“Why We Say No! A Look Through the Editor’s Eye”
Aarti Garg1, Sunanda Das2, Hemant Jain3
1 Assistant Editor, Journal of Clinical and Diagnostic Research, Delhi, India.
2 Assistant Editor, Journal of Clinical and Diagnostic Research, Delhi, India.
3 Editor-in-Chief, Journal of Clinical and Diagnostic Research, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hemant Jain, Editor-in-Chief, 1/9 Roop Nagar, Below Punjab National Bank, GT Road, Delhi-110007, India.
E-mail: drhemantjain@jcdr.net
Correction:
This article has been updated on 1 Feb 2016, to see correction please see link which is given below:
http://jcdr.net/article_fulltext.asp?issn=0973-709x&year=2016&volume=10&issue=2&page=ZZ01&issn=0973-709x&id=7514
Background
The rapidly flourishing health science has provided a ground to perform research work and contribute to the field of science. On the other hand, reporting the research is equally important as carrying out research. Many such researches and their ground breaking work remain unreported or do not reach the guild, because of poor drafting skills. In nine years since Journal of Clinical and Diagnostic Research (JCDR) inception, editorial have come across many manuscripts which are clinically and socially relevant in their message, but lack legible drafting. It was felt that an objective analysis of the reasons for rejection, of manuscripts, is required.
Aim
The present study was conducted with the aim to determine the reasons for rejection of medical and dental manuscript submitted in JCDR.
Materials and Methods
Retrospective analysis of 1000 consecutive medical and dental articles submitted to JCDR since 1st August 2014 was done. Only those articles (902) that reached the end point on decision were considered. The reasons of rejection for medical and dental articles were enlisted and analyzed. When there were multiple reasons of rejection and all of them were critical, then they were counted in all the categories.
Results
Out of the 902 consecutive articles 522 articles underwent rejection. Among the rejected ones, dental specialty comprised of 43.5% and medical articles contributed 56.5%. The most frequent reasons for rejection were commonality (44.6%), non compliance by authors (17.8%), methodological issues (17.3%), plagiarism (11.1%), received same topic and published (7.66%), poor draft (6.70%), data inconsistency (5.77%), mismanagement (1.72%), blacklisted author (1.14%), ethical and out of scope were 0.57% each.
Conclusion
Based on our findings, it can be concluded that manuscript rejection can be avoided by the authors, if the topic is well choosen and communication is maintained with the journal editorial.
Fabrication, Manuscript, Plagiarism, Peer review, Rejection
Introduction
The publication of a scientific work is a vital part of a researcher’s career and lists among his aspirations. Researchers always look forward to publish their findings in reputed scientific journals and getting it utilized and recognized by fellow scientists, thus making their contribution available globally for referencing.
In India, the medical/dental education governing bodies (DCI/MCI) have impromptu linked publications with promotions [1,2]. Similar norms exist in institutions across the world. This has facilitated the intellectual curiosity as well as given a much needed push to conduct research and even more to get it published. This scientific revolution, has also lead to the rapid proliferation of journals [3].
The inclusion of research works and publications in the curriculum has been a milestone in the field of health science. But still much remains to be harnessed from a researcher’s mind. The status of publication remains far behind than what can be said as an achievement.
In the process of publication, peer–reviewed journals, appear to be the best platform for sharing the research findings [4]. The peer review process decides the fate of a manuscript. However, a substantial number of articles do not even reach the peer-review process [5]. Thus there are two levels where a manuscript gets rejected – editorial and peer review [6].
Editors of journals, now and then have looked out for reasons why a manuscript gets rejected [1,5,7–10]. A lot of reviews and guidance for drafting scientific manuscript exists. However, a systemic and objective analysis of data regarding manuscript rejection has been done only occasionally.
After reviewing literature, we could locate only a few original articles relating to reasons for rejection [4,6,8,11–19]. Most of these studies were more than a decade old and were introspections of a specialty journals. No such study was done by a widescope journal or by a journal accepting dental articles. Few journals have published original articles after reviewing their own data [6,8,11,14–17]. Among them the most extensive analysis was done by the Canadian Journal of Anesthesia [15]. There was a questionnaire based study in 2000, that evaluated data based on the response of editors/reviewers/nobel laureates [8]. However, as the response rate was noticeably low (22%), the facts can not be taken with certainty. A more recent study in 2013 [4] drew conclusions from meager 42 manuscripts, published across eight different biomedical journals spread over two continents. Considering the volume of submissions and rejections the number of submissions considered were small to reflect a global scenario. Very few of these studies have detailed the reasons of rejection specific to case reports [15,17].
JCDR is a free access, peer reviewed, indexed, international, biomedical journal (ISSN - 0973-709X). It includes all medical and dental specialties. The authors who are the editors in this journal, while working on manuscripts felt need to evaluate the reasons for rejection in a more objective manner, in process to guide prospective authors and a chance for journal to introspect its own decisions. Further, editors had a general feeling that the sudden rush of publication has led to lot of cutting corners and bending of ethical norms.
Materials and Methods
All manuscripts and their processing status-related information were obtained from the JCDR editorial data-base with the permission of the editor-in chief. A retrospective analysis was conducted to categorize the reasons for rejections.
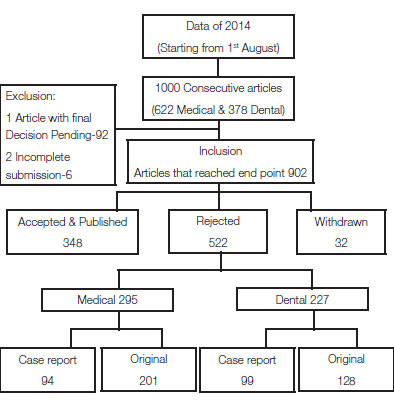
The editors associated with journal change over a period of time and so do active peer reviewers. Therefore, a narrow period of study, which will remove the inadvertent bias. The mammoth task of going through decisions on 1000 consecutively submitted manuscripts since 1st August 2014, both medical and dental was undertaken. Only those articles that had reached the end point on decision were considered, i.e. accepted, published, rejected and withdrawn. Articles with final decision pending, along with those that were not processed because of incomplete submission were excluded from the study. [Table/Fig-1].
Flowchart showing the chronology of assessing the articles and the obtained results
The final decision based on which an article has been rejected was traced (editorial and/or peer review level) and then these reasons were categorized. The articles were divided into original (including reviews) and case reports (including case series, images in medicine, short communication and letter to editor) of medical and dental specialties. If there were more than two reasons and both of them were considered critical, then they were included under multiple categories.
Since the journal includes both medical and dental sections, the difference of reasons of rejection between them was also studied, to find if any variation can be delineated between the two.
Results
Of 902, 522 (57.87%) articles underwent rejection. Among the rejected ones, 295 articles were medical and 227 were of dental specialty. The reasons for rejection are depicted in [Table/Fig-2,3 and 4].
Depicting the reasons of rejection of medical and dental Case Reports
| Serial No. | Reasons For Rejection | MedicalN=94* | DentalN=99* |
|---|
| 1 | Common | 31 | 66 |
| 2 | Poor draft | 7 | 5 |
| 3 | Incomplete Case | 5 | 6 |
| 4 | Medical Mismanagement | 4 | 3 |
| 5 | Non Compliance of Author | 40 | 7 |
| 6 | Received Same Topic And Published | 3 | 11 |
| 7 | Plagiarism | 11 | 6 |
| 8 | Ethical issues | - | 1 |
* For articles that were rejected for more than one reason (both critical), it was counted in both the categories. Hence the numbers would not add up
Depicting the reasons of rejection of medical and dental Original articles
| Serial No. | Reasons For Rejection | MedicalN=201* | DentalN=128* |
|---|
| 1 | Common | 72 | 64 |
| 2 | Methodology issues | 39 | 18 |
| 3 | Plagiarism | 31 | 10 |
| 4 | Received Same Topic and Published | 16 | 10 |
| 5 | Non Compliance Of Author | 33 | 13 |
| 6 | Blacklisted Author | 3 | 2 |
| 7 | Poor draft | 16 | 7 |
| 8 | Topic out of Scope of Journal | 3 | - |
| 9 | Medical Mismanagement | 2 | - |
| 10 | Data Inconsistency/fabrication | 12 | 7 |
| 11 | Ethical issues | 1 | 1 |
* For articles that were rejected for more than one reason (both critical), it was counted in both the categories. Hence the numbers would not add up
Overall percentage of reasons of rejection
| Serial No. | Reasons of rejection | Medical | Dental | Total numbers | Percentage (%) |
|---|
| 1 | Common | 103 | 130 | 233/522 | 44.63 |
| 2 | Non compliance of author | 73 | 20 | 93/522 | 17.81 |
| 3. | Methodology issue | 39 | 18 | 57/329 | 17.32 |
| 4 | Plagiarism | 42 | 16 | 58/522 | 11.11 |
| 5 | Received same topic and published | 19 | 21 | 40/522 | 7.66 |
| 6 | Poor draft | 23 | 12 | 35/522 | 6.70 |
| 7 | Data inconsistency/fabrication | 12 | 7 | 19/329 | 5.77 |
| 8 | Incomplete cases | 5 | 6 | 11/193 | 5.69 |
| 9 | Medical Mismanagement | 6 | 3 | 9/522 | 1.72 |
| 10 | Blacklisted author | 3 | 2 | 5/522 | 0.95 |
| 11 | Ethical issues | 1 | 2 | 3/522 | 0.57 |
| 12 | Out of scope of journal | 3 | - | 3/522 | 0.57 |
Discussion
The peer review process has norms that is followed by all peer reviewed journals. In JCDR, too, there are steps of screening articles before they reach the editor’s desk or are sent for peer review. The incomplete submissions get rejected at the level of technical screening. All the complete submissions then reach the technical staff who upload a plagiarism report using a plagiarism checking software, make blinded files and forward it to assistant editors, who further recheck the plagiarism report and in addition the topic relevance in terms of published data both in international literature and within published titles of JCDR. With all these inputs, the article is forwarded to specialty editors with broad marking as to be considered for rejection or to be processed further. Articles under rejection list are rescrutinized and decisions taken in consultation with Chief editor. Those which are recommended for further processing are skimmed through and are sent for peer review. In case of original articles, data verification is an added step which junior editors perform with the help of a statistician. The review report with additional inputs based on the internal assessment of article is then sent to the author. Our own data analysis for 2014 showed that approximately 48% of all the submitted articles get rejected, of these rejected articles one third are rejected at the editorial level without being sent for peer review. Peter Thrower (Elsevier) also noted that 30 to 50 percent articles do not make it to the peer review process [5].
Reasons for Rejection: Our experience with 522 articles that were rejected-
Commonality – This accounted for 44 percent of the reason for rejection. Our in-house definition of Commonality includes: topic that has been well studied previously both by international and national researchers, information present in standard textbooks or present no new perspective. Further, it also includes studies whose results have lost their relevance in current times, as techniques described are obsolete or surpassed by better alternatives [9]. Most but not all these rejections happen at editorial level itself. Gupta et al., also found around 50% rejection based on absence of message and poor originality in Indian Pediatrics [6].
Articles in Grey zone: Includes those original works which have been discussed in western literature and not much by national authors. Our view is that if such study result is likely to vary with the population studied, then it is allowed to go for peer review, if no other flaw is found on initial screening.
It is important to note that, at times, an uncommon aspect is present in an article however the author has not highlighted the same. At other times authors have noticed an uncommon secondary result, but played it down since they were not sure how to defend it in absence of supportive literature. These authors forget that the whole idea of repeating research is to discover these differences and not be apprehensive to discuss such outcomes. When a topic which comes to senior editor’s desk for rejection are based on commonality one singular question is asked : is there any uncommon or yet undiscussed feature brought out by the article? If the answer is yes then the article merits reassessment. It is worth mentioning that editors have time constrains and have to screen through a wide range of articles. If authors bring out this uniqueness in their article themselves, it becomes less likely to face rejection.
Methodology issues – It is the second most common cause of rejection among original articles. It was found that researchers might have started a project without giving a deep thought to all the methodological aspects. After completion of the study the error comes up, thus invalidating the research work. Before initiating a research, statistical and methodological issues need to be evaluated. Some of such issues can be, sample size, faulty selection criteria, flawed study design, weak analysis, unaccounted confounders and the methodology considered does not correspond to the aim [3,17].
These aspects of methodology were not adequately dealt with researchers, specially in dental articles. eg. saliva has been used as a diagnostic tool by many researchers. The results vary even if the complete methodology has been repeated by another researcher. The facts are hidden in the bias created by difference in sample collection procedure. What is commonly omitted by many, is that if saliva collection is done after mouth rinsing, the ions get diluted and hence lead to variation in result.
Although these facts might be well known, it must be emphasized because this leads to wastage of a lot of hard work and frustration of the researcher.
Non compliance of author– It comprised of 18% of all the rejections. This aspect comes into play once the first feedback has been sent by the journal. Usually 3 week period is given to author to resubmit the revision. The period was extended on valid requests. Failure to submit the revised manuscripts accounted for 10% rejections of the 18%. In these instances, the editorial takes a serious note and it does impact indirectly the future decision of the journal if author or any of the co-author resubmits another manuscript to the journal [20]. This non serious attitude leads to waste of editorial and most importantly, peer review time. Second most common reason within this group was the authors who did cosmetic corrections following only few suggestions suggested by the peer reviewer. At times author may not agree with reviewer suggestions, that is never an issue. However, author is required to provide reasons why he feels the corrections should not be done [21]. At other times we have come across certain good quality, although poorly drafted research works. The refusal of author to improve the draft led to a negative decision. On the other hand there were authors who diligently work on their revisions. They were appreciated and even if further revisions and editorial inputs were needed, these were readily offered. Author should always aim to carry the manuscript through publication and not abandon it midway because of negative comments by the reviewer [20]. If the editor indicates willingness to evaluate a revision, it means the manuscript may be publishable if the reviewers’ concerns could be addressed satisfactorily [22]. It is important to note that, returning authors are remembered by editorial and these factors do tangentially effect decisions, with due diligence, especially if negatives exist. In the process, what remains a bitter fact is that, such noncompliant behavior leads to a lot of revenue and logistic loss for the journals which do not charge upfront processing fee, but charge fee only for the accepted manuscripts. The authors of medical specialty were found to have a more noncompliant behavior in comparison to the dental specialty.
Failure to submit revision has been occasionally mentioned but never been deeply analyzed. Canadian Journal of anesthesia, which conducted a very detailed and structured study, did not enlist failure to send revised submission as a reason for rejection [15]. One study in Indian subcontinent by Gupta et al., analyzing the data of Indian Paediatrics (2002), found 7% noncompliance by authors, but this category also included those articles that were withdrawn and had ethical reasons [6]. Either this was not a real factor a decade back or was under reported. One proposed explanation can be that with push of publication authors tend to submit manuscript simultaneously to more than one journal and whichever journal gives quicker and positive response is continued. The other journal is abandoned without any communication. The real reason can be known only once the fate of articles rejected under this category is analyzed.
Plagiarism – This accounted for 11% of the reasons for rejection. The impact of plagiarism vary depending upon the type of article i.e. research work, case reports and reviews [23]. There are many views as well as guidelines on this aspect [BMJ, COPE] The part of manuscript where plagiarism has been detected has to be considered important for further processing of the article. [13,24–28].
The process to check plagiarism is both automated and manual. Though there are well-recognized softwares that have lessened the manual work immensely [29], however even such softwares have flaws, like figures and equations can not checked [30]. There were quite a number of manuscripts, that cleared such automated checks but got caught when rechecked manually. The rechecks were at times done on a hunch or due to certain valid reasons associated with manuscript drafting or author’s reputation. Hence, we recommend, decisions should not be solely based on automated plagiarism reports, they must be re-evaluated manually. This fact is supported by a study conducted by Croatian journal of Anesthesia [24].
We encountered a case report in which the case was new and unique however introduction as well as discussion was heavily plagiarized. Internationally, such articles are rejected outright, however the author was allowed one opportunity to redraft the article. On the other hand in case of an original article, if the results and discussion was found to be plagiarized then the article was rejected.
Self Plagiarism– Out of 58 articles that were rejected for plagiarism, 23 were self plagiarized. Croatian medical journal found 85 plagiarized manuscripts of which 22 were self plagiarism [25]. Slicing own research work for the sake of increasing the number of publications, is also considered as self plagiarism.
Plagiarism of Images – One article was rejected as the image was not original, but a cropped image picked from Google database. This was a photomicrograph and it could be traced to the Google database. The author confessed when the editorial communicated with him.
Ethical issues – Three articles were rejected due to ethical concerns. Ethical concerns in publication are same across the globe. However few issues which were faced repeatedly are highlighted here.
Patient issues: As per norms, the patient consent or ethical committee approval is asked for while submitting the manuscript [10]. Authors have been asked to furnish required documents whenever editor or peer review felt it necessary. They were rejected if author could not comply. In dental case reports, the patient consent and de-identification, holds importance as the patient identity gets revealed in most of the cases.
Authorship issues: Articles have been rejected when, upon search, it was found to be listed as thesis work of a postgraduate and in the list of authors presented to us, the primary investigator’s name was missing. Such matters are further complicated when the primary investigator is not amongst the first two/three authors or the guide is not enlisted as an author or acknowledged in the article. Regarding such conflicts, we had discussion with senior editors of other reputed journals and ironically came across conflicting opinions.
Discussion of such dilemma that may or may not lead to rejection are beyond the scope of current manuscript. Though according to COPE guidelines, the authorship is decided by the author and not the journal [28]. And journal is not to arbitrate between authors, however, many a times we have been inadvertently pulled into center of the conflict.
There was a case report where it was required to ascertain the originality of the case as it was a rare variation. In this case, a calculi was removed from a visceral organ. Only the gross image of the calculi was presented with no supportive investigations. Hence, the copy of discharge summary of the patient was requested from the author, to authenticate the case. Author was unable to furnish any details and the article was rejected.
Poor drafting – There are two aspects of this. One, poor English language and other the flow of the article or the subsection break if not conform to journal guidelines. Both aspects are weighed differently. In JCDR, as rule of thumb, the language is not taken in isolation for rejection. Many of our authors are not native English speakers, hence an opportunity is given, as cited by other journals also. Similarly, improper flow of the article does not in isolation merit rejection, as there are many inexperienced writers, however in extreme cases exceptions do happen. Failures to correct the above issues in revised files are viewed negatively and have lead to rejection. The concern regarding language might be a bigger issue for journals who receive articles from non-english speaking authors [5,14,25]. Unlike us, many journals are more stern during their initial screening if the drafting is poor.
Around 7% manuscripts had drafting and language issues for which they were rejected, although it was not the sole reason for rejection. Only one manuscript had a major problem with drafting and hence was rejected based on the same.
Topic Out of scope of journal – For certain journals that cover few specialties, rejections based on this aspect, may be more compared to us, we being a widescope journal. But there are many fields of science that has to be dealt with separately or with special consideration, as in, psychology, environment science, etc. Before submitting a manuscript an author should go through the subjects that a journal deals with, can mail or have a telephonic conversation with the editor to know the subjects covered by a journal. A pre information on this will lead to avoiding the wastage of editorial time as well as reduce author’s anxiety [9].
Blacklisted author – There was an incident where an author had submitted three articles and all were under process. One of them was found to have a serious issue which put in doubt the originality of the work submitted. Hence the author was debarred and his all other submissions were by de-facto rejected.
Data inconsistency/fabrication- This parameter is for original articles and it accounted for 5.7% of our rejections. Flaws in the data can be broadly classified into two types. One, obvious data inconsistency within the article i.e. numbers not matching in abstract, results and table. An occasional typographical error is ignored, however more than that goes fatally against the article. In addition, besides being consistent throughout, the data or result should reflect the real life scenario. A huge variation should be accompanied with an appropriate justification by author [10,28]. Second, when our in-house statistical calculation differed in absolution, author was asked to submit the original data. If the author refused to share the data the manuscript was rejected [5,9,12].
Data issues in revised file - If a change in data has been observed in revised files which cannot happen without redind the study, it reflects fabrication. For example, a reviewer had pointed out the lack of a control group, and in the subsequent revision instead of adding it as a limitation or justifying the redundancy for a control group, a previously nonexistent control group was added. There were rare exceptions also. An example of when it was acceptable to change original data: an author encountered more cases by the time article had been through second revision. Then he had asked prior permission and editors felt it will strengthen the article and thus addition of cases was allowed.
Wrong diagnosis, unjustified management, false claim (morphed image): This is for case reports or images in medicine and accounted for almost 2% of our rejections. In case reports, if diagnosis was wrong, based on concurrence of two peer reviewers, the article was rejected. Further, if the treatment imparted appeared unconventional, reasoning for the same was asked from the author. The manuscript was considered only if a satisfactory justification was provided. In suspicious cases or cases with excellent visual outcomes, images were checked to rule out forging/morphing. In more than one incidence a discovery of false claim of healing by morphing an image, led to rejection of article. This issue has made the editors sought more and more help from in-house graphic experts. This aspect has rarely been dealt in literature and we feel more journal editors peer reviewers should be aware of this [31]
When a doubt arose in photomicrographs, the scanned copy of the histopathology report, was asked, failure to do so led to rejection of article. Images which depict clinical examination done with unsterile practices brought negative reviews. As in, an ungloved hand demonstrated an intraoral lesion.
Received same topic more than once within short span of time – A nicely written draft was also put for rejection as the topic has already been covered by the journal recently. This is an unfortunate but unavoidable situation in which article is rejected for no fault of authors. At other times authors were given the opportunity to highlight the work/result which go further from the published article.
Learning Lessons
The process of data analysis and compilation of this manuscript has been a journey that made us to go through a lot of introspection. We came across few incidents where the decision taken by our own team was felt to be stern. Also certain breaches were noticed which happened inadvertently. The decisions are largely dependent on peer review system which in itself has weakness and pitfalls. The reasons for rejection that have been enlisted in this manuscript might have been overlooked by the editorial team handling the early years of publication. We could roughly estimate our in-house screen value against the peer review reports. Being a young journal we still have miles to go in improving our services.
Conclusion
This study, conducted with constraints of including only 1000 articles, found that the overall rejection rate of articles submitted to JCDR, was around 57.87%. Most of the articles were rejected as the topics chosen were not very innovative and were already much studied. Hence, the topic needs to be chosen well, methodology properly thought through, in consultation with a statistician, draft to be read well by a language expert and run through a plagiarism software. Another feature which was observed was that, most of the reasons for rejections can be avoided by improving inter author and author-journal communication. There are areas where more detailed study is required. The author-guide conflict is one of them. Also, limitations of a journal in holding responsibility for an ethical misconduct of an author should be defined, especially when the governing bodies do not have strict rules for such authors.
* For articles that were rejected for more than one reason (both critical), it was counted in both the categories. Hence the numbers would not add up
* For articles that were rejected for more than one reason (both critical), it was counted in both the categories. Hence the numbers would not add up
[1]. Eligibility Criteria to be a P.G. Teacher. http://0801.nccdn.net/1_5/08f/3c0/217/DCI-PG-Teacher.pdf [Google Scholar]
[2]. Minimum Qualifications for Teachers in Medical Institutions Regulations, 1998. http://www.mciindia.org/Rules-and-Regulation/TEQ-REGULATIONS-06.08.12.pdf (amended upto 2012) [Google Scholar]
[3]. Ajao OG, Some reasons for manuscript rejection by peer-reviewed journalsAnnals of Ibadan Postgraduate Medicine 2005 3(2):9-12. [Google Scholar]
[4]. Ezeala CC, Nweke IN, Ezeala MO, Common Errors in Manuscripts Submitted to Medical Science JournalAnn Med Health Sci Res 2013 3(3):376-79. [Google Scholar]
[5]. Thrower P. Eight Reason I Rejected Your Article. Linked- http://www.elsevier.com/connect/8-reasons-i-rejected-your-article [Google Scholar]
[6]. Gupta P, Kaur G, Sharma B, Shah D, Choudhury P, What is submitted and what gets accepted in Indian Pediatrics: Analysis of Submission, review Process, Decision Making, and Criteria for RejectionIndian Pediatrics 2006 43:479-89. [Google Scholar]
[7]. Pierson DJ, The top 10 Reasons Why Manuscript Are Not Accepted for PublicationRespir Care 2004 49(1):1246-52. [Google Scholar]
[8]. Byrne DW, Common Reason for Rejecting Manuscript at Medical JournalScience Editor 2000 23(2):39-44. [Google Scholar]
[9]. Fonseca M. Most common reasons for journal rejection. Linked: http://www.editage.com/insights/most-common-reasons-for-journal-rejections [Google Scholar]
[10]. Plotkin H, How to get your paper rejectedBMJ 2004 329:1469doi: http://dx.doi.org/10.1136/bmj.329.7480.1469. http://www.bmj.com/content/329/7480/1469 [Google Scholar]
[11]. Kan CC, Lockefeer JH, Overbeke AJ, Reasons for rejection of articles vor publication in the NederlandsNederlands Tijdschrift voor geneeskunde 1991 135(19):840-45. [Google Scholar]
[12]. Boradage G, Reasons Reviewers Reject and Accept Manuscripts: The Strengths and Weakness in Medical Education ReportsAcademic Medicine 2001 76(9):889-96. [Google Scholar]
[13]. Masic I, Plagiarism in Scientific PublishingActa Inform Med 2012 20(4):208-13. [Google Scholar]
[14]. Wyness T, Mcghee CNj, Patel DV, Manuscript rejection in ophthalmology and visual science journals: identifying and avoiding the common pitfallsClin Experiment Ophthalmol 2009 37(9):864-67. [Google Scholar]
[15]. Turcotte C, Drolet P, Girard M, Study Design, originality and overall consistency influence acceptance or rejection of manuscripts submitted to the journalCan J Anesth 2004 51(6):549-56. [Google Scholar]
[16]. Bloemenkamp DG, Walvoort HC, Hart W, Overbeke AJ, Duplicate publication of articles in the Dutch Journal of MedicineNederlands Tijdschrift Voor Geneeskunde 1999 143(43):2150-53. [Google Scholar]
[17]. Ehara S, Takahashi K, Reasons for Rejection of Manuscripts Submitted to AJR by international AuthorsAJR 2007 188(2):W113-16. [Google Scholar]
[18]. Dewan P, Gupta P, Shah D, Fate of Articles rejected by Indian PediatricsIndian Pediatrics 2010 47:1031-35. [Google Scholar]
[19]. McDonald RJ, Cloft HJ, Kallmes DF, Fate of submitted Manuscript Rejected from the American Journal of Neuroradiology : Outcomes and commentaryAm J Neuroradiol 2007 28:1430-34. [Google Scholar]
[20]. Proveenzale JM, Revising a Manuscript: Ten Principles to Guide Success for PublicationAJR 2010 198:W382-83. [Google Scholar]
[21]. Ali J, Manuscript rejection: Causes and RemediesJ Young Pharm 2010 2(1):3-6. [Google Scholar]
[22]. Eleven Reasons why Manuscripts are Rejected. San Francisico Edit. http://www.sfedit.net/rejection.pdf [Google Scholar]
[23]. Michel R, Plagiarism in the Medical/scientific LiteratureJournal of Cardiovascular Pharmacology 2010 56(6):709 [Google Scholar]
[24]. Bazdaric K, Plagiarism detection- quality management tool for all scientific journalsCroat Med J 2012 53:1-3. [Google Scholar]
[25]. Bazdaric K, Bilic-Zulle L, Brumini G, Petrovecki M, Prevalance of plagiarism in recent submission to Croatian medical journalSci. Eng. Ethics 2012 18(2):223-39. [Google Scholar]
[26]. Castillo M, Cross-Checking for plagiarismAJNR 2008 29:1035 [Google Scholar]
[27]. Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals. Published by ICMJE, 2013 Update. http://www.icmje.org/icmje-recommendations.pdf [Google Scholar]
[28]. COPE. COPE flowchart. 2006. Available from: http://publicationethics.org/files/u7140/Full%20set%20of%20flowcharts.pdf. Assessed: March10,2015 [Google Scholar]
[29]. Rathore FA, Farooq F, Plagiarism detection softwares: Useful tools for medical writers and editorsJ Pak Med Assoc 2014 64(11):1329-30. [Google Scholar]
[30]. Plagiarism detection. http://www.elsevier.com/editors/perk/plagiarism-detection [Google Scholar]
[31]. Rao SA, Singh N, Kumar R, Thomas AM, More than meets the eye: Digital fraud in dentistryJISPPD 2010 28(4):241-44. [Google Scholar]