direct medical cost | ₹63789±14692*# | $1025±236 | 100 | ₹55383±16838 | $890±270 | 100 | ₹60363±15824* | $970±254 | 100 |
(Cost expressed in ₹Indian Rupee converted in $ US dollar)
* p <0.05 (t-test) significantly higher as compared to surgical patients
** p <0.05 (t-test) significantly higher as compared to medical patients
# p <0.05 (t-test) significantly higher as compared to total patients
Cost of drug therapy
The cost of drug therapy per patient was calculated. Cost of drug therapy per patient in above 45 years age was significantly (p<0.05) higher as compared to below 45 years age. It was observed that cost of drug therapy per patient in survived cases and patients on ventilator support were significantly (p<0.05) higher as compared expired cases and patients without ventilator support [Table/Fig-4]. Cost of fibrinolytics, anticoagulants, inotropes, antiepilepics/sedatives, cardiovascular drugs, respiratory drugs, diuretics, antidiabetic drugs, anticholinergic drugs were significantly (p<0.05) higher in medical patients as compared to surgical patients. Cost of antimicrobials, IV fluids/Plasma expander, PPIs, antiemetics, analgesics, were significantly (p<0.05) higher in surgical patients as compared to medical patients [Table/Fig-5].
Analysis of cost of drug therapy according to ventilator support and outcome basis (n=400)
| Group | Medical Patients(n=237)Mean±SD | Surgical Patients(n=163)Mean±SD | Total Patients(n=400) Mean±SD |
|---|
| Cost of therapy per patient age >45 | ₹11831±2876*# $190±46 | ₹8872± 2098 $142±33 | ₹10625±2258* $170±36 |
| Cost of therapy per patient in age ≤45 | ₹4375± 1785 $70±28 | ₹4454± 2102 $71±33 | ₹4407±2056 $70±33 |
| Cost of therapy per patient in survived cases | ₹10354±2042*# $166±32 | ₹9231± 1587 $148±25 | ₹9856±2174* $159±34 |
| Cost of therapy per patient in expired cases | ₹5852± 2346*# $94±37 | ₹4095± 2537 $65±40 | ₹5136±2203* $82±35 |
| Cost of therapy per patient on ventilator | ₹10482±2874*# $168±46 | ₹8364± 2162 $137±35 | ₹9619±2332* $154±35 |
| Cost of therapy per patient on without ventilator | ₹5724± 2034* $92±32 | ₹4762± 2130 $76±34 | ₹5413±2146* $87±34 |
(Cost expressed in ₹Indian Rupee converted in $ US dollar)
* p <0.05 (t-test) significantly higher as compared to surgical patients
** p <0.05 (t-test) significantly higher as compared to medical patients
# p <0.05 (t-test) significantly higher as compared to total patients
Analysis of cost of drug therapy among various drug groups (n=400)
| Group | Medical Patients(n=237) Mean±SD | % oftotalcost | Surgical Patients(n=163) Mean±SD | % oftotalcost | Total Patients(n=400) Mean±SD | % oftotalcost |
|---|
| Cost inIndianRupee | Cost inUS dollar | Cost inIndianRupee | Cost inUS dollar | Cost inIndianRupee | Cost inUS dollar |
|---|
| Antimicrobials | ₹4672±2462 | $75±39 | 28.83 | ₹5356±3478** | $86±55 | 40.19 | ₹4951±2826 | $79±45 | 32.94 |
| Fibrinolytics | ₹2862±1478*# | $46±23 | 17.66 | ₹824±568 | $13±9 | 6.18 | ₹2032±1674* | $32±26 | 13.52 |
| Anticoagulant | ₹1236±984* | $19±15 | 7.63 | ₹926±742 | $14±11 | 6.94 | ₹1109±918* | $17±14 | 7.38 |
| Antiepileptic/ Sedatives | ₹1204±714*# | $19±11 | 7.43 | ₹654±498 | $10±8 | 4.91 | ₹980±746* | $15±11 | 6.52 |
| IV fluids/ Plasma expander | ₹837±563 | $13±9 | 5.16 | ₹934±762** | $15±12 | 7.01 | ₹877±643 | $14±10 | 5.83 |
| Inotropes | ₹1033±846*# | $16±13 | 6.37 | ₹648±464 | $10±7 | 4.86 | ₹875±710* | $14±11 | 5.82 |
| Analgesics | ₹735±459 | $11±7 | 4.54 | ₹1024±832**# | $16±13 | 7.69 | ₹853±584** | $13±9 | 5.67 |
| Proton Pump Inhibitors | ₹578±320 | $9±5 | 3.56 | ₹964±712**# | $15±11 | 7.24 | ₹735±512** | $11±8 | 4.89 |
| Cardiovascular drugs | ₹834±692*# | $13±11 | 5.15 | ₹234±142 | $3±2 | 1.76 | ₹589±394* | $9±6 | 3.92 |
| Antiemetics | ₹422±318 | $6±5 | 2.61 | ₹682±514**# | $10±8 | 5.12 | ₹528±402** | $8±6 | 3.51 |
| Respiratory drugs | ₹624±486*# | $10±7 | 3.85 | ₹312±172 | $5±2 | 2.34 | ₹497±264* | $7±6 | 3.3 |
| Antidiabetic drugs | ₹428±316*# | $6±5 | 2.64 | ₹124±98 | $1±1 | 0.93 | ₹304±172* | $4±2 | 2.02 |
| Diuretics | ₹324±164*# | $5±2 | 1.99 | ₹104±82 | $1±1 | 0.78 | ₹234±174* | $3±2 | 1.56 |
| Anticholinergics | ₹215±135*# | $3±2 | 1.33 | ₹128±76 | $2±1 | 0.96 | ₹180±114* | $2±1 | 1.2 |
| Others | ₹202±108 | $3±1 | 1.25 | ₹412±214**# | $6±3 | 3.09 | ₹288±168** | $4±2 | 1.92 |
(Cost expressed in ₹Indian Rupee converted in $ US dollar)
* p <0.05 (t-test) significantly higher as compared to surgical patients
** p <0.05 (t-test) significantly higher as compared to medical patients
# p <0.05 (t-test) significantly higher as compared to total patients
Discussion
In our study more than 60% patients were above 45 years age group. It may be due to life threatening diseases like cardiovascular diseases, respiratory infection, diabetes and traumatic injury which are common in above 45 years age group which may required hospitalization. In our study male patients were significantly higher as compared to female patients. Roy et al., reported that due to social status and economic dependence women did not get better health care facilities as compared to male [6]. Similar report of gender disparity in use of health care service also observed in China and Nigeria [7,8]. It is concern for our society and government to look after and provide health care service to women. Mortality was significantly higher in medical patients (34%) as compared to surgical patients (25%). Patients on ventilator were significantly higher in medical patients (38%) as compared to surgical patients (23%). Mukhopadhyay et al., reported that mortality was higher in patient on ventilator due to critically illness as well as cardio respiratory complication [9]. Average duration of stay was significantly (p<0.05) higher in medical patients as compared to surgical patients. In medical patients co-morbid condition was highly observed while surgical patients were admitted for postoperatively observation.
In direct medical cost, ward bed charge, ICU bed charge and ventilator charge per patient were significantly higher in medical patients while in USA it was higher in surgical patients [10]. Dasta et al., reported that cost per patient on ventilator was $31,574±42,570 which was higher as compared to our ventilator cost per patient ($103±60) [11]. Parikh et al., reported that cost per patient per day in ICU was ₹1,973 (U.S. $57) which was lower as compared to our ICU bed cost per patient (₹15325±9825) [12]. It may be due to their study conducted in 1999 while our study was conducted a period of 2013-14. Ward bed charge, ICU bed charge and ventilator charge were accounted 47% of direct medical cost. It suggested that cost of ICU care in direct medical cost was higher and create more financial burden to patients. ICU care cost has major part in direct medical cost during hospitalization as various newer machine and ventilator charge accounted in the ICU care cost.
In surgical patients cost of OT per hour per patient was ₹3776±2631 which was lower to compared to both studies by Singh M et al., and Siddarth V et al., where per hour OT cost was ₹11948 and ₹22626 respectively [13,14]. It may be due to different patient profile and different surgical procedure which required different operation theatre. Chatterjee S et al., reported that unit cost of operative procedure was ₹27,236 in private hospital which was higher as compared to operative cost of surgical patients where it was ₹9500±6408 [15]. It may be due to number of surgical procedure in our study was 96 while it was 2058 in their study. By comparing average cost of procedure among different hospital, it will be helpful for hospital administration to monitor the operation cost for better resource utilization. OT charge and procedural charge accounted 23% of direct medical cost during hospitalization in surgical patients. Our study revealed that OT charge and procedural charge has greater contribution in direct medical cost in surgical patients.
Consultation cost per patient was above ₹3700 in all patients which was higher as compared to Kumpatla et al., where it was ₹1050 [16]. This may be due to different consulting charge of doctor among different hospital in different location of country as well as patient duration of stay in ward or ICU in hospital affect consulting cost. Total cost of investigation of per patient was more than ₹2500 in our study which was lower to ₹25,030 reported by Pattanaik S et al., [17]. It may be due to they include intervention procedure cost while we include only investigation cost.
Direct medical cost of hospitalization was significantly higher in medical patients as compared to surgical patients. It may be due to cost of ICU care was higher in medical patients as compared to surgical patients. Dror et al., reported that cost of hospitalization was ₹1405±151 in private hospital which was lower as compared to our study [18]. It may be due to study location of both studies as our study was at private hospital in metro city while their study was five resource poor locations in India.
Cost of drug therapy per patient was ₹16206±3286 ($260±52) in medical patients which was significantly higher as compared to surgical patients where it was ₹13326±2486 ($214±39). Both were lower as compared to ₹19,725 reported by Biswal et al., [19]. Data from the western literature reported drug costs per patient-day ranging from $208 to $312 which was similar to our study [20]. Cost of drug therapy was 25% of direct medical cost in our study which was lower to 74% reported by Chatterjee et al., [21]. It may be due to different cost methodology used in both studies. Cost of drug therapy in our study was similar to western countries. It will affect utilization of health care service for our people as there is less medical insurance penetration as compared to western countries.
Cost of drug therapy per patient in survived cases was above ₹9000 in our study which was higher ascompared to Patel MK et al., (₹2932.36) [22]. It may be due to survival rate was 21% in their study while it was 70% in our study [22]. Cost of fibrinolytics, anticoagulants and inotropics were significantly higher in medical patients and accounted 31% of cost of drug therapy in medical patients. Patel BJ et al., and Patel MK et al., reported that cost of inotropic agents per patient was ₹262 and ₹408 respectively which was lower compared to our study (₹875±710) [22,23]. Patient of IHD, pulmonary embolism were admitted in medical ward and in these patient inotropes, fibrionolytics and anticoagulant were used.
Cost of PPIs, antiemetics, analgesics were above $10 in surgical patients which was lower to reported by Kaur S et al., where they were above $70 [24]. These three drugs accoutend 20% of cost of drug therapy in surgical patients. Pantoprazole is useful in preventing bleeding and analgesics to reduce and treat postoperative pain while antiemetics were commonly prescribed to prevent nausea and vomiting in postoperative patients.
Cost of antimicrobials per patient was ₹5356±3478 ($86±55) in surgical patients which was significantly higher as compared to medical patients. In surgical patients antimicrobials were prescribed to prevent and treatment of infections. Study conducted at Nepal reported that cost of antimicrobials per patient was $16.5±13.4 which was lower as compared to our study [25]. Daily antimicrobial cost was ₹114 and $89 in Belgium and Turkey respectively [26,27]. Both were higher as compared to our study. In our study cost of antimicrobials was 33% of total drug cost in all patients which was lower to 72.3% reported by Williams P et al., [28]. Antimicrobial cost accounted more in total cost of drug therapy due to its inappropriate and irrational use during hospitalization. So, specific guideline should be made for rational, affordable use of antimicrobials during hospitalization.
In our study ward bed charge, ICU bed charge, ventilator charge accounted one third of direct medical cost of hospitalization and cost of drug therapy accounted one fourth of cost of direct medical cost in all the patients. Antimicrobials accounted 33% of total drug cost in total patients. Our study will be helpful for hospital administration to monitor and maintain affordable health care service to patients and quality health service with least possible cost. It will also help to educated prescribers about use of cheap and affordable drugs and antimicrobials. It will also help government and hospital administration to give economic benefits to poor people by evaluation of direct medical cost of hospitalization.
Limitation
Our study limitation, we did not calculate indirect cost like transport cost, loss of wages, medical equipment cost, staff salary cost. Further we did not include tertiary teaching care hospital, charitable trust hospital and other corporate hospital. Our study is a preliminary study on hospital costing in private hospital in Western India. In account of the size and diversity of our country and charge variations across hospitals further large size study should be undertaken to know better understanding of hospital costing. It provides more comprehensive information to hospital administration and policy makers for policy purposes.
Conclusion
In conclusion, our study reveals that ward bed charge, ICU bed charge, ventilator charge has more contribution in direct medical cost of hospitalization. Cost of drug therapy accounted one fourth of direct medical cost of hospitalization. Cost of antimicrobials accounted 33% of cost of drug therapy. This study will helpful for hospital administration to monitor their hospital charges to affordable for patients and education to prescribers for affordable prescription of antimicrobials and better management of patients.
*p <0.05 (z-test) significantly higher as compared to surgical patients
**p <0.05 (t-test) significantly higher as compared to surgical patients
&p<0.05 (z-test) significantly higher as compared to medical patients
#p <0.05 (X2 test) significantly higher as compared to age ≤ 45 years
@p <0.05 (X2 test) significantly higher as compared to female