Can Erectile Dysfunction in Young Patients Serve as a Surrogate Marker for Coronary Artery Disease?
Kaje Yogesh Dattatrya1, Tanwar Harshawardhan Vedpalsingh2, Wagaska Vinayak Gorakhnath3, Patwardhan Sujata kiran4
1 Registrar, Department of Urology, Seth G.S Medical College & KEM Hospital, Mumbai, Maharashtra, India.
2 Registrar, Department of Urology, Seth G.S Medical College & KEM Hospital, Mumbai, Maharashtra, India.
3 Registrar, Department of Urology, Seth G.S Medical College & KEM Hospital, Mumbai, Maharashtra, India.
4 Head of Department, Department of urology, Seth G.S Medical College & KEM Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Tanwar Harshawardhan Vedpalsingh, Registrar, Department of Urology, New Building, Seth G.S Medical College & KEM Hospital, E Boreges Marg, Parel, Mumbai, Maharashtra-400012, India.
E-mail: harsh_bj1@rediffmail.com
Introduction
Early diagnosis and expeditious management of coronary artery disease (CAD) has a rewarding survival benefit.
Aim
To study whether erectile dysfunction (ED) serves as a surrogate marker for CAD in a young patient.
Settings and Design
Males (n=207) between ages 20-60 years with ED were evaluated prospectively for risk factors for CAD.
Materials and Methods
Blood Glucose Levels (BGL) fasting and post meal), lipid profile (LP) and 12 lead electrocardiogram (ECG) was done in all of them. International Index of Erectile Function-5 (IEF-5) was used for the evaluation of ED. Those with abnormal parameters were assessed by cardiologists by echocardiography, stress test and if necessary coronary angiography (Non-Invasive or Invasive).
Statistical Analysis
All the data were analysed using SPSS. 16 statistical software (SPSS Inc., Chicago, IL, USA). All data are expressed as mean and standard deviation. The Student’s t-test was used to compare means between groups, and the chi-square test was used to compare proportions between the groups. P-value <0.05 was considered statistically significant. All confidence intervals (CIs) are two tailed and calculated at the 0.05 level.
Results
Out of 207, 149 patients had at least one abnormal screening parameter. All underwent cardiology consultation and 2D ECHO and Stress test. Thirty six patients underwent coronary angiography. CAD was found in 22 patients. Of these, 19 patients had severe ED. Nine patients were between 20-40 years of age (13.23%). All 9 young patients had deranged LP; severe ED. Six patients were smokers while nobody was hypertensive.
Conclusion
ED serves as a surrogate marker for CAD in young patients (p=0.001). Presence of risk factors and lab abnormalities in young patients with ED warrants a cardiology referral to detect CAD.
Coronary angiography, International Index of Erectile Function-5 (IEF-5), Smokers
Introduction
Erectile dysfunction (ED) is defined as the inability to reach or maintain an erection satisfactory for sexual performance. It is present in up to 100 million men worldwide [1]. In the Massachusetts Male Aging Study (MMAS), ED has been found to some degree in 52% of adult men between the ages of 40 and 70 years [2]. The risk of ED is directly influenced by age, number of risk factors, and presence of cardiovascular disease [2,3]. Moreover, high prevalence of ED has been reported in conjunction with vascular abnormalities, such as coronary artery disease (CAD) [4–6], hypertension [7], cerebrovascular disease [8], and peripheral arterial disease [9]. Despite these studies suggesting that ED should be classified as a vascular disease, little is known about potential mechanism(s) by which ED and CAD may be associated.
Coronary artery disease (CAD) and erectile dysfunction (ED) are closely intertwined disease processes. The temporal relationship between onset of ED symptoms and clinically evident CAD may be explained by the “artery size hypothesis” [10] which states that a larger vessel can better tolerate the same amount of plaque compared with a smaller one. Thus, a small atherosclerotic plaque burden in the narrower penile arteries would reduce blood flow and produce symptoms of ED may result, whereas a larger plaque burden would be required for obstruction and symptoms in the larger coronary artery. However, data supporting parallel development of plaques in penile and coronary arteries is inadequate, and alternative explanations should be evaluated.
Coronary circulation will not be critically affected because of its larger size, suggesting a mechanism for the theoretical lack of concomitant CAD in early-stage ED. If this hypothesis is valid, then ED should precede the onset of symptoms of CAD in the majority of cases. Available clinical evidence appears to support conclusions drawn from this hypothesis.
In India and worldwide, a large population of adult men has ED and/or CVD. Worldwide, approximately 140 million men have ED, and the number is expected to double in the next 15 years. Because ED and CVD share many of the same risk factors, the relationship between CVD and ED is a very valid concern. Among Asian Indians, there is rising trend of CAD with disease often being more extensive and severe than their Western counterpart [11,12]. Despite this, there are limited data on the prevalence of ED and its association with angiographically documented CAD in these patient populations. Patients were divided into groups based on IIEF-5 scores as no ED (22–25), mild (17–21), mild to moderate (12–16), moderate (8–11), and severe (<7) ED [13]. Patients with abnormal parameters were assessed by cardiologists by echocardiography, stress test and if necessary coronary angiography (Non-Invasive or Invasive). Significant CAD was defined as stenosis of 50% or greater in ≥1 of the major epicardial vessels or their branches. Diabetes was defined by fasting plasma glucose levels >126 mg/dL (7 mmol/L) and hypertension was diagnosed as blood pressure (BP) >140/90 mm Hg or already on antihypertensive medications [14,15]. Over the past two decades, there have been many studies that have linked both conditions and established ED as a risk factor for CVD. Data is largely exotic and may not represent Indian population. The present study was conducted with the aim to study whether erectile dysfunction (ED) serves as a surrogate marker for CAD in a young patient.
Materials and Methods
The study is a cross-sectional, observational study carried out at Seth GS medical college and KEM hospital, Mumbai a tertiary hospital in India. A total of 224 male patients between ages 20-60 years with ED were enrolled, 207 of whom were finally included in the study, which conformed to the institutional ethical guidelines. Out of which 68 patients were in age group 20-40 years (Young patient group) and 139 in age group of 40-60 years (Old patient group). They were evaluated for history of hypertension (HTN), Diabetes mellitus (DM), Ischemic heart disease (IHD) and smoking (S). BGL (fasting and post meal), Lipid Profile and 12 Lead electrocardiogram (ECG) was done in all of them. ED was evaluated and diagnosed using the International Index of Erectile Function (IIEF)-5 self-administered questionnaire, wherein ED is addressed by a five-question scoring method and each question scored 0–5. Patients with comorbidities such as thyroid disorders, renal failure, liver cirrhosis, stroke, chronic obstructive respiratory disease, hypogonadism, or traumatic causes and those who had undergone pelvic, penile, urethral, or prostate surgery or were being already treated for ED were excluded.
Statistical Analysis
All the data were analysed using SPSS 16 statistical software (SPSS Inc., Chicago, IL, USA). All data are expressed as mean standard deviation. The Student’s t-test was used to compare means between groups, and the chi-square test was used to compare proportions between the groups. P-value <0.05 was considered statistically significant. All confidence intervals (CIs) are two tailed and calculated at the 0.05 level.
Results
The demographics of the overall patient population are summarized in [Table/Fig-1].
Demographics of the overall patient population
| Variable | Overall(n= 207) | Young pt(n=68) | Older pt.(n=139) | p-value |
|---|
| Age (years) | 52.4 ± 8.6 | 32.6 ± 3.1 | 59.2 ± 6.4 | 0.024 |
| DM | 62 (22.95%) | 6 (8.82%) | 56 (40.28%) | 0.03 |
| HTN | 102 (49.27%) | 8 (11.76%) | 94 (67.6%) | 0.02 |
| Smoking | 55 (26.57%) | 24 (35.29 | 31 (22.30%) | 0.6 |
| IHD | 7 (3.38%) | 0 (0%) | 7 (5.03%) | 0.001 |
Out of 207 patient severity of ED was mild, moderate and severe in 26 (12.5%), 72 (34.7%) and 109 (52.6%) patients respectively. One hundred forty nine patients had at least one abnormal screening parameter. Abnormal lipid profile was most common screening abnormality (n=93, 44.9%) followed by abnormal ECG (n=65, 31.4%), HTN (n=43, 20.7%), deranged BGL (n=9, 4.3%). All patients with abnormal screening underwent cardiology consultation. 2D ECHO and Stress test was done when necessary. Thirty six patients underwent coronary angiography. CAD was found in 22 patients (10.62%). Nine patients were between 20-40 years of age (13.23%) and 13 patients were between 40-60 years of age (9.35%). All 9 young patients had deranged LP; severe ED. Six patients were smokers while nobody was hypertensive. While severe ED affected 10 out of 13 patients (76.9%) above 40 years of age with CAD, 6(46.1%) were smokers, 11(84.6%) had both deranged LP and HTN. Ten (76.9%) patients were diabetics [Table/Fig-2].
Demographics of patient population subsequently found to have CAD
| Variable | Young Pt.(n=9) | Older Pt.(n= 13) | p-value |
|---|
| Severe ED | 9 (100%) | 7 (53.84%) | 0.003 |
| Deranged LP | 9 (100%) | 11 (84.61%) | 0.04 |
| HTN | 0 (0%) | 11 (84.61%) | 0.0024 |
| DM | 1 (11.11%) | 10 (76.92%) | 0.001 |
| Smoking | 6 (66.6%) | 6 (46.15%) | 0.6 |
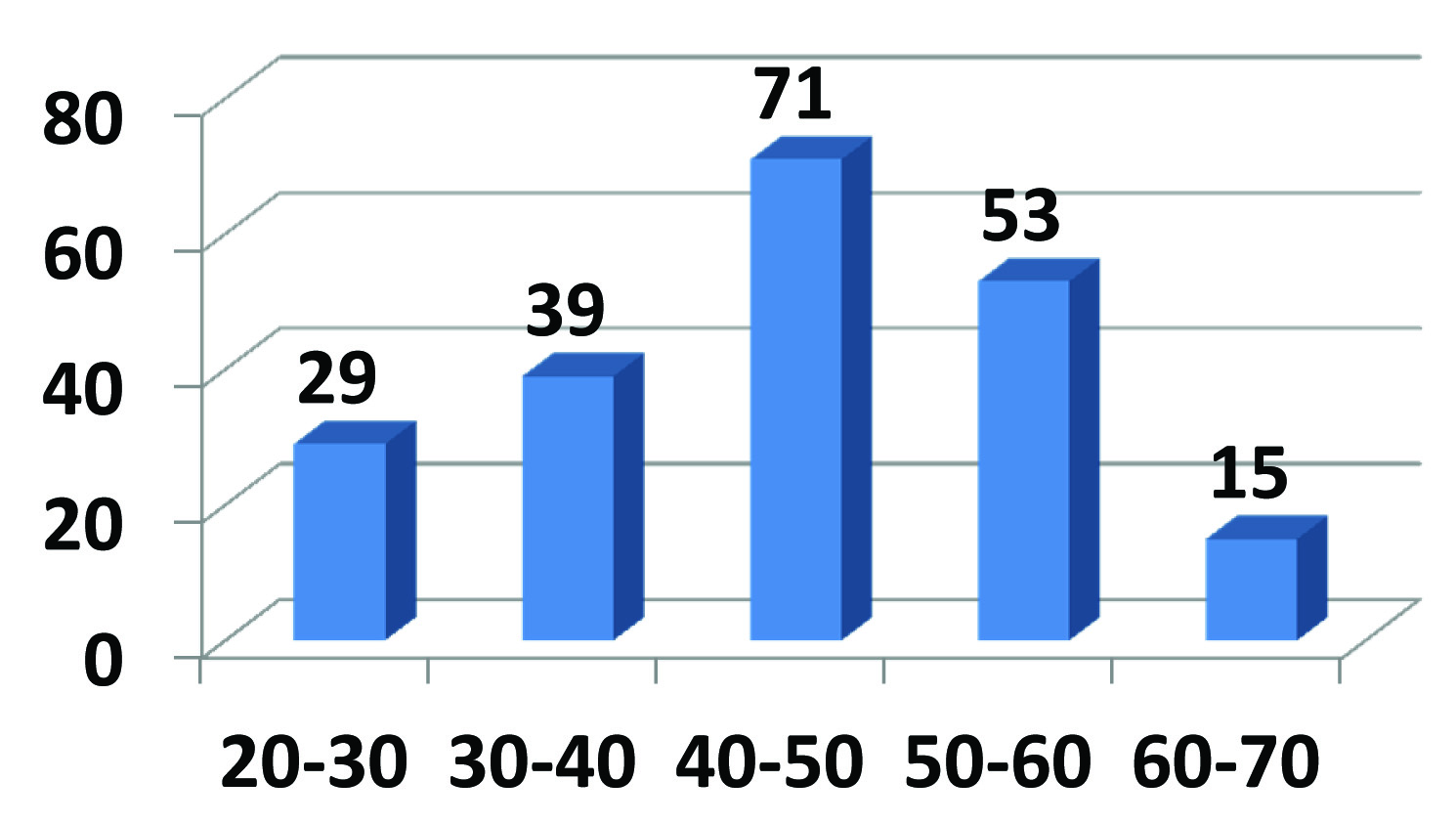
A total of 224 male patients, 207 patients between ages 20-60 years with ED were enrolled, which conformed to the institutional ethical guidelines. Out of which 68 patients were in age group 20-40 years (Young patient group) and 139 in age group of 40-60years (Old patient group) [Table/Fig-3].
Age distribution of patients (X axis- age in years, Y axis- no. of pt.)
Discussion
There are number of studies in literature mostly western that have assessed relationship between ED and risk of CVD. These studies have described the penis as a barometer of endothelial health. Endothelial diseases were largely ascribed to western lifestyle and dietary habits. Not with standing these facts, some studies have mentioned more severe ED in Indian population to our surprise. Vlachopaulos et al., carried out a similar study on 436 men and found out 13.3% rate of occult CAD in patients presenting with ED [16]. Montorasi et al., studied that in patients with established CAD, ED preceded CAD by an average of 2 to 3 years [10]. These findings support the assertion that ED is a harbinger of cardiovascular events and is related to the severity of CAD.
Three recent studies have evaluated the effect of age on the relationship between ED and cardiovascular risk. A random sample of more than 1400 community-dwelling men who had regular sexual partners and no known CAD were studied by Inman et al., [17]. These men were biennially screened for the presence of ED over a 10-year follow-up period. In their study, prevalence’s of ED were 2%, 6%, 17%, and 39% for men 40 to 49 years, 50 to 59 years, 60 to 69 years, and ≥70 years of age, respectively. The incidence densities for CAD per1000 person-years for men without ED were 0.94 (40–49-year-old), 5.09 (50–59-year-old), 10.72 (60–69-year-old), and 23.30 (≥70-year-old). CAD incidence densities increased to 48.52 (40–49-year-old), 27.15 (50–59-year-old), 23.97 (60–69-year-old), and 29.63 (≥70-year-old) for men with ED. These data suggest that while in older men, the prognostic importance of ED is diminished, ED in younger men is associated with a marked increase in the risk of future cardiac events,. Chew et al., analysed hospital morbidity data and death registrations in a retrospective cohort study of 1660 men with ED [18]. A standardized incidence rate ratio was used to compare the incidence of cardiovascular events subsequent to the manifestation of ED in this cohort to that in the general male population. They observed a significantly higher incidence of atherosclerotic cardiovascular events in men with ED than was observed in the general population (standardized incidence rate ratio, 2.2). In men 20 to 40 years of age with ED the incidence of atherosclerotic cardiovascular events was more than 7 times the incidence in the same age groups in the general population. However a poor relationship between ED and cardiovascular events was observed with increasing age. The incidence rate ratios were also not statistically significant in men 70 years and older.
Recently, a case control study involving 242 men (mean age, 58 years) referred for elective coronary angiography was performed by Riedner et al., [19]. One hundred fourteen men had significant CAD. CAD was not associated with increased likelihood of ED in men ≥60 years (p = 0.5). However, men below 60 years with CAD were significantly more likely to have ED than those without CAD (p = .009). The probability of CAD was 2.3 times higher in men below 60 years of age with ED versus those without ED (p = 0.04) in a statistical model that controlled for the effects of cardiovascular risk factors, testosterone and C-reactive protein. No association between ED and probability of CAD was found in men ≥60 years (p = 0.3). Above mentioned studies support ED as a surrogate marker of CAD in men in their third, fourth, fifth and sixth decades and suggest that ED screening is a valuable means of identifying young and middle-aged men who are candidates for cardiovascular risk assessment and medical intervention.
Another study by Jackson et al., suggested that ED is a useful predictor of subclinical, non–flow-limiting CAD that is not detectable using stress ECG. Stress myocardial perfusion single-photon emission CT is a technique commonly used to diagnose and stratify CVD [20]. Min et al., studied 221 men referred for the same and found that men with ED exhibited more severe coronary heart disease than men without ED (43% vs. 17%, respectively) [21]. Left ventricular dysfunction was also significantly more common among men with ED (24% vs. 11%). The prevalence of ED in Asian Indian patients undergoing coronary angiography was studied by Jatinder Kumar et al., [22]. Whether the severity of ED correlates with angiographic severity of CAD was also studied. Kumar J et al., found out that, among 175 patients evaluated, ED was present in 70%. There was higher incidence of multi vessel CAD (80% versus 36%, p 0.001), diffuse CAD (81% versus 34%, p 0.001), and higher number of mean coronary vessels involved in patients with ED compared with those without ED (especially those with severe ED). Symptoms of CAD were preceded by onset of symptoms of ED by a mean of 24.6 months [22]. Number of patient approaching tertiary care hospital for evaluation of ED is increasing. On routine evaluation of ED along with few specialised tests, we could detect CAD in 10.62% of otherwise asymptomatic young patients. Incidence of CAD in this age group without ED is within the range of 1-3.3 %. These statistics belong to Indian population. In present study, P-value of ED for detection of CAD in younger patients was significant (p= 0.001) than in older patients. Similarly deranged LP (p=0.04) and DM (p=0.003) were powerful predictors of CAD in young and older patients respectively.
Limitations
We did not perform physiological ED vascular studies including anatomical or functional evaluation of penile circulation and testing for inflammatory markers in our patient population and primarily categorized ED based on the IIEF-5 score. Further studies are needed to assess the role of physiological ED vascular studies and inflammatory markers in these patients. In patients with normal coronaries on invasive coronary angiography (which is the gold standard for this), we did not perform any further imaging such as computed tomography coronary angiography. Coronary intravascular ultrasound or assessment of coronary flow reserve may provide more definitive information in patients with early coronary atherosclerotic changes and a normal coronary angiogram because coronary angiography is at best a lumenogram, which may not detect true plaque volume extension. We excluded patients already being treated for ED and this may have artificially reduced the actual number of ED patients in the study group. Although lack of a control group is also a limitation of the study, the main aims of the study were to prospectively assess the prevalence of CAD in Asian Indian patients undergoing evaluation of ED.
Conclusion
Presence of an ED in a patient below 40 years of age serves as a surrogate marker for CAD. Presence of risk factors and lab abnormalities in patients with ED warrants a cardiology referral to detect CAD.
[1]. Lue TF, Erectile dysfunctionN Engl J Med 2000 342(24):1802-13. [Google Scholar]
[2]. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB, Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging StudyJ Urol 1994 151(1):54-61. [Google Scholar]
[3]. Bortolotti A, Parazzini F, Colli E, Landoni M, The epidemiology of erectile dysfunction and its risk factorsInt J Androl 1997 20(6):323-34. [Google Scholar]
[4]. Solomon H, Man JW, Wierzbicki AS, Jackson G, Relation of erectile dysfunction to angiographic coronary artery diseaseAm J Cardiol 2003 91(2):230-31. [Google Scholar]
[5]. Kloner RA, Mullin SH, Shook T, Matthews R, Mayeda G, Burstein S, Erectile dysfunction in the cardiac patient: how common and should we treat?J Urol 2003 170(2 Pt 2):S46-50.discussion S50 [Google Scholar]
[6]. Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi A, Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery diseaseEur Urol 2003 44(3):360-4.discussion 364-65 [Google Scholar]
[7]. Burchardt M, Burchardt T, Anastasiadis AG, Kiss AJ, Shabsigh A, de La Taille A, Erectile dysfunction is a marker for cardiovascular complications and psychological functioning in men with hypertensionInt J Impot Res 2001 13(5):276-81. [Google Scholar]
[8]. Korpelainen JT, Kauhanen ML, Kemola H, Malinen U, Myllylä VV, Sexual dysfunction in stroke patientsActa Neurol Scand 1998 98(6):400-05. [Google Scholar]
[9]. Virag R, Bouilly P, Frydman D, Is impotence an arterial disorder? A study of arterial risk factors in 440 impotent menLancet 1985 1(8422):181-84. [Google Scholar]
[10]. Montorsi P, Montorsi F, Schulman CC, Is erectile dysfunction the “tip of the iceberg” of a systemic vascular disorder?Eur Urol 2003 44(3):352-54. [Google Scholar]
[11]. Misra A, Pandey RM, Devi JR, Sharma R, Vikram NK, Khanna N, High prevalence of diabetes, obesity and dyslipidaemia in urban slum population in northern IndiaInt J Obes Relat Metab Disord 2001 25(11):1722-29. [Google Scholar]
[12]. Enas EA, Coronary artery disease epidemic in Indians: a cause for alarm and call for actionJ Indian Med Assoc 2000 98(11):694-5.:697-702. [Google Scholar]
[13]. Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH, Diagnostic evaluation of the erectile function domain of the International Index of Erectile FunctionUrology 1999 54(2):346-51. [Google Scholar]
[14]. Standards of medical care in diabetes—2011American Diabetes AssociationDiabetes Care 2011 34(Suppl 1):S11-61. [Google Scholar]
[15]. Jones DW, Hall JE, Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and evidence from new hypertension trialsHypertension 2004 43(1):1-3. [Google Scholar]
[16]. Vlachopoulos C, Ioakeimidis N, Aznaouridis K, Terentes-Printzios D, Rokkas K, Aggelis A, Prediction of cardiovascular events with aortic stiffness in patients with erectile dysfunctionHypertension 2014 64(3):672-78. [Google Scholar]
[17]. Inman BA, Sauver JL, Jacobson DJ, McGree ME, Nehra A, Lieber MM, A population-based, longitudinal study of erectile dysfunction and future coronary artery diseaseMayo Clin Proc 2009 84(2):108-13. [Google Scholar]
[18]. Chew KK, Finn J, Stuckey B, Gibson N, Sanfilippo F, Bremner A, Erectile dysfunction as a predictor for subsequent atherosclerotic cardiovascular events: findings from a linked-data studyJ Sex Med 2010 7(1 Pt 1):192-202. [Google Scholar]
[19]. Riedner CE, Rhoden EL, Fuchs SC, Wainstein MV, Gonçalves SC, Wainstein RV, Erectile dysfunction and coronary artery disease: an association of higher risk in younger menJ Sex Med 2011 8(5):1445-53. [Google Scholar]
[20]. Jackson G, Boon N, Eardley I, Kirby M, Dean J, Hackett G, Erectile dysfunction and coronary artery disease prediction: evidence-based guidance and consensusInt J Clin Pract 2010 64(7):848-57. [Google Scholar]
[21]. Ko SM, Song MG, Chee HK, Hwang HK, Feuchtner GM, Min JK, Diagnostic Performance of Dual-Energy CT Stress Myocardial Perfusion Imaging: Direct Comparison With Cardiovascular MRIAJR Am J Roentgenol 2014 203(6):W605-13. [Google Scholar]
[22]. Kumar J, Bhatia T, Kapoor A, Ranjan P, Srivastava A, Sinha A, Erectile dysfunction precedes and is associated with severity of coronary artery disease among Asian IndiansJ Sex Med 2013 10(5):1372-79. [Google Scholar]