Among the patients attending the Emergency Department, chest pain is one of the most common and important complaints. Apart from AMI, gastro-oesophageal, musculo-skeletal and pulmonary disorders are the other common causes of chest pain [1]. AMI accounts for 5-15% of all the causes of chest pain in USA. In countries like India, considerably higher number of patients present with chest pain as the chief complaint to the emergency department [2]. By accurately ruling out chest pain of cardiac origin, 40% of patients presenting with acute chest pain could be spared from the risks and costs of unnecessary hospital admission and more invasive cardiac testing [3]. Early accurate diagnosis and treatment of acute myocardial infarction (AMI) can reduce the mortality and associated long term morbidity. Majority of deaths due to AMI occur during the first hour after the onset of symptoms. If AMI cases are diagnosed and treated effectively during the first hour (so called Golden Hour) after the onset of symptoms, the mortality can be reduced from 9% to 3%, but if delayed for 3-4 hours mortality can be 5 times higher [4].
However, there are no reliable tests for the diagnosis of AMI in the early hours after the onset of symptoms. Electrocardiographic (ECG) ST elevation has only 50-60% sensitivity for the diagnosis of myocardial necrosis [5]. Currently creatine kinase–MB isoenzyme (CK-MB), myoglobin and cardiac troponins (cTnI & cTnT) are used in the diagnosis of AMI. However, these cardiac marker proteins are also not satisfactory for the diagnosis of AMI within first 6 hours of the onset of chest pain. Myoglobin which appears in the blood within 2 hours after myocardial infarction, lacks specificity because myoglobin released from skeletal muscles cannot be distinguished from that released from heart. Cardiac troponins and CK-MB though more specific for cardiac injury, lack early sensitivity because their blood concentrations do not rise until 6-8 hours after the onset of symptoms [6].
Heart-type fatty acid binding protein (H-FABP) is a novel marker with the potential for the early diagnosis of AMI within 6 hours of onset of symptoms. It offers several theoretical advantages over traditional cardiac bio-markers. H-FABP is a 15 kDa soluble protein, consisting of 132 amino acids. It is one of the most abundant proteins in the cardio myocytes comprising 5-15% of the total cytosolic protein pool. It is involved in the delivery of fatty acyl coenzyme A for oxidation in the mitochondria. Under normal conditions H-FABP is not present in plasma. During ischemia, H-FABP leaks out of myocardial tissue and the concentration increases in the blood within 2 hours and is reported to peak at about 4-6 hours and return to normal baseline value in 20 hours [7].
In view of above observations, we compared the diagnostic value of H-FABP with CK-MB and myoglobin within 6 hours after the onset of symptoms. The objective of the study was to compare the sensitivity, specificity, positive predictive value, negative predictive value and area under ROC curve of H-FABP with those of myoglobin and CK-MB within 0-3 hours and 3-6 hours after the onset of chest pain.
Materials and Methods
The study was carried out at BLDEU’s Shri B M Patil Medical College, Hospital and Research Centre, Vijayapur, Karnataka, India during the period from May 2013 to June 2014. The study was approved by the Institutional Ethical Clearance Committee (IECC) and informed consent was obtained from all the study participants before their inclusion in the study. Also the procedures followed were in accordance with the Helsinki Declaration of 1975 that was revised in 2000.
The study included 40 AMI cases and 40 non cardiac chest pain but otherwise healthy controls. Both cases and controls were further divided into two groups as those reporting within 3 hours and those between 3-6 hours after the onset of chest pain. As a part of routine assessment in our institution each patient underwent an initial clinical and laboratory evaluation, which included the detailed clinical history, clinical examination, standard 12 lead ECG, chest X-ray, routine blood investigations, echocardiography and cardiac biomarkers (CK-MB and cardiac troponin I). Diagnosis of either MI or non-cardiac chest pain was made after critical review of all the above information by a cardiologist. Patients arriving to hospital after 6 hours of onset of chest pain, those with Chronic muscle disease, renal disease, recent surgery, those receiving direct current shocks and who underwent PTCA or CABG procedures within 30 days were excluded from the study.
From all the cases and controls, 5 ml of venous blood sample was drawn as early as possible after admission using all the aseptic precautions, serum was separated and kept at -200C until the analysis was done. Serum troponin-I [8] and myoglobin [9] levels were measured by chemiluminescence immunoassay on Abbott Architect c4000 analyser (Abbott Laboratories, Illinois, USA) and serum CK-MB by Immuno-inhibition method [10,11] using Stat Fax 3300 Biochemistry analyser (Awareness Technology Inc., Florida, USA). Serum H-FABP levels were measured by Automated Immuno-turbidimetric method [12,13] (Reagent kit from Randox Laboratories, and using Roche C-311 fully automated Biochemistry analyser). The method is based on the principle that, H-FABP present in the sample reacts with buffer and anti-H-FABP coated latex. The formation of antigen-antibody complex during the reaction results in an increase in turbidity, the extent of which is measured as the amount of light absorbed at 700 nm. By constructing a standard curve from the absorbance of the standards, H-FABP concentration in the sample can be determined. The cut off levels and coefficients of variation (CV) of H-FABP, troponin-I, myoglobin and CK-MB used for the diagnosis of AMI in this study were >6.32ng/ml (at 99th percentile & CV = 7.94%), >0.032 μg/L in males & >0.022 μg/L in females (at 99th percentile & CV = 10%), >106 ng/ml in males & >155 ng/ml in females (at 99th percentile & CV = 7.94%) and 24 IU/L respectively. These values are according to the recommendations of the reagent kit manufacturers [8–13].
Statistical Analysis
Data is presented as mean ± SD values. Differences between means of two groups were assessed by Student t-test. Sensitivity, specificity, positive and negative predictive values were calculated and Receiver operating characteristic (ROC) curve analysis was done to assess the diagnostic accuracy of each study parameter. For all the tests, p-value of 0.05 or less is considered for statistical significance.
Baseline clinical characteristics of AMI cases and controls
| SI No. | Clinical characteristic | AMI cases(n = 40) | Controls(n = 40) |
|---|
| 01 | Age (Years) (Mean ± SD) | 60.5 ± 12.8 | 54.8 ± 15.2 |
| 02 | Males | 28 (70%) | 27 (67.5%) |
| 03 | Females | 12 (30%) | 13 (32.5%) |
| 04 | Smoking | 12 (30%) | 11 (27.5%) |
| 05 | Alcohol intake | 11 (27.5%) | 11 (27.5%) |
| 06 | Hypertension | 17 (42.5%) | 10 (25%) |
| 07 | Diabetes Mellitus | 13 (32.5%) | 10 (25%) |
| 08 | Hyperlipidemia | 06 (15%) | 03 (7.5%) |
| 09 | H/o previous IHD | 02 (5%) | 00 |
| 10 | ECG changes • ST Elevation • T- wave inversion • Other changes (STdepression/ Tall T waves/Q wave) | 33 (82.5%)07 (17.5%)07 (17.5%) | —05 (8.3%)03 (5%) |
| 11 | Troponin I (μg/L) (Mean ± SD) | 7.57 ± 16.9 | 0.0065 ± 0.008 |
Results
A total of 80 patients were included in this study. Of these 40 were AMI cases and 40 were non cardiac chest pain otherwise healthy controls. Of 40 AMI cases 28 were males and 12 females and of 40 controls 27 were males and 13 females. The average age for the AMI cases was 60.45 years and that in controls was 54.83 years. [Table/Fig-2] shows the mean levels of four cardiac biomarkers in AMI cases and controls. The mean levels of H-FABP, myoglobin, troponin I and CK-MB activity were significantly higher in AMI cases when compared to that of controls in both 0-3 hour and 3-6 hour groups. In both the groups, the difference was statistically significant (p < 0.01). [Table/Fig-3] shows the sensitivity, specificity, positive and negative predictive values of H-FABP were greater than CK-MB and myoglobin in both 0-3 hour and 3-6 hour groups. The diagnostic ability of each marker to distinguish between AMI and non-AMI groups was assessed by receiver operating characteristic curve (ROC) analysis. The area under the curve (AUC) of H-FABP was higher than CK-MB and myoglobin in both 0-3 hour group and 3-6 hour groups [Table/Fig-4,5,6 and 7].
Mean levels of four cardiac biomarkers in cases and controls
| AMI cases(Mean ± SD) | Controls(Mean ± SD) | p1 value | p2 value |
|---|
| 0-3 h(n = 17) | 3-6 h(n = 23) | 0-3 h(n = 17) | 3-6 h(n = 23) |
|---|
| CK-MB(IU/L) | 40.9 ± 22.6 | 74.9 ± 58.4 | 19 ± 10.04 | 25.2 ± 10.1 | < 0.01 | < 0.01 |
| Myoglobin(ng/mL) | 320.1 ± 344.7 | 439.9 ± 396.7 | 60.96 ± 57.7 | 87.1 ± 75.4 | < 0.01 | < 0.01 |
| H-FABP(ng/mL) | 31.9 ± 51.7 | 66.4 ± 58.1 | 5.28 ± 8.5 | 5.9 ± 7.8 | < 0.01 | < 0.01 |
| Troponin I(μg/L) | 10.4 ± 16.5 | 12.4 ± 17.5 | 0.005 ± 0.008 | 0.008 ± 0.008 | < 0.01 | < 0.01 |
p1 = AMI cases (0-3 hours group) versus Controls (0-3 hours group)
p2 = AMI cases (3-6 hours group) versus Controls (3-6 hours group)
Sensitivity, specificity, PPV and NPV of CK-MB, myoglobin and H-FABP in 0-3 hour and 3-6 hour groups after the onset of chest pain
| Sensitivity | Specificity | PPV | NPV |
|---|
| 0-3 h | 3-6 h | 0-3 h | 3-6 h | 0-3 h | 3-6 h | 0-3 h | 3-6 h |
|---|
| CK-MB(IU/L) | 23.5 | 60.9 | 58.8 | 56.5 | 36.4 | 58.3 | 43.5 | 59.1 |
| Myoglobin(ng/mL) | 70.6 | 87 | 76.5 | 69.6 | 75 | 74 | 72.2 | 84.2 |
| H-FABP(ng/mL) | 94.1 | 91.3 | 88.2 | 73.9 | 88.9 | 77.8 | 93.8 | 89.5 |
PPV = Positive Predictive Value; NPV = Negative Predictive Value
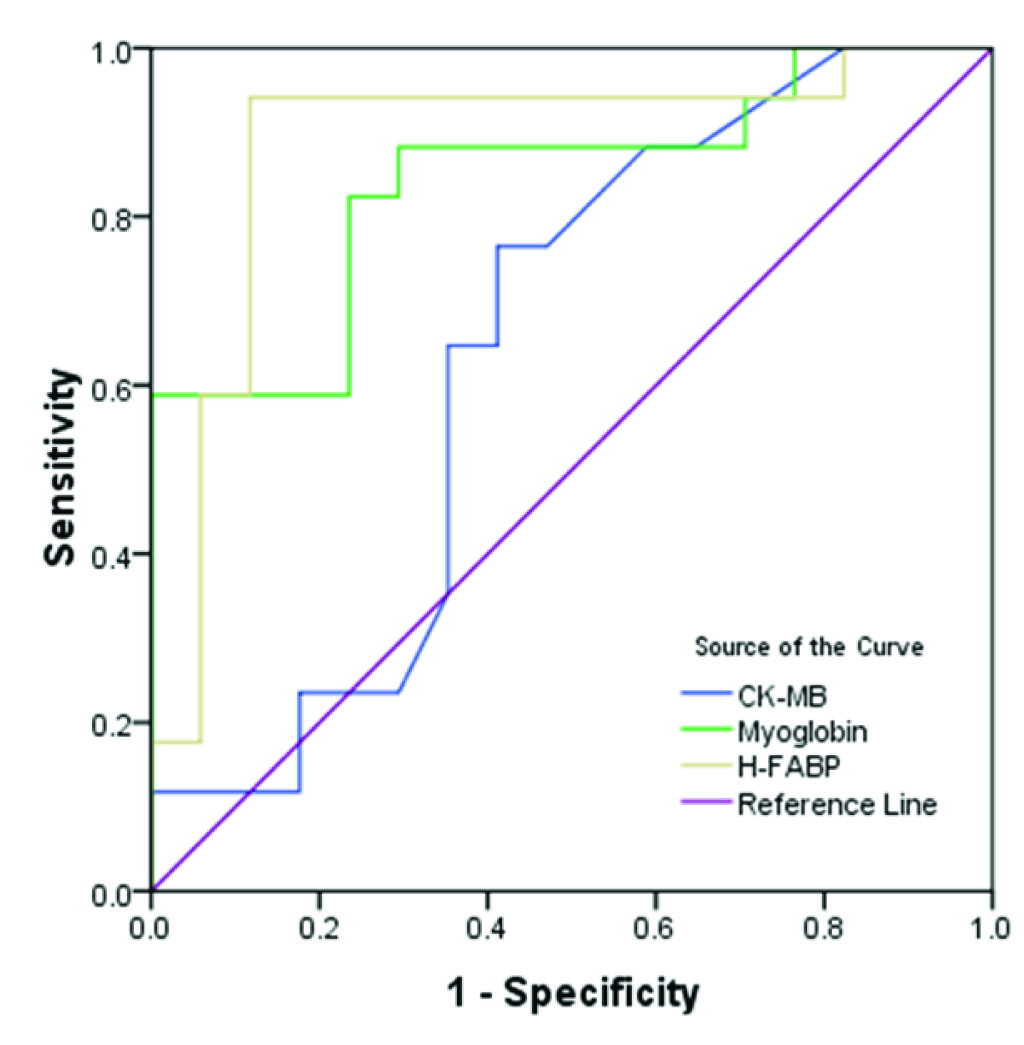
ROC curve analysis of CK-MB, Myoglobin & H-FABP in 0-3 hour group
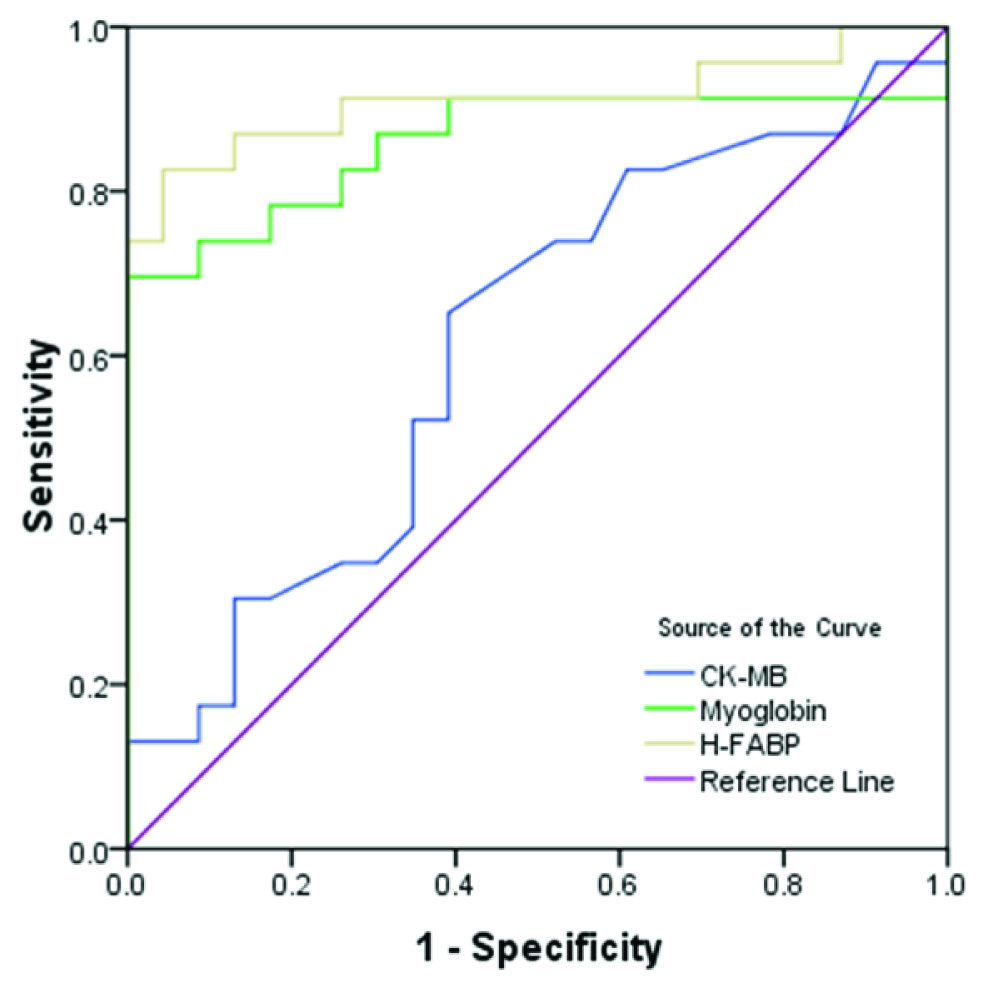
ROC curve analysis of CK-MB, Myoglobin & H-FABP in 3-6 hour group
Area under ROC curve for cardiac markers in 0-3 hour group
| AUC | p-value | Confidence Interval |
|---|
| Lower limit | Upper limit |
|---|
| CK-MB | 0.640 | 0.163 | 0.446 | 0.834 |
| Myoglobin | 0.841 | 0.001 | 0.705 | 0.977 |
| H-FABP | 0.886 | 0.000 | 0.756 | 1.015 |
AUC = Area under curve
Area under ROC curve for cardiac markers in 3-6 hour group
| AUC | p-value | Confidence Interval |
|---|
| Lower limit | Upper limit |
|---|
| CK-MB | 0.616 | 0.177 | 0.452 | 0.781 |
| Myoglobin | 0.860 | 0.000 | 0.738 | 0.983 |
| H-FABP | 0.911 | 0.000 | 0.816 | 1.007 |
AUC = Area under curve
Discussion
Acute myocardial infarction is the major cause of mortality and long term morbidity in the modern world. Early and correct diagnosis is of utmost importance to enable the immediate and intensified treatment which consequently reduces the mortality [14]. The golden time for the optimal outcome of coronary revascularization is within 4 hours after the onset of coronary thrombosis [15]. Cardiac troponins, CK-MB and myoglobin assays are the most commonly used cardiac markers for the detection of AMI [16]. Collisson et al., showed that, diagnosis of AMI cannot be made solely on the basis of either CK-MB or troponin I individual test results [17]. Yamamoto et al., demonstrated that, rapid quatitative test for cTnT and myoglobin at 6, 12, 24, 48 hours after onset of symptoms is useful for the early diagnosis and assessment of severity in AMI [18]. To date, myoglobin is the only cardiac biomarker used for the diagnosis of AMI in hyperacute phase (within 3 hours after the onset of symptoms). However, myoglobin is not a specific marker as its concentration is much higher in skeletal muscles than cardiac tissue [19].
In the present study, the incidence of myocardial infarction was more common in males, smokers, and those having hypertension, diabetes and hyperlipidemia. The reason being the above mentioned factors are the known risk factors for coronary heart disease [20]. In cases diagnosed with AMI, only 83.5% of the patients were having ECG changes and among the control group, 8.3% of the patients with non-cardiac chest pain presented with ECG changes suggestive of AMI. The diagnostic value of the admission ECG is limited in following situations; i) The presence of conduction disorders including left bundle branch block (LBBB); ii) If Q waves and ST-T changes are already present e.g. old infarcts and digoxin effects, respectively; iii) ST-T wave changes of marked left ventricular hypertrophy; iv) In posterior infarct or right ventricular infarct. 30% of patients may have no diagnostic changes on their admission ECG [7].
In our study, mean serum concentrations of HFABP, myoglobin and CK-MB activity were significantly higher (p< 0.01) in AMI cases when compared to controls both in 0-3 hour and 3-6 hour groups [Table/Fig-2]. Also, the mean levels of cardiac markers were much higher in 3-6 hour group when compared to 0-3 hour group of AMI cases. This finding is in full agreement with the studies conducted by Glatz JFC et al., Elmadbouh I et al., Pasaoglu H et al., and Orak M et al., [21–24].
In this study, H-FABP demonstrated highest sensitivity, specificity, PPV and NPV followed by myoglobin and CK-MB in patients with suspected AMI both within 3 hours and 3-6 hours after the onset of chest pain [Table/Fig-3]. This finding emphasizes two important facts: High sensitivity is essential for the early ‘rule in’ of AMI patients and high NPV is important for the early ‘rule out’ of AMI. Since more than 90% of patients who present with acute chest pain to an emergency department do not have AMI, H-FABP can prevent unnecessary admissions or inadvertent discharge of patients suspected for AMI.
Many studies have compared the diagnostic efficiency of H-FABP with the two routinely used cardiac markers CK-MB and myoglobin in the early diagnosis of AMI and arrived at nearly consistent results. In their study, Glatz JFC et al., found H-FABP having greater diagnostic sensitivity (73% at 1.5-3 hour and 100% at 4.5-6 hours) than myoglobin and CK-MB in the early diagnosis of AMI [21]. Elmadbouh I et al., found that within 3 hours, H-FABP had diagnostic sensitivity (81.8%) equal to that of CK-MB [22]. However, H-FABP had higher specificity (88.2%) equal to that of myoglobin but superior to that of CK-MB. This trend extends to within 6 hours as well. H-FABP had highest PPV (81.8%) and NPV (88.2%) [12]. Pasaoglu H et al., demonstrated that at 1-2, 3 and 6 hours after the onset of AMI, the diagnostic sensitivity and specificity of H-FABP were higher than CK-MB but similar to myoglobin [23]. In another study Orat M et al., showed that, for patients admitted with chest pain, HFABP is more sensitive and specific than CK-MB in the early diagnosis of ACS [24]. In patients with ACS who were admitted within 0 to 3 hours, the H-FABP sensitivity was 100% and specificity was 75%; and for CK-MB, the sensitivity was 81% and the specificity was 16%. In patients with ACS who were admitted within 3 to 6 hours, the H-FABP sensitivity was 97% and specificity was 68%; and for CK-MB, the sensitivity was 90% and specificity was 80% [14]. Alhadi H et al., conducted a study in 100 consecutive patients admitted with acute chest pain suggestive of ACS and found that, H-FABP peak concentration occurred at 8 hours after symptoms onset and was the most sensitive early marker with 79.9%, 98% and 95.3% sensitivity at presentation, 2 hours and 4 hours after presentation respectively [25]. The sensitivity of all other cardiac markers (CK-MB mass and myoglobin) was <62% at presentation. The negative predictive value of H-FABP was also superior to other markers. Myoglobin was the second most sensitive early marker at presentation. McMahon CG et al., concluded that, of the four biomarkers measured, H-FABP demonstrated highest sensitivity (64.3% at 0-3 hours and 85.3% at 3-6 hours) and NPV (93% at 0-3 hours and 97% at 3-6 hours) at the early time points [26].
Diagnostic ability of each cardiac marker for 0-3 hours and 3-6 hours groups were examined by ROC curve analysis. In both the groups, H-FABP had the highest area under curve followed by myoglobin and CK-MB [Table/Fig-4,5]. The AUC values of these markers in both the groups were statistically significant (p < 0.05) except for CK-MB [Table/Fig-6,7]. This finding is in agreement with the studies conducted by Elmadbouh I et al., Pasaoglu H et al., Orak M et al., McMahon CG et al., and Kim KS et al., [22–24,26,27].
The observed better diagnostic value of H-FABP than myoglobin and CK-MB in AMI is probably because of its early rise in the serum concentration which in turn is related to the smaller molecular size (15kDa and 17 kDa for H-FABP and myoglobin respectively), higher concentration in the myocardial tissue (Concentration of myoglobin is approximately 2 fold lower in cardiac than skeletal muscle but H-FABP concentrations are 2-10 fold higher in heart than in skeletal muscle) and very low plasma concentration under normal conditions (< 5 μg/l; The ratio of cytoplasmic to vascular concentration is 200000:1, which is 10-15 fold lower than myoglobin). Even though H-FABP is not completely cardiac specific, its tissue distribution outside the heart is comparable to that of CK-MB [7]. CK-MB has low sensitivity because it takes atleast 4-6 hours after the onset of myocardial injury to appear in the blood. Due to outstanding diagnostic performance of cardiac troponins, H-FABP is likely to play a role only in the early presentation after the symptom onset.
Limitations for the clinical use of H-FABP concentration in the early diagnosis of AMI includes: Increase in the concentration of H-FABP may be seen in conditions of skeletal muscle injury (e.g. intramuscular injections, electric cardioversion, traumatic cardiopulmonary resuscitation, surgery, crush injury, etc.) as the FABP from skeletal muscle origin is identical to that of cardiac origin. Also, renal insufficiency can result in the elevation of H-FABP level because it is excreted thoursough the kidney [7].
Limitations
Our study presents few limitations such as small sample size and we could not do the serial measurements of the cardiac markers for the assessment of their kinetics.
Conclusion
H-FABP is more sensitive and specific cardiac biomarker than myoglobin and CK-MB and shows better diagnostic efficiency for the early diagnosis of myocardial infarction within 6 hours of chest pain. H-FABP can be used as an additional diagnostic tool for the early diagnosis of acute myocardial infarction.
p1 = AMI cases (0-3 hours group) versus Controls (0-3 hours group)
p2 = AMI cases (3-6 hours group) versus Controls (3-6 hours group)
PPV = Positive Predictive Value; NPV = Negative Predictive Value
AUC = Area under curve
AUC = Area under curve