Metastatic Squamous Cell Carcinoma of the Stomach
Lamine Hamzaoui1, Mahdi Bouassida2, Houda Kilani3, Mouna Medhioub4, Emna Chelbi5
1 Gastroenterologist, Department of Gastroenteroloy, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
2 Surgeon, Department of General Surgery, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
3 Histopathologist, Department of Histopathology, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
4 Gastroenterologist, Department of Gastroenteroloy, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
5 Histopathologist, Department of Histopathology, Mohamed Tahar Maamouri Hospital, Nabeul, Tunisia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lamine Hamzaoui, Mohamed Tahar Maamouri Hospital, Route d’Hammamet, Mrezga, 8000 Nabeul, Tunisia. E-mail : lamine015@yahoo.fr
Primary squamous cell carcinoma of the stomach is very rare. Its pathogenesis is unclear and the treatment strategy is controversial. We report an agressive primary squamous cell carcinoma of the stomach with liver and lung metastases in a 55-year-old man. The patient presented with a 1-month history of abdominal pain, vomiting and weight loss. Abdominal ultrasound revealed multiple liver metastases. Endoscopic examination showed two tumour masses on the fundus of the stomach. Biopsy of the lesions revealed squamous cell carcinoma of the stomach. Chest x-ray showed multiple large pulmonary nodules highly suggestive of pulmonary metastases. The patient died ten days after he was admitted because of progression of the tumour and before any therapeutic decision.
Gastric carcinoma, Immunohistochemistry, Prognosis
Case Report
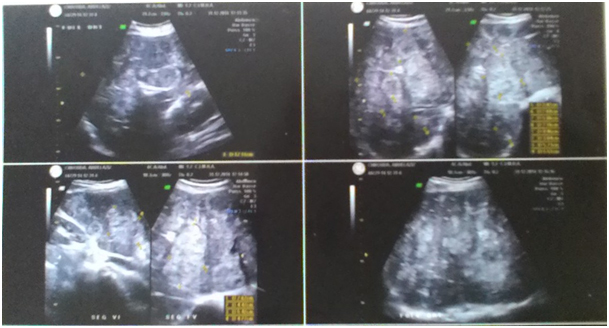
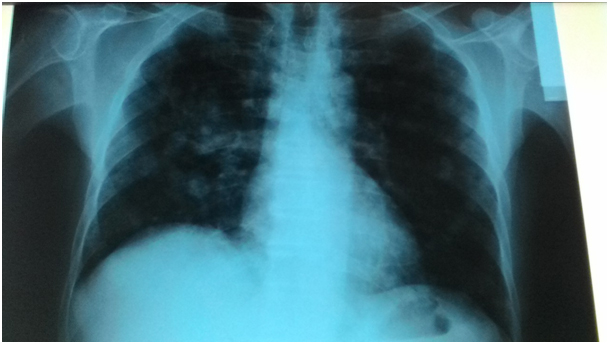
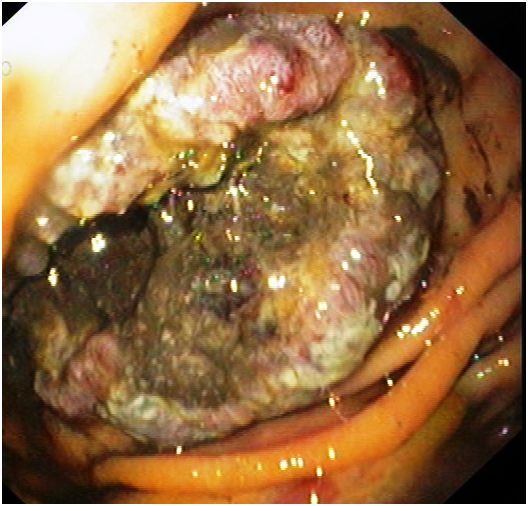
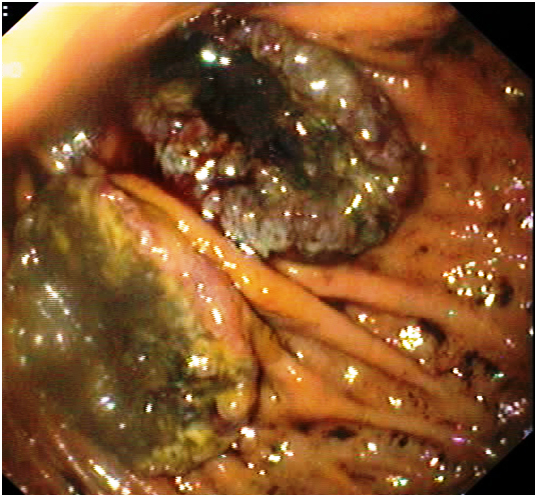
A 55-year-old man, operated for perforated bulbar ulcer 28 years ago. He was admitted in January 2015 in the gastroenterology department of Mohamed Tahar Maamouri Hospital (Nabeul / Tunisia) with a 1-month history of abdominal pain, vomiting and weight loss. History of smoking 1 pack of cigarettes per day for 30 years. Physical examination revealed jaundice and tumoural hepatomegaly. Laboratory tests showed normocytic-normochromic anemia (Hb=8.3g/dL), biological inflammatory syndrome (CRP = 130mg/L), cholestasis (Total blirubin = 54μmol/L, direct bilirubin = 45μmol/L, GGT = 502 UI/L (normal values <55 UI/L), ALP = 515 UI/L (normal values<250 UI/L), cytolysis: ALT = 386 UI/ L (normal values<40UI/L). Tumour markers (ACE/CA19-9) were normal. Abdominal ultrasound showed a diffuse infiltration of the liver by multiple hyperechoic nodules with hypoechoic center, suggestive of metastases [Table/Fig-1]. Investigations to find the primitive tumour included a chest x-ray which showed multiple, large, round and bilateral nodules suggestive of pulmonary metastases [Table/Fig-2]. Then, upper gastrointestinal endoscopy was performed and revealed two oval-shaped and ulcerated masses of the fundus, both measuring 6 cm in diameter [Table/Fig-3,4]. Several biopsies of the masses were realised and histological examination with immunohistochemistry revealed a poor-differentiated squamous cell carcinoma (SCC), p63+ with keratinization. No evidence of glandular differentiation was identified [Table/Fig-5,6 and 7]. Therefore, a probable primary SCC of the stomach with liver and lung metastases was evoked. The patient died 10 days after he was admitted because of tumour progression, before any therapeutic decision. An autopsy with histopathological examination of the whole stomach was not performed.
Abdominal ultrasound showing multiple and diffuse hyperechoic nodules of the liver with hypoechoic center
Chest-x ray showing the presence of large and multiple pulmonary nodules suggestive of «canon ball» metastases
Endoscopy: endoscopy examination revealed two large tumoural lesions located in the fundus, oval-shaped
Endoscopy: zoom on one gastric mass which is ulcerated and covered by a liquid
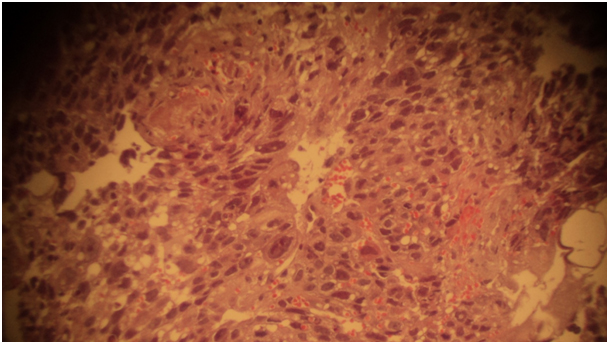
Histology: features consisting of poorly differentiated SCC, exhibiting keratinization and intercellular bridges (H&E staining; magnification- 200X)
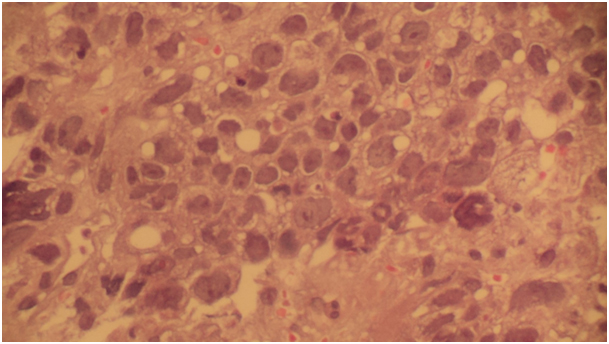
Histology: the tumour was composed of multi-mitotic cells and necrosis (H&E staining; magnification- 400X)
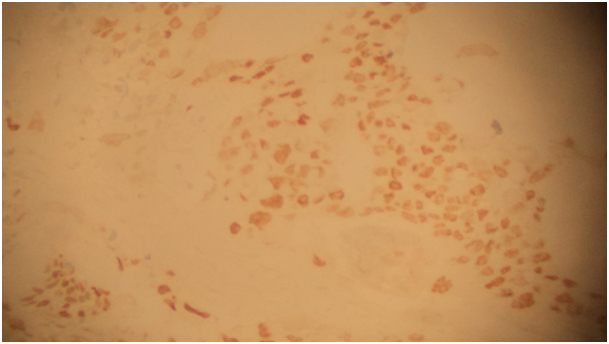
Immunohistochemistry: the immunostaining of the tumour cells was positive for p63
Discussion
Primary SCC of the stomach is extremely rare, with an incidence ranging between 0.04 and 0.09 % and < 100 cases have been reported [1]. Diagnostic criteria were proposed by the Japanese Classification of Gastric Carcinoma and consists of: SCC cells, absence of adenocarcinomatous components in any sections, SCC arising from the gastric mucosa [2].
Immunohistochemistry examination should be realised and includes CK5/6 and p63 immunomarkers [3]. Immunostaining was positive for p63 in our case. The pathogenesis of SCC remains unclear. Different pathological mechanisms have been proposed: heterotopic squamous epithelium, squamous metaplasia, multipotent stem cells able to differentiate into cells of any type, overgrowth of the squamous component in primary adenocarcinoma and local extension or metastasis of esophageal SCC [4]. Only 56 cases of primary SCC of the stomach have been reported in Japan with a median age of 64.7± 1.7 years (29 to 81 years) and a male predominance. The most common tumour location was the upper third of the stomach (57.1%), followed by the lower third (21.4%) and the middle third (19.6%). Tumour diameter was 2.1 to 13 cm (mean, 6.6±0.3 cm) [5]. There is not a particular management strategy and prognosis is difficult to predict. Surgical resection (R0= no residual tumour) remains the mainstay of the treatment. Survival periods of >3 years, in a case of advanced stage SCC with a good quality of life for five years without recurrence was reported after adjuvant chemoradiotherapy [6]. The tumour was aggressive in our patient who died before any therapeutic decision.
Conclusion
SCC is very rare. Its pathogenesis, diagnosis and treatment has been considered poor. This case presented with liver metastases and endoscopy showed two gastric masses. Diagnosis was confirmed by histological examination with immunohistochemistry. It was an aggressive tumour with a poor prognosis.
Abreviations
SCC : Squamous cell carcinoma
CRP : C-reactive protein
GGT : γ-glutamyltranspeptidase
ALP : Alkaline phosphatase
ALT: Alanine aminotransferase
[1]. Straus R, Henschel S, Fortman DJ, Primary adenosquamous carcinoma of the stomach. A case report and reviewCancer 1969 24:985-95. [Google Scholar]
[2]. Japanese Gastric Cancer AssociationJapanese classification of gastric carcinoma: 3rd English editionGastric Cancer 2011 14:101-12. [Google Scholar]
[3]. Schmidt C, Schmid A, Lutteges JE, Kremer B, Henne-Bruns D, Primary squamous cell carcinoma of the stomach. Report of a case and review of literatureHepatogastroenterology 2001 48:1033-36. [Google Scholar]
[4]. Hwang SH, Lee JH, Kim K, Shin DH, Kim JY, Sol MY, Primary squamous cell carcinoma of the stomach: A case reportOncol Lett 2014 8(5):2122-24. [Google Scholar]
[5]. Wakabayashi H, Matsutani T, Fujita I, Kanazawa Y, Nomura T, Hagiwara N, A Rare Case of Primary Squamous Cell Carcinoma of the Stomach and a Review of the 56 Cases Reported in JapanJ Gastric Cancer 2014 14(1):58-62. [Google Scholar]
[6]. Michalet V, Gaudin JL, Bancel B, El Khaddari S, Baulieux J, Rode A, Squamous cell carcinoma of the celiac area. Report of a case and review of the literatureGastroenterol Clin Biol 2002 26:1168-71. [Google Scholar]