EMPADE Study: Evaluation of Medical Prescriptions and Adverse Drug Events in COPD Patients Admitted to Intensive Care Unit
Mir S. Adil1, M. Amer Khan2, M. Nematullah Khan3, Ihtisham Sultan4, M. Aamer Khan5, S. Amir Ali6, Afroze Farooqui7
1 Deccan School of Pharmacy, Clinical Pharmacist, Apollo Hospital, Jubilee Hills, Hyderabad, India.
2 Student, Deccan School of Pharmacy, Hyderabad, India.
3 Student, Deccan School of Pharmacy, Hyderabad, India.
4 Student, Deccan School of Pharmacy, Hyderabad, India.
5 Student, Deccan School of Pharmacy, Hyderabad, India.
6 Head of Department, Department of Pharmacy Practice, Owaisi Hospital & Research Centre, Hyderabad, India.
7 Student, Deccan School of Pharmacy, Hyderabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mir S Adil, New Malakpet, Hyderabad-24, India.
E-mail: iampharmd@rediff.com
Introduction
Inappropriate drug usage may preclude ideal benefit due to increased medical cost, antimicrobial resistance, adverse effects and mortality. Therefore drug utilization studies have become a plausible means in evaluating the healthcare systems. COPD management usually involves more than one drug which may escalate the risk of ADEs (adverse drug events).
Aim
The present study was aimed at assessing the current drug practice and ADEs in COPD management in ICU.
Materials and Methods
A total of 1,044 patients admitted for the treatment of COPD were included in the study. Their prescriptions were recorded for evaluation of drug utilization and patients were counseled for assessing ADEs. Results were evaluated by Chi-square test and percentages.
Result
All-embracing 15,360 drugs were prescribed at an average of 14.71 drugs per patient, wherein β2-agonists were extensively prescribed agents followed by inhaled-corticosteroids and anti-cholinergics. 372 ADEs were reported in 252 patients, wherein restlessness was the most frequent ADE and theophylline was found to be associated with highest cases of ADEs.
Conclusion
Practitioners should prescribe least number of drugs to mitigate the likelihood of adverse outcomes in patients due to numerous drugs usage, which may be achieved by following GOLD guidelines. The present work may help in improving the current management of COPD by rectifying the flaws delineated in this article.
Chronic obstructive pulmonary disease, Physician’s practice patterns, Respiratory medicine, Undesirable effects
Introduction
Drug utilization studies, one of the most essential aspects of Pharmacoepidemiology, is defined as the marketing, distribution, prescription and use of drugs in a society, with distinct prominence to the resulting medical, social and economic outcomes [1,2]. Drug utilization audits ensure safe and correct usage of drugs, which can either be quantitative or qualitative or a combination of both [3]. Inappropriate usage of drugs may act as barrier in achieving ideal benefit as it may lead to sub-therapeutic effect, antimicrobial resistance, excess medical cost, adverse effects or mortality. Hence, drug utilization studies have become a plausible means in evaluating the health systems [1]. Chronic Obstructive Pulmonary Disease (COPD), the fourth leading cause of death worldwide, is a common evitable, manageable and progressive disease characterized by sedulous airflow restriction [4]. Pharmacotherapy in COPD usually involves usage of numerous drugs, thereby increasing the risk of adverse drug events (ADEs) proportionally. Predominantly, no drug is absolutely innocuous and an ADE can eventuate when it is administered singly or in concoction. An ADE is “A response to a drug which is detrimental, unintended and which eventuate at doses commonly used in man for the prophylaxis, diagnosis or therapy for an illness” [5]. Most physicians fail to discern bacterial infections from viral infections and eventually end up prescribing antibiotics in viral infections [6]. Antibiotics serve the most frequent cause of ADEs in hospitalized patients, while bronchodilators are associated with approximately 20% of all ADEs in COPD, mostly fatal in severity [7]. Corticosteroids are also responsible for a number of potential ADEs [8].
The prediction of a drug to develop an adverse event is assessed by clinical prudence [9]. Of late, there are various methods for assessing the causality, which include WHO probability scale, Naranjo’s scale, Karch & Lasagna scale, European ABO system, to name a few [10]. Naranjo’s scale is the easiest and most commonly preferred; involving a set of questionnaires, each attributed a certain score. Based on the total score, the drug-ADE association is termed definite, probable, possible or doubtful [5,11].
Many studies have been conducted in the past on respiratory diseases, however to our knowledge published data particularly focused on COPD especially in India is limited. It was indeed necessary to assess the approach of Indian pulmonologists in treating COPD patients in order to refine the treatment practice. The present study aimed at assessing the current drug practice and ADEs in COPD management in ICU.
Materials and Methods
Patients and Methods: EMPADE study was single-centered, prospective, observational, cross-sectional, conducted at Respiratory Intensive Care Unit after acquiring an approval from the Medical Superintendent (Approval no: DCMS/PEH/740/2013), while ethics committee waiver was taken from the hospital’s ethics committee. A total of 1,044 prescriptions were analysed from October 2012 to April 2014. Individual patients who cooperated were interviewed and relevant information was recorded in case report form (CRF), which was designed in a manner to collect data related to medication utilization, ADEs, patient’s habits and family history. Verbal consent was taken from each patient before their enrollment. The patient population was divided into adults with 18-59 years and geriatrics who were 60 years of age or above.
Inclusion/ Exclusion Criteria
Patients elder than 18 years of both genders suffering from COPD and willing to give consent were included, whereas pregnant women and pediatric patients were excluded from the study.
Statistical Analysis
Data comprising patient demographics, co-morbidities, medications prescribed and daily progress of patient were collected from treatment charts/case sheets, laboratory reports and verbal information from patients during interviews. Data was compiled by classifying it in independent variables, evaluated by Chi-square test and calculated in percentages.
Results
Analysis of 1,044 patients revealed that COPD was more prevalent in males (59.8%) than in females (40.2%) with a male to female ratio of 1.49 and mean age of 61.29 years. Demographic characteristics revealed that patients above 60 years were suffering more (58.6%) from COPD than adults (41.4%). Of all the patients, about 34.9% were current smokers, besides 11.9% who were smokers in their past life. Most of the patients (44.8%) in EMPADE study were prescribed 11-15 drugs in their prescriptions, while 17.6% and 37.5% were prescribed ≤10 and ≥16 drugs in their prescriptions, respectively. Despite the best efforts of the medical team, 12 patients unfortunately breathed their last during the course of study [Table/Fig-1]. Patients were found to be suffering from different co-morbidities as seen in [Table/Fig-2].
| Demographics | Patients |
|---|
| Adult (18-59 years)MaleFemaleGeriatric (≥60 years)MaleFemaleRangeMean AgeStandard DeviationMaleFemaleMale/Female ratio | 432 (41.4%)240 (23%)192 (18.4%)612 (58.6%)384 (36.8%)228 (21.8%)65 (25-90)61.2814.2846244201.485 |
| Cigarette smokersNon-smokersEx-smokerCurrent smokers | 556 (53.2%)124 (11.9%)364 (34.9%) |
| No. of patients died during the study | 12 |
| Total no. of patients | 1,044 |
| Total no. of drugs prescribed | 15,360 |
| Drugs prescribed per patient≤1011-15≥16 | 184 (17.6%)468 (44.8%)392 (37.5%) |
Distribution of underlying co-morbidities in patients
| Co-morbid diseases | No. of Patients |
|---|
| Endocrine disorders | 117 |
| Cardiovascular disorders | 184 |
| Neurological disorders | 42 |
| Dermatological disorders | 61 |
| Gastrointestinal disorders | 87 |
| Cardiovascular + Endocrine disorders | 302 |
| Others | 25 |
| None | 226 |
| Total | 1,044 |
A total of 15,360 drugs were prescribed to 1,044 patients at an average of 14.71 drugs. Based on the usage, important drugs in this study were clubbed together in decreasing order from β2-agonists to Leukotriene antagonists as seen in [Table/Fig-3]. These drugs constituted about 61.2% of all drugs utilized in the study while rest was used for minor ailments/co-morbidities.
Drug classes’ proportion in total drugs
| Category | Drug | Drug utilization |
|---|
| Timesprescribed(n=15360) | Patientsreceived(n=1044) |
|---|
| β2-agonists | Salbutamol | 996 | 1836 (11.95) | 1044 (100) |
| Oral Salbutamol | 804 |
| Salmetrol | 36 |
| Antibiotics | Penicillin | 588 | 1396 (9.09) | 588 (56.3) |
| Cephalosporin | 420 |
| Fluoroquinolone | 204 |
| Nitro-imidazole | 96 |
| Macrolide | 76 |
| Aminoglycoside | 12 |
| Inhaled-Corticosteroids | Budesonide | 1024 | 1024 (6.66) | 1024 (98.1) |
| Anti-cholinergics | Ipratropium Bromide | 996 | 1020 (6.64) | 996 (95.4) |
| Scopolamine | 24 |
| Xanthine Derivatives | Theophylline/Etophylline | 912 | 912 (5.93) | 912 (87.4) |
| Mucolytics | Ambroxol | 600 | 840 (5.46) | 840 (80.5) |
| Acetyl cysteine | 192 |
| Bromhexine/Terbutaline/Guaifenesin | 48 |
| Oral-Corticosteroids | Hydrocortisone | 420 | 816 (5.31) | 816 (78.2) |
| Methyl prednisolone | 396 |
| Anti-histamines | Levocetirizine | 720 | 756 (4.92) | 756 (72.4) |
| Chlorpheniramine | 24 |
| Loratidine | 12 |
| Leukotriene antagonist | Montelukast | 696 | 696 (4.53) | 696 (66.6) |
| Total | 9400 (61.19) | - |
Antibiotics were used in 56.32%, penicillins were the most commonly prescribed antibiotics (42.2%) accounting for nearly half of the whole antibiotics, followed by cephalosporins, fluoroquinolones and others. About 95.4% of total COPD patients were given the combination of LABA/SABA+ICS+LAMA/SAMA, whereas mono-therapy of LABA/SABA was used in just 20 patients and dual therapy of LABA/SABA+ICS in 28 patients.
Oral tablet/capsule (39.1%) were the most frequently prescribed dosage form followed by parenterals (35.4%), nebulization (12.4%), syrups (8.9%), inhalers (2.1%) and others (1.4%).
A high proportion of drugs were utilized for treating co-morbidities related to cardiovascular and endocrinological diseases, which are represented in [Table/Fig-4].
Drug used for co-morbid conditions
| Category of drug | Frequency |
|---|
| Anti-diabetic | 405 |
| Cardiovascular agents | Beta blocker | 134 |
| Calcium channel blocker | 153 |
| ARB | 167 |
| ACE | 145 |
| Diuretics | 216 |
| Vasodilator | 56 |
| Cardiac glycosides | 41 |
| Statins | 367 |
| Beta blocker + Calcium channel blocker | 107 |
| Beta blocker + Diuretics | 64 |
| ARB + Diuretics | 59 |
| Anti-platelet | 283 |
| Anti-coagulant | 214 |
Among 1,044 patients involved in the study, 252 patients suffered ADEs, wherein 144 (57.1%) were males and 108 (42.9%) were females. A substantial number of ADEs (71.4%) were found in patients above 60 years of age compared to adults (28.6%) {Chi square (χ2) value of 9.355 (dF=3); p<0.025} as shown in [Table/Fig-5]. A total of 372 ADEs were experienced by 252 patients indicating that some patients may have experienced multiple ADEs. Overall, 164 patients experienced single ADE, 68 patients experienced two ADEs, 12 patients experienced three ADEs and 4 patients each experienced four and five ADEs. Among 252 ADE experienced patients, 24 (9.5%) patients were hospitalized because of an ADE.
| Age Group | Sex | Patients with ADEs | Patients without ADEs | Total Patients |
|---|
| Observed Frequency | Expected Frequency | Observed Frequency | Expected Frequency |
|---|
| Adult (18-59) | Male | 24 | 57.92 | 216 | 182.08 | 240 |
| Female | 48 | 46.36 | 144 | 145.64 | 192 |
| Geriatric (≥60) | Male | 120 | 92.68 | 264 | 291.32 | 384 |
| Female | 60 | 55.04 | 168 | 172.96 | 228 |
| Total | 252 | 792 | 1,044 |
Various organ systems were affected by the ADEs, as depicted in [Table/Fig-6]. Gastrointestinal tract was affected the most accounting 48.38% of all ADEs. The five most frequently observed ADEs were restlessness, abdominal pain, diarrhea, nausea and constipation. ADEs were classified according to Naranjo’s scale as: Definite-52, Probable-232, Possible-88 and Doubtful-0.
Distribution of adverse drug events into different systems
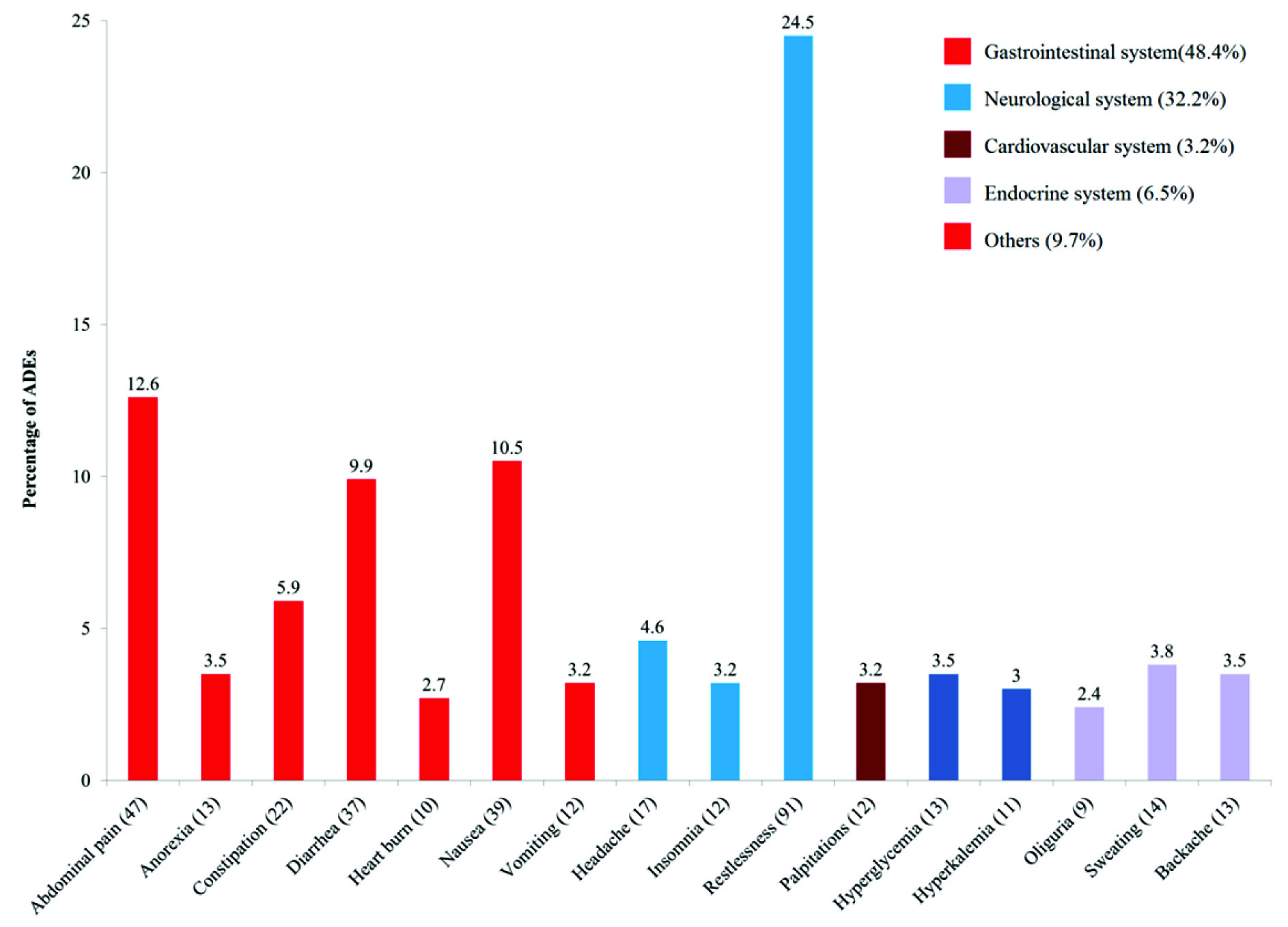
A total of 372 ADEs (2.42%) were observed from 15,360 drugs utilized in the study. Bronchodilators were responsible for 16.1% ADEs and theophylline was most commonly involved in causing ADEs with 168 (45.2%) events. Drug with highest suspected prevalence rate was levofloxacin, however it was administered to a small size of patients (24) as represented in [Table/Fig-7].
Suspected prevalence rate of drugs in causing adverse events
| Drugs | No. of times suspected | No. of times prescribed | Suspected prevalence |
|---|
| Amlodipine | 49 | 192 | 0.25 |
| Azithromycin | 10 | 36 | 0.27 |
| Bisacodyl | 22 | 96 | 0.24 |
| Budesonide | 60 | 996 | 0.06 |
| Cefaperazone | 11 | 360 | 0.04 |
| Chlordiazepoxide | 3 | 12 | 0.25 |
| Chlorpheniramine Maleate | 9 | 24 | 0.38 |
| Diclofenac | 11 | 60 | 0.18 |
| Fluticasone | 5 | 12 | 0.41 |
| Furosemide | 16 | 348 | 0.04 |
| Hydrocortisone | 9 | 460 | 0.02 |
| Iron | 35 | 652 | 0.05 |
| Levofloxacin | 12 | 24 | 0.50 |
| LevoCitirizine | 24 | 720 | 0.03 |
| Methyl Prednisolone | 17 | 396 | 0.04 |
| Metronidazole | 21 | 96 | 0.21 |
| Montelukast | 13 | 696 | 0.17 |
| Ondansetron | 24 | 192 | 0.12 |
| Pantoprazole | 96 | 948 | 0.10 |
| Pcm | 36 | 468 | 0.07 |
| Piperacillin/Tazobactam | 36 | 108 | 0.33 |
| Salbutamol | 77 | 1212 | 0.06 |
| Theophylline | 168 | 912 | 0.18 |
| Thyroxine | 11 | 24 | 0.46 |
| Tramadol | 13 | 144 | 0.09 |
| Ursodiol | 4 | 12 | 0.33 |
Discussion
A high number of average drugs per prescription shows physicians’ tendency to prescribe more drugs to control acute exacerbations of COPD. β2-agonist and corticosteroids were the preferred drugs in the present study, which was similar to observations from other studies [12]. However, extensive usage of mucolytics was a sharp contrast to previous studies [12,13]. Antibiotics usage was slightly higher than that of other studies [13], but the trend of using amoxicillin as a preferred agent was similar to the reviewed literature [14,15]. The study highlights that among all the antibiotics used, the preferred agents were penicillins especially the combination of amoxicillin-clavulanate. This combination is preferred in cases of complicated exacerbations (>4 exacerbations per year and FEV1 35%-50% of predicted). Second and Third generation cephalosporins and macrolides are preferred in uncomplicated exacerbations (<4 exacerbations per year FEV1 >50% of predicted).
It is widely acknowledged that LABA/SABA-ICS combination therapy is far better than LABA/SABA mono-therapy in controlling COPD; this combination not only reduces the risk of exacerbations but also improves QOL and airflow measures [16–19]. Anti-inflammatory activity of the combination may help in reducing the risks of re-hospitalization or death [20]. In the present study most of the patients were treated by the said combination as COPD exacerbations is the chief cause of patients to be admitted in ICU. During exacerbations, intensification of bronchodilator regimens is used commonly. Short acting beta 2 agonists were preferred owing to their rapid onset of action, while anti-cholinergics were added if symptoms persist after increased doses of beta 2 agonist.
Adding theophylline, leukotriene antagonists or antihistamines in routine treatment protocol seem to ameliorate respiratory symptoms [21], improve PFT, dyspnea score and QOL in stable COPD [22], accordingly these agents were utilized wherever necessary. Oral tablets/capsules were preferred dosage form; however, it is highly recommended that physicians prescribe inhalers more than tablets/capsules.
ADEs in patients above 60 years of age were higher than adults specifying that elderly are more prone to drug’s adverse effects. This observation was relatively similar to a previous study with ratio of ADEs in patients above 60 years to adults as 2.5 [7]. The five most frequently observed ADEs in our study were different from a past study [23]. Out of the total drugs, just 2.43% lead to ADEs, which was extremely less compared to a study conducted by N Tyagi et al, wherein the number was 31.5% [5]. Gallelli and Buajordet with their teams found that bronchodilators were responsible for 18.5% and 19.5% of all ADEs [7], whereas theophylline was found to be responsible for maximum ADEs, these reports were similar to our results [7,23].
Conclusion
The ongoing COPD management in Indian Hospitals is not sufficiently rational. Based on the lacunae in the current prescribing practice, there is a necessity to persuade physicians to follow GOLD guidelines while managing COPD patients. Unnecessary usage of antibiotics and high risk drugs such as theophylline led to a number of ADEs in the present study, therefore usage of these drugs should be restricted by physicians, unless patient’s condition demands. These situations not only endanger the quality of patients’ life but also increase the financial burden on patients. Authors of EMPADE study suggest physicians to prescribe least number of drugs considering the risk of drug-drug interactions resulting from multiple drugs usage. The present work may help improve the management of COPD by rectifying the loopholes postulated in this article.
[1]. Sachdeva PD, Patel BG, Drug Utilization Studies Scope and Future PerspectivesInternational Journal on Pharmaceutical and Biological Research 2010 1(1):11-17. [Google Scholar]
[2]. Gama H, Drug Utilization StudiesArquivos De Medicina 2008 22(2/3) [Google Scholar]
[3]. Hunninghake DB, Cardiovascular disease in chronic obstructive pulmonary diseaseProc Am Thorac Soc 2005 2(1):44-49. [Google Scholar]
[4]. Global initiative for chronic obstructive lung disease, 2013. www.goldcopd.org [Google Scholar]
[5]. Tyagi N, Gulati K, Vijayan VK, Ray A, A Study to Monitor Adverse Drug Reactions in Patients of Chronic Obstructive Pulmonary Disease: Focus on TheophyllineIndian J Chest Dis Allied Sci 2008 50:199-202. [Google Scholar]
[6]. Grossman RF, The Value of Antibiotics and the Outcomes of Antibiotic Therapy in Exacerbations of COPDChest 1998 113(4):249S-55S. [Google Scholar]
[7]. Gallelli L, Ferreri G, Colosimo M, Pirritano D, Flocco MA, Pelaia G, Retrospective analysis of adverse drug reactions to bronchodilators observed in two pulmonary divisions of Catanzaro, ItalyPharmacol Res 2003 47(6):493-99. [Google Scholar]
[8]. Mac Intyre NR, Corticosteroid Therapy and Chronic Obstructive Pulmonary DiseaseRespiratory Care 2006 51(3):289-96. [Google Scholar]
[9]. Decramer M, Bartsch P, Pauwels R, Yernault JC, Management of COPD according to guidelines. A national survey among Belgian physiciansMonaldi Arch Chest Dis 2003 59(1):62-80. [Google Scholar]
[10]. Adil MS, Farooqui AF, Ciprofloxacin Induced Systemic Lupus ErythematosusIndo American Journal of Pharm Research 2013 3(9):7485-92. [Google Scholar]
[11]. Moore N, Lecointre D, Noblet C, Mabille M, Frequency and cost of serious adverse drug reactions in a department of general medicineBr J Clin Pharmacol 1998 45(3):301-08. [Google Scholar]
[12]. Miravitlles M, Mayordomo C, Artés M, Sánchez-Agudo L, Nicolau F, Segú JL, Treatment of chronic obstructive pulmonary disease and its exacerbations in general practice. EOLO Group. Estudio Observacional de la Limitación Obstructiva al Flujoa EreoRespir Med 1999 93(3):173-79. [Google Scholar]
[13]. Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM, Antibiotics and steroids for exacerbations of COPD in primary care: compliancewith Dutch guidelinesBr J Gen Pract 2006 56(530):662-65. [Google Scholar]
[14]. Dawadi S, Rao BS, Khan GM, Pattern of antimicrobial prescription and its cost analysis in respiratory tract infection, Kathmandu UniversityJournal of Science, Engineering and Technology 2005 1(1):1-9. [Google Scholar]
[15]. Smith JA, Redman P, Woodhead MA, Antibiotic use in patients admitted with acute exacerbations of chronic obstructive pulmonary diseaseEur Respir J 1999 13(4):835-38. [Google Scholar]
[16]. Johnson M, Interactions between corticosteroids and beta2-agonists in asthmaand chronic obstructive pulmonary diseaseProc Am Thorac Soc 2004 1(3):200-06. [Google Scholar]
[17]. Combination Long-Acting Beta-Agonist Inhaled Corticosteroid: Summary of Clinical Evidence and Drug Utilization Evaluation. Drug Use Research & Management Program [Google Scholar]
[18]. Guidelines for the diagnosis and treatment of Chronic Obstructive Pulomonary DiseaseThe Japanese Respiratory Society2nd edition:1-36. [Google Scholar]
[19]. Cazzola M, Matera MG, The effective treatment of COPD: Anticholinergics and what else?Drug Discovery Today: Therapeutic Strategies 2006 3(3):277-86. [Google Scholar]
[20]. Kiri VA, Pride NB, Soriano JB, Vestbo J, Inhaled corticosteroids in chronic obstructive pulmonary disease: results from two observational designs free of immortal time biasAm J Respir Crit Care Med 2005 172(4):460-64. [Google Scholar]
[21]. Nishimura K, Koyama H, Ikeda A, Sugiura N, Kawakatsu K, Izumi T, The additive effect of theophylline on a high-dose combination of inhaled salbutamol andipratropium bromide in stable COPDChest 1995 107(3):718-23. [Google Scholar]
[22]. Celik P, Sakar A, Havlucu Y, Yuksel H, Turkdogan P, Yorgancioglu A, Short-term effects of montelukast in stable patients with moderate to severe COPDRespir Med 2005 99(4):444-50. [Google Scholar]
[23]. Ohta K, Fukuchi Y, Grouse L, Mizutani R, Rabe KF, Rennard SI, A prospective clinical study of theophylline safety in 3810 elderly with asthma or COPDRespir Med 2004 98(10):1016-24. [Google Scholar]