Bacteriological Quality of Treated Water and Dialysate in Haemodialysis Unit of A Tertiary Care Hospital
Shiva Verma1, V A Indumathi2, K C Gurudev3, Shalini Ashok Naik4
1 Post Graduate, Department of Microbiology, M.S. Ramaiah Medical College, Bangalore, Karnataka, India.
2 Professor, Department of Microbiology, M.S. Ramaiah Medical College, Bangalore, Karnataka, India.
3 Professor, Department of Nephrology, M.S. Ramaiah Medical College, Bangalore, Karnataka, India.
4 Associate Professor, Department of Microbiology, M.S. Ramaiah Medical College, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shiva Verma, Post Graduate, Department of Microbiology, M.S. Ramaiah Medical College, Bangalore-560054, Karnataka, India.
E-mail: drshivaverma@gmail.com
Introduction
Haemodialysis is one of the treatment modalities for patients suffering from end stage renal disease (ESRD). Dialysis patients are exposed to large volumes of water for production of dialysis fluids. Treated water and dialysate come in direct contact with the patient’s bloodstream. Such patients suffer from abnormalities of the immune system, making them more susceptible to infections. Microbial contamination of the treated water and dialysate can lead to biofilm formation and release of endotoxins in Haemodialysis system. These can give rise to pyrogenic reactions in the short term and β2 amyloidosis, atherosclerosis, and increased mortality in the long term.
Aim
To assess the bacteriological quality of treated water and dialysate used in the Haemodialysis unit of a tertiary care hospital.
Materials and Methods
A retrospective review of records of treated water and dialysate samples sent to the Microbiology laboratory for analysis of bacteriological contamination of the water used in haemodialysis treatment from January 2013 to June 2014 was conducted. The acceptable limits for treated water and dialysate were taken as <200 CFU/ml and < 2000 CFU/ml respectively as per Government of India Guidelines for Maintenance Haemodialysis.
Results
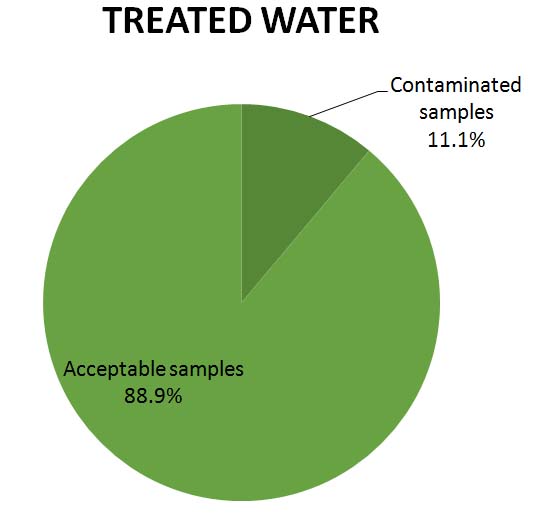
Thirty six samples of treated water and 394 samples of dialysate were analysed for bacteriological contamination. 4 out of 36 (11.1%) samples of treated water and 44 out of 394 dialysate samples (11.2%) showed unacceptable bacteriological growth.
Conclusion
Regular and continual monitoring of the disinfection protocol of the water distribution system in haemodialysis unit is necessary to get good microbiological quality of treated water and dialysate fluid.
Dialysis fluid quality, Microbiological contamination, Water treatment
Introduction
The burden of End stage kidney disease is on the rise worldwide with about 100,000 new patients developing this disease in India every year [1,2]. With the kidney donor programme still in its primitive stage and the associated financial constraints, most of the patients in India live on maintenance dialysis [3]. It is estimated that the population requiring dialysis is growing at the rate of 10–20% annually with only 16.3% being able to afford it [1,2]. This is just the tip of the iceberg because no national registries exist in our country.
Patients undergoing dialysis are exposed to large volumes of water (~ 400 litres/week) for production of dialysis fluids [4]. Treated water and dialysate come in direct contact with the patient’s bloodstream. Such patients, because of uremia and its related metabolic consequences, have a debilitated immune system. The situation is potentially aggravated by the lack of protective barrier of the gastrointestinal tract and detoxification by kidneys, which places them at a higher risk of acquiring infections [5,6].
Microbial contamination of water can lead to biofilm formation in Haemodialysis (HD) system and release of endotoxins. Biofilm once formed is difficult to remove inspite of regular disinfection and is the constant source of endotoxins, peptidogycans and fragments of bacterial DNA that can cross the dialyser membrane and stimulate cytokine production and trigger elevation of acute phase reactants. These can give rise to acute intradialytic complications like fever, chills, hypotension, headache, nausea, cramps [5]. Studies also suggest evidence of a possible relationship between water contamination and long-term morbidity, β2 amyloidosis, atherosclerosis [6,7].
Microbial quality of dialysis fluids is still too often a neglected problem. It is critical to monitor the bacteriological quality of dialysis water. Good quality water can help improve patient’s quality of life and could possibly increase their survival rates [8,9].
Aim
The aim of this retrospective study is to assess the bacteriological quality of treated water and dialysate used in the Haemodialysis unit of M.S. Ramaiah Hospital, Bangalore.
Materials and Methods
The study was conducted in M.S. Ramaiah Hospital, Bangalore. A retrospective review of records of treated water and dialysate samples sent to the Microbiology laboratory for analysis of bacteriological contamination of the water used in haemodialysis treatment from January 2013 to June 2014 was conducted. Total number of 36 treated water samples and 394 Dialysate samples were analysed during this period.
Sample collection: Treated water samples were collected immediately past the water purification system (Reverse Osmosis) water tank and from Reverse Osmosis (RO) lines supplying the HD unit. Dialysate samples were taken from each haemodialysis machine where dialysate exits the dialyzer in the HD unit. The sample ports were disinfected with alcohol and allowed to dry before collecting the samples. At each point of collection, the valve was opened and water allowed to flow for a minimum of 2 minutes at normal pressure and flow rate before the samples were drawn. Samples were collected using a “clean catch” technique to minimize potential contamination of the sample [3].
Sample processing: Mueller Hinton Agar plates (150mm diameter) were used. The samples were mixed by vortexing. 0.1ml of treated water samples were pipetted and placed on the centre of the plate. Dialysate samples were inoculated onto separate Mueller Hinton Agar plates using 1μl calibrated loop. The sample was spread with a cool alcohol flamed glass rod spreader onto the plate. The plates were incubated at 350C for 48 hrs [3].
Interpretation: For treated water, the colony count/ml was determined by multiplying the number of colonies seen by 10. The number of colonies seen was multiplied by 1000 to get the colony count per ml of dialysate sample.
The acceptable limits of bacterial contamination for Treated water and Dialysate were taken as less than 200 CFU/ml and less than 2000 CFU/ml respectively in accordance with the Govt of India guidelines for Haemodialysis [3].
Results
4 out of 36 (11.1%) of Treated water and 44 out of 394 (11.2%) dialysate samples showed growth above acceptable limits of bacterial contamination [Table/Fig-1,2].

In cases of samples showing unacceptable levels of bacterial contamination, disinfection of the water treatment system was repeated and follow-up cultures done until samples showed growth within acceptable limits.
Discussion
The results of our study were found to be in the same range as other similar studies [8,10–13]. In a cross-sectional survey done across 51 chronic and acute dialysis centres in the central United States, 35.3% of the water samples and 19% of the dialysate samples did not satisfy the AAMI guidelines [10]. A study done in Germany observed that 17.8% of all water samples and 11.7% of all dialysate samples showed contamination higher than the accepted standard values [11]. Study conducted by Asserraji et al., in Saudi Arabia found the incidence of unacceptable bacterial contamination of treated water to be 9.2% while dialysate samples did not show any contamination. They suggested that frequent disinfection of the water treatment plant is required to get better quality water for production of dialysis fluids [12].
In a similar study done by El-Koraie et al., out of 321 samples taken from different points in the water distribution system and the dialysate sampling system, 16.8% samples showed unacceptable growth. They concluded that HD centres need regular monitoring and maintenance to provide good quality haemodialysis [13]. Various studies have also suggested incorporation of endotoxin assays to monitor the quality of water used for production of dialysis fluids [7,13–15].
In a survey done by the Japanese Society for Dialysis Therapy (JSDT) on bacteriological quality of dialysis fluid in all the dialysis facilities in Japan, 3.9% and 2.6% samples were found to be outside acceptable limits in 2006 and 2007 respectively. They found that the survival rate in dialysis patients in Japan was very high as compared to those of the other countries. The good quality of water and dialysate used in their dialysis facilities was suggested as one of the probable reasons for decreased rates of mortality in their patients [8].
Results of few studies similar to the present study are depicted in [Table/Fig-3].
Comparison with other similar studies
| Study By | Unacceptable Samples |
|---|
| Treated Water (%) | Dialysate (%) |
|---|
| Klein et al., [10] | 35.3 | 19 |
| Bambauer et al., [11] | 17.8 | 11.7 |
| Asserraji et al., [12] | 9.2 | Nil |
| Present study | 11.1 | 11.2 |
Different guidelines suggest different reference values as acceptable limits of contamination. The AAMI guidelines recommend <200 CFU/ml of treated water and <2000 CFU/ml of dialysate as permissible limits of contamination. The European Pharmacopoeia is more stringent, with growth ≥ 100 CFU/ml each of dialysate and treated water considered as unacceptable [3].
This study highlights the importance of regular monitoring of quality of water used in HD units. Compliance could be increased further by frequent disinfection of the HD system. It is necessary to upgrade the disinfection protocols of the HD system. Further studies need to be done to identify the causes of contamination. Other options of disinfection of the water systems can be explored.
Limitations
Endotoxin assays could not be done due to financial constraints as this stays the limitation of our study.
Conclusion
The quality of dialysis water depends on microbial contamination of untreated water, water purification techniques used and maintenance of water treatment and distribution systems. It is necessary to regularly monitor the quality of water used in HD units. Also, adoption and strict implementation of standard disinfection protocols of the water distribution and HD system is required to obtain good quality of water to minimize exposure of these immunodeficient patients to contaminated sources of water.
[1]. Sakhuja V, Sud K, End-stage renal disease in India and Pakistan: burden of disease and management issuesKidney Inter Suppl 2003 83(2):S115-18. [Google Scholar]
[2]. Jha V, Current status of end-stage renal disease care in India and PakistanKidney Inter Suppl 2013 3(2):S157-60. [Google Scholar]
[3]. Guidelines for Maintenance Hemodialysis in IndiaMinistry of Health & Family Welfare Govt. of IndiaInd J Nephrol 2012 Suppl:S1-46. [Google Scholar]
[4]. Pontoriero G, Pozzoni P, Andrulli S, Locatelli F, The quality of dialysis waterNephrol Dial Transplant 2003 18(Suppl):vii:21-25. [Google Scholar]
[5]. Perez-Garcia R, Cinio Rodriquez-Benitez PO, Why and how to monitor bacterial contamination of dialysate? Nephrol DialTransplant 2000 15(6):760-65. [Google Scholar]
[6]. Montanari LB, Sartori FG, Cardoso MJ, Microbiological contamination of a haemodialysis center water distribution systemRev Inst Med Trop Sao Paulo 2009 51(1):37-43. [Google Scholar]
[7]. Lonnemann G, The quality of dialysate: An integrated approachKidney International 2000 58(76):S112-19. [Google Scholar]
[8]. Masakane I, Takemoto Y, Nakai S, Bacteriological water quality in the central dialysis fluid delivery system from the survey of the Japanese Society for Dialysis TherapyBlood Purif 2009 27(Suppl 1):11-16. [Google Scholar]
[9]. Oumokhtar B, Lalami AEO, Mahmoud M, Prevent infection linked to the dialysis water in a hemodialysis center in Fez city (Morocco)The Pan African Medical Journal 2013 16(11):122 [Google Scholar]
[10]. Klein E, Pass T, Harding GB, Wright R, Million C, Microbial and endotoxin contamination in water and dialysate in the central United StatesArtif Organs 1990 14(2):85-94. [Google Scholar]
[11]. Bambauer R, Schauer M, Jung WK, Daum V, Vienken J, Contamination of dialysis water and dialysate: A survey of 30 centersASAIO J 1994 40(4):1012-16. [Google Scholar]
[12]. Asserraji M, Maoujoud A, Belarbi M, Elfarouki R, Monitoring the microbiological quality of dialysate and treated waterSaudi J Kidney Dis Transpl 2014 25(1):91-95. [Google Scholar]
[13]. El-Koraie AF, Hazzah WA, Abbass AA, El-Shazly SA, Bacteriological monitoring of dialysis fluid in 2 hemodialysis units in Alexandria, EgyptSaudi Med J 2007 28(8):1234-38. [Google Scholar]
[14]. Lima JRO, Marques SG, Gonçalves AG, Microbiological analyses of water from hemodialysis services in São Luís, Maranhão, BrazilBraz. J. Microbiol 2005 36:103-08. [Google Scholar]
[15]. Hoenich NA, Levin R, The implications of water quality in hemodialysisSemin Dial 2003 16(6):492-97. [Google Scholar]